
A Population-Based Twin Study of the Relationship Between Neuroticism and Internalizing Disorders
Abstract
Objective: The anxiety and depressive disorders exhibit high levels of lifetime comorbidity with one another. The authors examined how genetic and environmental factors shared by the personality trait neuroticism and seven internalizing disorders may help explain this comorbidity. Method: Lifetime major depression, generalized anxiety disorder, panic disorder, agoraphobia, social phobia, animal phobia, situational phobia, and neuroticism were assessed in over 9,000 twins from male-male, female-female, and opposite-sex pairs through structured diagnostic interviews. Multivariate structural equation models were used to decompose the correlations between these phenotypes into genetic and environmental components, allowing for sex-specific factors. Results: Genetic factors shared with neuroticism accounted for between one-third and one-half of the genetic risk across the internalizing disorders. When nonsignificant gender differences were removed from the models, the genetic correlations between neuroticism and each disorder were high, while individual-specific environmental correlations were substantially lower. In addition, the authors could identify a neuroticism-independent genetic factor that significantly increased risk for major depression, generalized anxiety disorder, and panic disorder. Conclusions: There is substantial, but not complete, overlap between the genetic factors that influence individual variation in neuroticism and those that increase liability across the internalizing disorders, helping to explain the high rates of comorbidity among the latter. This may have important implications for identifying the susceptibility genes for these conditions.
The existence of high rates of comorbidity among the internalizing (i.e., anxiety and depressive) disorders is well established (1) . Studies have consistently demonstrated associations between high levels of neuroticism in individuals and increased likelihood that they suffer from one or another of these syndromes. A smaller number of studies have examined the role that neuroticism may play in explaining the comorbidity findings. Andrews et al. analyzed patterns of comorbid neurotic disorders and neuroticism scores in a subsample (N=892) of the Australian Twin Registry plus a clinical sample of 165 panic disorder patients and found that higher neuroticism scores predicted the number of internalizing disorders diagnosed in a subject (2) . In their examination of the relationship between the five-factor model of personality and comorbidity among phobic, panic, and depressive disorders, Bienvenu et al. showed not only that neuroticism was significantly associated with each disorder but also that it was the strongest predictor of comorbidity (3) . In an earlier analysis in the Virginia Adult Twin Study of Psychiatric and Substance Use Disorders, our group demonstrated that neuroticism accounted for a high proportion of phenotypic comorbidity across a range of internalizing disorders (4) .
Some studies have begun to examine the sources of correlation between neuroticism and anxiety and depressive symptoms and disorders. The authors of a report on one large population-based twin study that examined neuroticism and self-report symptoms of anxiety and depression concluded that genetic variation in these symptoms largely depends on the same factors as those affecting neuroticism (5) . Our group has extended these findings in two separate studies examining the genetic and environmental sources of covariation between neuroticism and major depression (6) and between neuroticism and generalized anxiety disorder (7) . Each of those analyses showed substantial genetic correlation between neuroticism and the respective psychiatric disorder.
In this study, we sought to answer several related questions. First, to what extent are the associations between levels of neuroticism and risk for each of the internalizing disorders explained by genetic versus environmental factors, i.e., what etiologic factors are behind the observed associations between neuroticism and the internalizing disorders? Second, to what extent do the genetic and environmental factors underlying neuroticism account for comorbidity among these disorders? Third, are there genetic and environmental factors independent of neuroticism that also contribute to their comorbidity?
Method
Sample and Assessment Procedures
The twins in this study derive from the population-based Virginia Adult Twin Study of Psychiatric and Substance Use Disorders (9) . Female-female twin pairs from birth years 1934–1974 became eligible if both members previously responded to a mailed questionnaire in 1987–1988, the response rate to which was about 64%. They were approached for four subsequent waves of personal interviews conducted between 1988 and 1997, with cooperation rates ranging from 85% to 92%. The male-male and male-female twin pairs, covering the birth years 1940–1974, were ascertained in a separate study—with an initial cooperation rate of 72%—and were approached for two waves of interviews from 1993 until 1998. Zygosity was determined by a combination of standard questions (8) , photographs, and DNA analysis (9) . The mean age of the female-female participants was 36.6 years (SD=8.1) at their final interview, and for the male-male and male-female subjects it was 36.8 years (SD=9.1). At each wave, the members of each twin pair were interviewed by different interviewers, who were blind to clinical information about the co-twin. Each interviewer had a master’s degree in a mental health-related field or a bachelor’s degree in this area plus 2 years of clinical experience.
Neuroticism was assessed by using the 12 items from the short form of the Eysenck Personality Questionnaire (10) in a self-report questionnaire. It was analyzed as an ordinal variable with scores from 0 to 12. We used DSM-III-R diagnostic criteria to assess lifetime major depression and modified DSM-III-R criteria for lifetime generalized anxiety disorder and panic disorder. Since their low prevalences had been problematic in previous analyses (11 , 12) , we adopted a broad diagnostic approach to these two disorders, reducing the minimum duration from 6 months to 1 month for generalized anxiety disorder and requiring a history of panic attacks meeting at least two criteria within 30 minutes for panic disorder. Phobia was diagnosed by using an adaptation of DSM-III criteria that required the presence of one or more fears, out of 22, that the respondent recognized as unreasonable and that, in the judgment of the interviewer, objectively interfered with the respondent’s life (13) . As we had to restrict our analyses to the simultaneous modeling of six phenotypes in order to keep computer run times tractable, we included agoraphobia and social phobia in one set of analyses and two specific phobias (animal and situational) in a second set.
The diagnostic data used in these analyses came from various waves of the two samples. In the female-female sample, all measures came from the fourth wave except for generalized anxiety disorder (wave 1) and panic disorder (wave 2). For the sample of male-male and male-female twins, all measures came from the second wave with the exception of major depression. The total number of complete pairs and singletons available for analysis differed slightly as a function of interview wave but were approximately as follows, by zygosity group: female-female monozygotic, 678 pairs and 65 singletons; female-female dizygotic, 467 pairs and 46 singletons; male-male monozygotic, 869 pairs and 230 singletons; male-male dizygotic, 653 pairs and 275 singletons; male-female dizygotic, 1,429 pairs and 462 singletons, giving a total of 9,270 twin subjects.
Statistical Analysis
We have outlined elsewhere our approach to multivariate genetic analysis (14 , 15) , which is designed to explain covariation and its sources (genetic and environmental) among multiple variables with a smaller set of higher-order factors. Using the software package Mx (16) , we fit liability-threshold models by the method of maximum likelihood to raw data from all individual twins, including those without an interviewed co-twin and subjects missing some of the outcome measures.
For these analyses, we used independent pathway models that contained two additive genetic common factors (A1, A2), two shared environmental common factors (C1, C2), and two unique environmental common factors (E1, E2) in addition to disorder-specific factors (A SP , C SP , E SP ). Common pathway models were initially tested and subsequently rejected because of poorer fit to the data. Two factors were used in a confirmatory strategy based on indications from analyses in this and other samples of a delineation of two clusters representing “anxiety-misery” and “fear” factors in the structure of the internalizing disorders (17 – 19) . However, for this analysis, we specified the first factor in each domain to account for all of the variance of neuroticism and the second factor to be independent of neuroticism. This represents our central hypothesis that the genetic and environmental factors underlying neuroticism are shared with the internalizing disorders and account for a portion of their associations, while there may also be other factors not shared with neuroticism that account for their remaining associations.
In first fitting this model, we allowed all the parameters, including thresholds, to vary by sex. In particular, we fit a sex-limitation model, which tests for both differences in magnitude of the effects of the same genetic risk factors between men and women as well as sex-specific risk factors. We then constrained all the path estimates (but not the thresholds) to be equal in the two sexes to test for these two types of sex differences. We did this for all of the path estimates en masse to test the global structural equivalence across genders rather than test each individual pathway.
Twice the difference in log-likelihood between the two models yields a statistic that is asymptotically distributed as chi-square with degrees of freedom equal to the difference in their number of parameters. We used Akaike’s information criterion (20) for model selection.
Results
Figure 1 depicts the path estimates for the full models in men and women that included agoraphobia and social phobia. Figure 2 depicts similar path estimates for animal and situational phobias. Although small differences were observed in both the effect size and sources of risk between men and women, when the parameter estimates were constrained to be equal across the sexes, this provided a slightly better overall model fit to the data by Akaike’s information criterion than when we retained sex differences. Paths that account for more than 5% of the variance in the phenotype (i.e., path loadings greater than √0.05, or 0.23) are depicted with thicker lines to provide a visual representation of the basic covariance structure. Comparing Figures 1 and 2 shows that substitution of the phobias produces small changes in the estimates for the path loadings on the other phenotypes but that the overall structure is preserved. The figures show that A1, the genetic factor for neuroticism, significantly affects all of the internalizing disorders, while A2, the common genetic factor independent of neuroticism, accounts for degrees of variance and covariance among major depression, generalized anxiety disorder, and panic disorder that are similar to those for the common genetic factor shared with neuroticism. Disorder-specific genetic factors (A SP ) are substantial for the phobias but not the other phenotypes in this model. The common (C1 and C2) and disorder-specific (C SP ) shared (familial) environmental factors have much smaller loadings, accounting for less than 5% of the variance for most of the measures except for panic disorder and situational and social phobias. The two common unique environmental factors (E1 and E2) vary in their effects, while disorder-specific environmental factors (E SP ) show substantial loadings across most disorders. We tested submodels to see if they would provide a more parsimonious explanation of the data, but we chose not to present them because of space limitations. Those results, which are consistent with the pattern of findings seen in the full models, are available on request. In particular, dropping the second genetic factor, A2, produced a significant deterioration in model fit by chi-square, indicating that including this neuroticism-independent source of genetic risk provides an improved fit to the data over the fit with A1 alone. Since the parameter estimates were similar for the phenotypes neuroticism, major depression, generalized anxiety disorder, and panic disorder estimated in both models, we took their average value across the two models to simplify their presentation or that of derivative measures in the following tables.
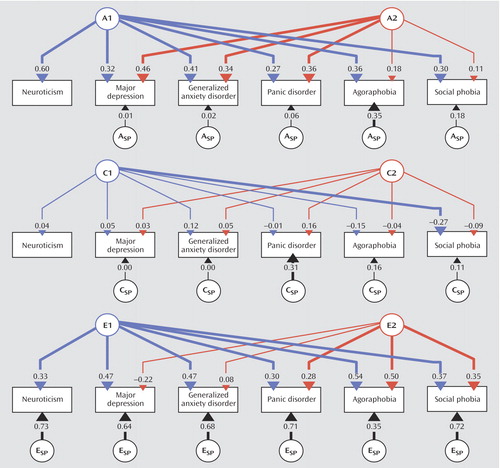
a The models contain six sets of latent factors (in circles)—two additive genetic common factors (A1, A2), two shared environmental common factors (C1, C2), two unique environmental common factors (E1, E2)—and disorder-specific factors (A SP , C SP , E SP ). The first common factors (A1, C1, E1) plus E SP account for all of the variance of neuroticism, while the second common factors (A2, C2, E2) are independent of neuroticism. Paths that account for more than 5% of the variance in a phenotype (i.e., path loadings greater than √0.05, or 0.23) are depicted with thicker lines for emphasis.
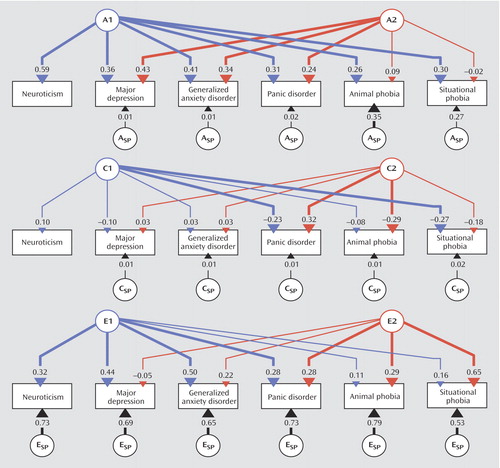
a The models contain six sets of latent factors (in circles)—two additive genetic common factors (A1, A2), two shared environmental common factors (C1, C2), two unique environmental common factors (E1, E2)—and disorder-specific factors (A SP , C SP , E SP ). The first common factors (A1, C1, E1) plus E SP account for all of the variance of neuroticism, while the second common factors (A2, C2, E2) are independent of neuroticism. Paths that account for more than 5% of the variance in a phenotype (i.e., path loadings greater than √0.05, or 0.23) are depicted with thicker lines for emphasis.
The proportions of variance in liability for all of the phenotypes due to the factors included in these models are shown in Table 1 . Several key results regarding the pattern of genetic risk derive from this table. First, A1, the genetic factor for neuroticism, accounts for between one-third and two-thirds of the genetic liability for each of the disorders. Second, the neuroticism-independent common genetic factor, A2, was similarly important for major depression, generalized anxiety disorder, and panic and accounts for the majority of their remaining genetic liability. Third, a substantial proportion of the total risk variance shared between phenotypes is due to these two common genetic factors. Finally, disorder-specific sources of genetic risk not shared with these other phenotypes uniquely influence an individual’s liability to the phobic disorders.
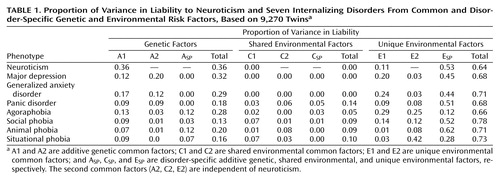
An alternative way to compare sources of covariation is by calculating bivariate genetic and environmental correlations, which are ratios of the covariance between two phenotypes to the square root of the products of their variance, where the variance and covariance used are genetic or environmental, respectively (15) . Table 2 lists the estimates for the genetic (r g ) and unique environmental (r e ) correlations between neuroticism and each of the internalizing disorders, again averaged across models for the nonphobic disorders. As indicated, the genetic correlations between neuroticism and each disorder are all positive and high, in the range of 0.60–0.82. The unique environmental correlations are somewhat lower (0.05–0.27). The point estimates for the shared environmental correlations (not shown) are both positive and negative but vary widely, not significantly differing from zero owing to the small parameter estimates from which they derive.
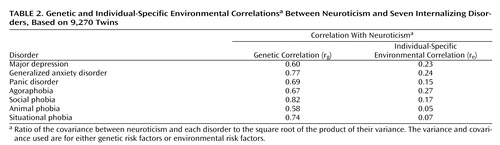
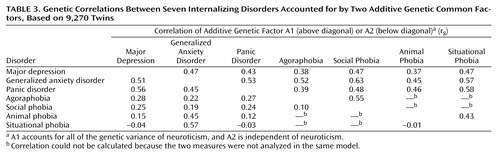
Table 3 shows the estimated genetic correlations between pairs of internalizing disorders that were included in the same models, separated into portions associated with the genetic factor for neuroticism (above the diagonal) and those independent of it (below the diagonal). The total genetic correlation between any two disorders is the sum of these two components. For example, the genetic correlation between major depression and generalized anxiety disorder is 0.47+0.51=0.98, while between panic disorder and situational phobia the genetic correlation is 0.58+(–0.03)=0.55. It is noteworthy that 50% or more of the genetic correlations between the internalizing disorders derives from the genetic factor for neuroticism.
Discussion
In this study we used multivariate modeling of twin data to examine the genetic and environmental risk factors shared by the personality trait neuroticism and a range of internalizing disorders. Our results suggest that the genetic factors underlying neuroticism are largely shared with those that influence liability to these conditions. Environmental risk factors, on the other hand, are only modestly correlated between these phenotypes. Furthermore, shared genetic factors account for a substantial amount of the comorbidity among the internalizing disorders, especially the genetic factors shared with neuroticism. These effects are roughly the same in men and women.
Relation to Previous Findings
To our knowledge, this is the first study to examine the factors underlying the relationship between neuroticism and a range of internalizing disorders. A large, population-based study of Australian twins that examined the covariation between neuroticism and current depression and anxiety symptoms showed genetic correlations between symptom scores and neuroticism of about 0.8 in both sexes (5) . Our group previously published the results of separate bivariate analyses on the sources of covariation between neuroticism and major depression (6) and between neuroticism and generalized anxiety disorder (7) , with findings consistent with those in the current study.
Several large, population-based phenotypic factor analytic studies examining comorbidity among psychiatric disorders have provided evidence for a single, higher-order “internalizing” factor that accounts for correlations among anxiety and depressive disorders and differentiates itself from an “externalizing” factor, which relates to the substance use and antisocial personality disorders (17 , 18) . The internalizing factor is made up of two lower, correlated factors, the first roughly corresponding to an “anxiety-misery” factor, which loads most strongly on major depression, dysthymia, and generalized anxiety disorder, and the second a “fear” factor, which loads primarily on panic and phobic disorders. This model has been expanded by our group through a population-based twin sample version of a similar factor analysis that allows differentiation of genetic and environmental components of these factors (19) . That study identified internalizing and externalizing genetic risk factors that help explain the phenotypic factor structure, the former being made up of analogous lower-order “anxiety-misery” and “fear” factors. In this context, the current analysis ascribes a somewhat different partitioning of this two-factor internalizing structure into genetic factors specifically shared or not shared with the Eysenck Personality Questionnaire concept of neuroticism. The genetic factors underlying individual differences in neuroticism exhibit significant overlap with the genetic risk for major depression, generalized anxiety disorder, panic disorder, and the phobias. They also account for a sizable proportion of the observed comorbidity among these disorders. Other common genetic risk factors not shared with neuroticism are important for major depression, generalized anxiety disorder, and panic disorder but hardly at all for phobias. In addition, each phobia type has contributions from disorder-specific genetic factors not accounted for by the two common genetic factors. One might speculate that, had we been able to analyze models with more than two common factors, a third factor might have been identified that represents genetic risk shared among the phobias alone.
Environmental Correlations
The finding of substantially smaller environmental than genetic correlations between disorders despite common factor loadings of similar magnitude is notable. Substantial factor loadings suggest that there are nonfamilial factors, such as an individual’s unique experience of stressful life events, that are etiologically related to the development of these conditions with nonspecific effects across disorders. For example, many forms of childhood adversity, such as childhood sexual abuse or parental loss or separation, are associated with adult psychiatric outcomes with little specificity (21 – 24) . However, any correlation between the different measures not shared with the subject’s co-twin could also elevate these factor loadings. Such correlation might arise from state effects of interviewing twins from a pair on different days, under different circumstances, etc. The discrepancy between the magnitude of the factor loadings and the environmental correlations arises largely from the greater contributions from the disorder-specific unique environmental factors, E SP , which decrease the correlations. These may similarly reflect either environmental risk factors not shared between disorders or disorder-specific sources of measurement error.
Gene Studies
These findings have several important implications for identifying candidate susceptibility genes for depressive and anxiety disorders. First, although many published studies have used the assumption that the phenotypic relationship between neuroticism and these conditions justifies its use in searching for genes for anxiety or depressive disorders, this study informs and extends those findings by establishing neuroticism as a reasonable target endophenotype in molecular genetic studies of a range of internalizing disorders. This has increasing relevance as both association studies (25) and linkage studies (26) have identified putative genetic regions that influence individual variation in neuroticism. Second, unlike in classic, Mendelian disorders, where pure, homogeneous phenotypes are the most powerful for identifying disease genes, for complex conditions like those studied herein, a phenotype that combines information from personality constructs, such as neuroticism, and several disorders may provide a more efficient initial target for gene-finding studies (27 , 28) . However, these results also show that neuroticism does not capture all the genetic variance underlying the internalizing disorders. Indeed, a second, neuroticism-independent common genetic factor was identified that accounted for a proportion of the genetic variance for the nonphobic internalizing disorders (major depression, generalized anxiety disorder, and panic disorder) that was similar to the proportion accounted for by the neuroticism-related common genetic factor.
Limitations
The results of this analysis should be interpreted in the context of several potential limitations. First, we used broadened diagnostic criteria for generalized anxiety disorder and panic disorder to increase prevalence and maximize our power to estimate model parameters. Prior analyses suggest that these approaches reflect the same continuum of liability as the fully syndromal disorders (11 , 12) . Consistent with this, our prior bivariate analysis of neuroticism and generalized anxiety disorder produced findings that did not strongly depend on the stringency of the definition used (7) .
Second, although the overall risk structure was generally invariant to sex, our study did not possess sufficient statistical power to determine whether the magnitudes and sources of genetic correlations among the phenotypes were the same or different in men and women. Thus, while such differences would have important implications for identifying susceptibility genes for these conditions, we were limited, despite the size of our sample, in our ability to establish their presence with a high degree of confidence.
Third, we had to restrict our analyses to the simultaneous modeling of six phenotypes in order to keep computer run times tractable; therefore, the analysis for animal and situational phobias was separate from that for agoraphobia and social phobia. This produced estimates of path coefficients and correlations for the remaining phenotypes (neuroticism, major depression, generalized anxiety disorder, and panic disorder) that differed somewhat from one model to another owing to stochastic variation. Calculating confidence intervals would have been desirable to estimate their precision, but the computer run times would have been prohibitively long.
Fourth, the findings of this analysis are predicated on the assumptions of the method used, that is, structural equation modeling of twins. These assumptions include independence and additivity of the latent variables, absence of assortative mating, and equal correlation in monozygotic and dizygotic twins for environmental experiences of relevance to the trait under study (15) . If the latter, known as the equal environment assumption, is violated, the greater similarity for monozygotic twins could potentially result from their increased environmental similarity instead of greater genetic similarity, potentially biasing the correlations obtained. Using several approaches to this problem, we have not been able to detect such violations for the psychiatric disorders examined in this study (29 , 30) .
Fifth, neuroticism and lifetime psychiatric diagnoses were each assessed at one time point, which potentially confounds the effects of individual-specific environment and measurement error, reducing the corresponding estimates of genetic effects. For example, we found, for major depression in our sample of female-female twin pairs, that improving the diagnostic reliability by reducing error through multiple, sequential assessments increased the heritability estimate substantially (31) . This measurement “noise” would reduce the correlations between twins and between measures. Given the low reliability for some measures, such as generalized anxiety disorder, this may have a substantial effect on our results. If this is the case, our analysis may have underestimated both genetic and environmental correlations.
Sixth, we were unable to examine the longitudinal relationship between neuroticism and the risk of developing any of the psychiatric disorders with the current design. In particular, we cannot differentiate state (i.e., “in episode”) and scar (“postepisode”) effects of illness on neuroticism that may disturb it from its premorbid or baseline level (32) . Similarly, while it is possible that some depressive and anxiety disorders might directly increase the risk for other disorders that we studied, our design does not test this model of causation.
Seventh, because the sample was made up entirely of Caucasian twin subjects born in Virginia, these results may not generalize to other groups.
1. Maser JD, Cloninger CR (eds): Comorbidity of Mood and Anxiety Disorders. Washington, DC, American Psychiatric Press, 1990Google Scholar
2. Andrews G, Stewart G, Morris-Yates A, Holt P, Henderson S: Evidence for a general neurotic syndrome. Br J Psychiatry 1990; 157:6–12Google Scholar
3. Bienvenu OJ, Brown C, Samuels JF, Liang KY, Costa PT, Eaton WW, Nestadt G: Normal personality traits and comorbidity among phobic, panic and major depressive disorders. Psychiatry Res 2001; 102:73–85Google Scholar
4. Khan AA, Jacobson KC, Gardner CO, Prescott CA, Kendler KS: Personality and comorbidity of common psychiatric disorders. Br J Psychiatry 2005; 186:190–196Google Scholar
5. Jardine R, Martin NG, Henderson AS: Genetic covariation between neuroticism and the symptoms of anxiety and depression. Genet Epidemiol 1984; 1:89–107Google Scholar
6. Fanous A, Gardner CO, Prescott CA, Cancro R, Kendler KS: Neuroticism, major depression and gender: a population-based twin study. Psychol Med 2002; 32:719–728Google Scholar
7. Hettema JM, Prescott CA, Kendler KS: Genetic and environmental sources of covariation between generalized anxiety disorder and neuroticism. Am J Psychiatry 2004; 161:1581–1587Google Scholar
8. Eaves LJ, Eysenck HJ, Martin NG, Jardine R, Heath AC, Feingold L, Young PA, Kendler KS: Genes, Culture and Personality: An Empirical Approach. New York, Academic Press, 1989Google Scholar
9. Kendler KS, Prescott CA: A population-based twin study of lifetime major depression in men and women. Arch Gen Psychiatry 1999; 56:39–44; correction, 2000; 57:94–95Google Scholar
10. Eysenck HJ, Eysenck SBG: Eysenck Personality Questionnaire Manual. London, Hodder and Stoughton, 1975Google Scholar
11. Hettema JM, Prescott CA, Kendler KS: A population-based twin study of generalized anxiety disorder in men and women. J Nerv Ment Dis 2001; 189:413–420Google Scholar
12. Kendler KS, Gardner CO, Prescott CA: Panic syndromes in a population-based sample of male and female twins. Psychol Med 2001; 31:989–1000Google Scholar
13. Kendler KS, Myers J, Prescott CA, Neale MC: The genetic epidemiology of irrational fears and phobias in men. Arch Gen Psychiatry 2001; 58:257–265Google Scholar
14. Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ: The genetic epidemiology of phobias in women: the interrelationship of agoraphobia, social phobia, situational phobia, and simple phobia. Arch Gen Psychiatry 1992; 49:273–281Google Scholar
15. Neale MC, Cardon LR: Methodology for Genetic Studies of Twins and Families. Dordrecht, The Netherlands, Kluwer Academic, 1992Google Scholar
16. Neale MC, Boker SM, Xie G, Maes HH: Mx: Statistical Modeling, 5th ed. Richmond, Medical College of Virginia of Virginia Commonwealth University, Department of Psychiatry, 1999Google Scholar
17. Krueger RF: The structure of common mental disorders. Arch Gen Psychiatry 1999; 56:921–926Google Scholar
18. Vollebergh WA, Iedema J, Bijl RV, de Graaf R, Smit F, Ormel J: The structure and stability of common mental disorders: the NEMESIS study. Arch Gen Psychiatry 2001; 58:597–603Google Scholar
19. Kendler KS, Prescott CA, Myers J, Neale MC: The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Arch Gen Psychiatry 2003; 60:929–937Google Scholar
20. Akaike H: Factor analysis and AIC. Psychometrika 1987; 52:317–332Google Scholar
21. Kessler RC, Davis CG, Kendler KS: Childhood adversity and adult psychiatric disorder in the US National Comorbidity Survey. Psychol Med 1997; 27:1101–1119Google Scholar
22. Lindesay J: Phobic disorders in the elderly. Br J Psychiatry 1991; 159:531–541Google Scholar
23. Harris T, Brown GW, Bifulco A: Loss of parent in childhood and adult psychiatric disorder: the role of lack of adequate parental care. Psychol Med 1986; 16:641–659Google Scholar
24. Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ: Childhood parental loss and adult psychopathology in women: a twin study perspective. Arch Gen Psychiatry 1992; 49:109–116Google Scholar
25. Lesch KP, Bengel D, Heils A, Sabol SZ, Greenberg BD, Petri S, Benjamin J, Muller CR, Hamer DH, Murphy DL: Association of anxiety-related traits with a polymorphism in the serotonin transporter gene regulatory region. Science 1996; 274:1527–1531Google Scholar
26. Fullerton J, Cubin M, Tiwari H, Wang C, Bomhra A, Davidson S, Miller S, Fairburn C, Goodwin G, Neale MC, Fiddy S, Mott R, Allison DB, Flint J: Linkage analysis of extremely discordant and concordant sibling pairs identifies quantitative-trait loci that influence variation in the human personality trait neuroticism. Am J Hum Genet 2003; 72:879–890Google Scholar
27. Kirk KM, Birley AJ, Statham DJ, Haddon B, Lake RI, Andrews JG, Martin NG: Anxiety and depression in twin and sib pairs extremely discordant and concordant for neuroticism: prodromus to a linkage study. Twin Res 2000; 3:299–309Google Scholar
28. Nash MW, Huezo-Diaz P, Williamson RJ, Sterne A, Purcell S, Hoda F, Cherny SS, Abecasis GR, Prince M, Gray JA, Ball D, Asherson P, Mann A, Goldberg D, McGuffin P, Farmer A, Plomin R, Craig IW, Sham PC: Genome-wide linkage analysis of a composite index of neuroticism and mood-related scales in extreme selected sibships. Hum Mol Genet 2004; 13:2173–2182Google Scholar
29. Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ: A test of the equal environment assumption in twin studies of psychiatric illness. Behav Genet 1993; 23:21–27Google Scholar
30. Hettema JM, Neale MC, Kendler KS: Physical similarity and the equal-environment assumption in twin studies of psychiatric disorders. Behav Genet 1995; 25:327–335Google Scholar
31. Foley DL, Neale MC, Kendler KS: Reliability of a lifetime history of major depression: implications for heritability and co-morbidity. Psychol Med 1998; 28:857–870Google Scholar
32. Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ: A longitudinal twin study of personality and major depression in women. Arch Gen Psychiatry 1993; 50:853–862Google Scholar

