
Predeployment Personality Traits and Exposure to Trauma as Predictors of Posttraumatic Stress Symptoms: A Prospective Study of Former Peacekeepers
Abstract
OBJECTIVE: The authors’ goal was to study the contribution of predeployment personality traits and exposure to traumatic events during deployment to the development of symptoms of posttraumatic stress disorder (PTSD) in individuals involved in military peacekeeping activities.METHOD: Five hundred seventy-two male veterans who participated in the United Nations Protection Force mission in the former Yugoslavia completed a short form of the Dutch MMPI before deployment. Following deployment, they participated in a survey of all Dutch military veterans who had been deployed in the years 1990–1995 and completed the Self-Rating Inventory for PTSD.RESULTS: Exposure to traumatic events during deployment had the highest unique contribution to the prediction of PTSD symptom severity, followed by the personality traits of negativism and psychopathology, followed by age.CONCLUSIONS: Both pretrauma vulnerabilities and exposure to traumatic events were found to be important factors in the etiology of posttraumatic stress symptoms. The current study replicates in a non-American sample of peacekeepers findings obtained among American Vietnam veterans. Particularly, there is accumulating evidence for an etiological role of the personality trait of psychoneuroticism in the development of posttraumatic stress symptoms.
To understand adaptation to trauma, particularly the development of posttraumatic stress symptoms, several models have been proposed. These models include personality and situation characteristics as explaining variables. Debate centers around the question of which variables are most important. Some authors have claimed that posttraumatic stress symptoms will develop in those individuals who were already vulnerable before they were exposed to trauma, but others have argued that exposure to traumatic events is the primary cause for symptoms of traumatic stress.
Definitive conclusions are hard to make because most studies in this area assessed personality characteristics following exposure to trauma. For instance, King and colleagues (1) found that the personality disposition termed “hardiness” was a significant and strong predictor of posttraumatic stress disorder (PTSD). McFarlane (2) found that a postdisaster-derived measure of neuroticism was associated with chronic psychopathology following the disaster. To consider these posttrauma personality measures as a reliable representation of pretrauma personality may be problematic. First, trauma may bring about changes in an individual’s personality (3–5); second, the individual’s present mood associated with PTSD is likely to influence the score profile on trait measures. Because of these problems, it is quite possible that consequences and not causes of PTSD have been measured in the studies cited.
Since trauma strikes suddenly and unexpectedly, prospective studies including personality traits that were measured before the traumatic event are rare. Card (6) performed a prospective study of Vietnam veterans and found that exposure to combat was more strongly correlated with later PTSD than with individual background variables measured at age 15. Of these variables, only low self-confidence was related to later PTSD. An important shortcoming of this study is that the measures of PTSD and personality traits were not validated.
In 1993, Schnurr and colleagues (7) published a prospective study that used MMPI scores collected during high school to assess predictors of combat-related lifetime symptoms of PTSD in male Vietnam veterans. They found that both personality traits and stressor characteristics were important predictors for the development of PTSD. A logistic regression analysis showed that the MMPI measures psychopathic deviate, masculinity-femininity, and combat exposure predicted lifetime PTSD symptoms.
In the present study we examined whether the results of Schnurr et al. obtained among an American sample of Vietnam veterans can be replicated in a non-American sample of former United Nations (UN) peacekeepers. Personality characteristics were obtained before deployment with the short form of the Dutch version of the MMPI. We examined whether predeployment personality characteristics were predictive of PTSD symptoms following deployment, controlling for predeployment demographic variables and the reported traumatic events during deployment. We also examined the unique contributions of the different variables to the development of PTSD symptoms.
Method
The participants were 572 male veterans who voluntarily fulfilled their compulsory military service by taking part in the UN Protection Force mission in the former Yugoslavia in 1993–1995. In a selection procedure of the Dutch Royal Army (time 1), consisting of a medical checkup and a semistructured interview with a psychologist, they were determined to be physically and mentally healthy and suited for deployment. As a part of the procedure, candidates filled out the short form of the Dutch version of the MMPI (8).
Following deployment, in 1996 (time 2), the subjects took part in a survey of all Dutch Royal Army veterans who had participated in peacekeeping missions in the years 1990–1995 and had left active service. A manuscript reporting the findings of this survey has been submitted for publication elsewhere. The veterans received a questionnaire by post with a cover letter explaining the purpose of the study and returned the completed questionnaire using a prepaid return envelope, thereby giving informed consent.
Predeployment personality traits were measured with a short form of the Dutch adaptation of the MMPI by Luteijn and Kok (8). This instrument consists of 83 items ordered into five scales. The negativism scale (22 items) measures a negative, dissatisfied, and hostile attitude toward others and life in general. The somatization scale (20 items) measures functional somatic complaints. The shyness scale (15 items) measures social inadequacy and fear for social contact. The psychopathology scale (13 items) measures paranoid ideas and psychotic experiences. The extroversion scale (13 items) measures outgoing behavior and a tendency to socialize with others. In Dutch populations, the scales have been found to be internally consistent and to have sound test-retest reliability and validity. No profiles have been developed for the Dutch MMPI. The scale scores were translated by using the general norm table into scores ranging from 1 (very low) to 7 (very high) (8).
The Self-Rating Inventory for PTSD developed by Hovens and colleagues (9) was also used. Three subscales on this instrument correspond to the symptom clusters of DSM-IV: reexperiencing (six items), avoidance (nine items), and hyperarousal (seven items). Summing scores on these subscales together leads to a total score of PTSD symptom severity. Each of the 22 items can be answered on a 4-point scale ranging from 1 (not at all) to 4 (very much). The validity, internal consistency, and test-retest reliability of the Self-Rating Inventory for PTSD have been found to be excellent (9).
A list of 13 possible traumatic events during deployment was presented, including the question of whether the subject experienced shootings directed at other people and/or at the subject himself and whether the subject was held at gunpoint, rejected by the local population, or witnessed human distress. Answer categories were yes or no. A summary score counted the number of events reported. The scale has an adequate test-retest reliability of 0.72 (manuscript in preparation).
A hierarchical multiple regression analysis with PTSD symptom severity in 1996 as the dependent variable was performed. To control the order of entry of variables in the regression equation, the independent variables were entered in three steps (10). First, the demographic variables age and level of education before deployment were entered, followed by the five predeployment personality traits, and, finally, the exposure variables. In each step, we examined the “effect” of variables entered, controlling for variables entered in previous steps. In this way, the analysis shows whether predeployment personality traits have a significant contribution to make, controlling for age and level of education, and whether exposure to stressful events contributes significantly to the prediction of PTSD symptoms, controlling for personality traits, age, and level of education.
Results
All 572 of the participants were male, and at time 1 their ages ranged from 16 to 27 years (mean=20.9, SD=2.1). At time 1, the majority had a lower (N=248 [43%]) or middle (N=281 [49%]) level of education, and 41 (7%) had a higher educational level. At the time of deployment, their ages ranged from 18 to 28 years (mean=21.8, SD=2.1). During deployment, four (1%) held the rank of officer, 17 (3%) were noncommissioned officers, and 538 (94%) held a rank below noncommissioned officer. The typical duration of the deployment was 6 months (SD=1.8). In 1996 (time 2), the subjects’ mean age was 24.0 (SD=2.1), and 160 (28%) had a lower level of education, 318 (56%) had obtained a middle level, and 89 (16%) a higher level of education.
The most frequently reported stressors during deployment were shootings not directed at the subject, reported by 488 (85%) of the men, witnessing human distress (N=415 [73%]), rejection by the local population (N=311 [54%]), and sight of dead and/or wounded people (N=269 [47%]). The participants reported experiencing a mean number of 4.6 stressful events (SD=2.4). In 1996, according to a cutoff score of 53 or higher on the Self-Rating Inventory for PTSD (9), 17 veterans (3%) fulfilled the criteria for a diagnosis of PTSD, and 120 veterans (21%) fulfilled at least one criterion for PTSD.
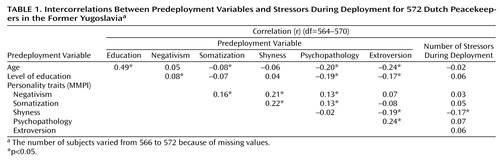
Table 1 shows the intercorrelations between the predictors of postdeployment adjustment. Predeployment age and level of education were moderately significantly and moderately strongly correlated. Most intercorrelations between the MMPI personality traits were significant but modest in size. Correlations between predeployment variables and the number of stressors during deployment were not statistically significant with one exception. A significant but small negative correlation was found between shyness and the number of war events.
Table 2 summarizes the results of the hierarchical multiple regression analysis. In model 1, with predeployment demographic variables only, age was significantly correlated with PTSD symptom severity. Age remained statistically significant when the other variables were entered. A younger age was associated with higher scores on PTSD symptom severity. When age was controlled for, educational level was no longer significantly correlated with PTSD.
Model 2, which controlled for age and level of education, showed that three personality variables—negativism, somatization, and psychopathology—were significantly correlated with PTSD symptom severity. Together, the variables of model 2 explained 10% of the variance (Table 1). In model 3, which controlled for exposure to traumatic events, negativism, and psychopathology, remained statistically significant. In model 3, with the inclusion of the number of events during deployment, the percentage of variance explained increased to 19% (Table 3). In this final model, the number of stressor events during deployment had the highest semipartial correlation, followed by the predeployment personality traits of negativism and psychopathology and, finally, age.
Discussion
We examined the contributions of predeployment personality traits, demographic variables, and exposure to stressors during deployment as a military peacekeeper to the development of PTSD symptoms afterwards. The personality traits were measured with a reliable and valid questionnaire, the short version of the Dutch MMPI. Before deployment, the men in this sample were found to be physically and mentally healthy and suited for taking part in the UN Protection Force mission in the former Yugoslavia. They were part of a random sample of peacekeepers who had left active service in 1996 and were not selected because they needed treatment.
One shortcoming of the study must be mentioned. The personality scores were obtained during the selection procedure, and the wish to take part in a peacekeeping mission may have inclined the men to give favorable answers. If such bias has occurred, the influence of personality scores may, in fact, be more influential for the later development of PTSD symptoms than our data suggest.
Multiple regression analysis showed that the number of stressors during deployment was the most important predictor of PTSD symptom severity, followed by two predeployment personality traits—negativism and psychopathology—and, finally, age. The personality trait of somatization was a significant predictor of PTSD symptoms in model 2 but not in the final model. The effect of the number of stressors during deployment was largely independent of the effect of predeployment personality traits. In other words, predeployment personality traits did not provide an explanation for the correlation between reporting exposure to stressful events and PTSD symptom severity.
These findings are in concordance with those of Schnurr et al. (7), who found that both MMPI scores obtained in college and stressors during Vietnam were significant predictors of lifetime symptoms of PTSD. Using logistic regression analysis, Schnurr et al. found a higher adjusted odds ratio for combat exposure than for the personality traits. Our findings lend additional support to a model that includes personality traits as well as the experience of stressors.
Doubts about the validity of self-reports of traumatic events, such as those used in the current study, have been raised (11). In particular, a correlation has been found between an increase in the number of reported events over time and symptoms of PTSD. Other studies (12, 13), however, have provided support for the accuracy of retrospective reports. These studies found that subjects were not very accurate in recalling exact details of the events, but they did well in reporting whether or not the event had occurred. In addition, preliminary analyses of our own data showed that our scale of events during deployment had good test-retest reliability, and, in contrast to Southwick et al. (11), we found no correlations between the number of disconcordances over time and symptoms of PTSD (manuscript in preparation). Therefore, it is very unlikely that the correlation between PTSD symptoms and events during peacekeeping found in the current study is fully explained by problems with recall in healthy peacekeepers or with increased recall in PTSD sufferers.
The peacekeepers were selected for participation in the UN Protection Force on the basis of their personality profile and a clinical interview. Those who were thought to have a high risk of developing adjustment problems were not deployed. Therefore, most MMPI scores were within the normal range. Nevertheless, these scores significantly predicted the development of symptoms of PTSD. It is important to note that the model including personality and exposure to traumatic events explained 19% of the variance, leaving room for still other variables not included in the current study.
Since the Dutch MMPI scales differ from the American scales, a straightforward comparison between the study of Schnurr et al. (7) and our study is not possible. However, the description of the Dutch negativism scale (having a negative, dissatisfied, and hostile attitude toward others and life in general) is very much in line with the description of the American psychopathic deviate scale (gloominess, dissatisfaction, impulsivity, and irritability). In addition, the Dutch negativism scale has been found to correlate highly with measures of psychoneuroticism (8). Thus, two prospective studies examining different populations exposed to traumatic stress provide support on a predisposing role of psychoneuroticism. Therefore, there is reason to believe that McFarlane’s study of firefighters (2), which used a posttrauma-derived measure of psychoneuroticism, did indeed measure a pretrauma vulnerability.
Our finding that psychopathology (having paranoid ideas and psychotic experiences) is uniquely correlated with PTSD is not in line with the findings of previous studies. Although Schnurr et al. (7) did find a significant association between paranoia and developing PTSD symptoms, they also found that this association was fully accounted for by other MMPI scales. Similarly, we found an association between somatization and PTSD symptom severity that was largely explained by other personality traits. Thus, these findings are not consistent across studies and should be treated with caution.
An issue of interest relates to the mechanisms that are involved in the differential adaptation to traumatic stress of individuals with certain personality traits as opposed to others. This may be understood in terms of the cognitive-motivational-relation theory (14). According to this theory, the interaction between person and environment determines the appraisal of and meaning attributed to the situation. This, in turn, influences coping activities and the experience of social support. These variables may alter the environment, the person, and indirectly the interaction between the two. Thus, in this complex and dynamic interaction, certain preexisting personality traits may influence not only the appraisal of stress but also the coping activities that follow. For instance, the peacekeepers with high scores on negativism, psychopathology, and somatization may appraise certain situations as more dangerous and threatening than peacekeepers with lower scores on these personality traits. Consequently, they may experience higher levels of anxiety, which place a greater demand on their capacity for working through the experience. In the aftermath of trauma, some personality traits may predispose individuals to engage in less successful coping strategies. For instance, individuals with high scores on negativism (having a negative, dissatisfied and hostile attitude toward others and life in general) may be less inclined to seek social support.
Similarly, the tendency to react to stressful situations with somatic complaints may actually be the result, or concomitant, of an avoidant coping style (15). Perhaps somatizers do not want to face their emotional problems directly, and this may lead to somatic symptoms and PTSD. Alternatively, it has been hypothesized that somatizers may have difficulties in recognizing and naming their own emotions, and that this may hinder or complicate the process of working through traumatic events (16). Yet another possibility is that somatizers have specific physical vulnerabilities that put them at risk for developing certain somatic symptoms in response to stress.
Another question to be raised is to what extent these results may be generalized to other populations. Are they specific to peacekeepers and peacekeeping stressors or can they be generalized to other populations as well? We may speculate that these results do have a broader relevance to human adaptation to stress, but further research is necessary among different populations, facing different stressful situations, to settle this issue. For such studies, an interesting hypothesis is that the etiological role of personality factors in the development of psychological adjustment problems (including adjustment disorder as well as PTSD) will decrease as stressor intensity increases (17).
In sum, the current study of Dutch peacekeepers has provided a replication of findings obtained among American Vietnam veterans, i.e., that both pretrauma personality and exposure to trauma are important factors in the etiology of posttraumatic stress symptoms. Particularly, there is accumulating evidence for an etiological role of the personality trait of psychoneuroticism. More studies, preferably with a prospective design, are needed to clarify to what extent other personality traits are involved in the development of symptoms of PTSD.
 |
 |
 |
Received July 26, 1999; revision received Jan. 6, 2000; accepted Jan. 27, 2000. From the Department of Medical Psychology, Vrije Universiteit, Amsterdam. Address reprint requests to Dr. Bramsen, Vrije Universiteit Amsterdam, Department of Medical Psychology, Van der Boechorststraat 7, 1081 BT Amsterdam, the Netherlands; [email protected] (e-mail). The authors thank the Dutch Ministry of Defense for making available part of the data.
1. King LA, King DW, Fairbank JA, Keane TM, Adams GA: Resilience-recovery factors in post-traumatic stress disorder among female and male Vietnam veterans: hardiness, postwar social support, and additional stressful life events. J Pers Soc Psychol 1998; 74:420–434Crossref, Medline, Google Scholar
2. McFarlane AC: The longitudinal course of posttraumatic morbidity: the range of outcomes and their predictors. J Nerv Ment Dis 1988; 176:30–39Crossref, Medline, Google Scholar
3. Herman JL: Trauma and Recovery. New York, Basic Books, 1993Google Scholar
4. Reich JH: Personality disorders and posttraumatic stress disorder, in Posttraumatic Stress Disorder: Etiology, Phenomenology, and Treatment. Edited by Wolf ME, Mosnaim AD. Washington, DC, American Psychiatric Press, 1990, pp 65–79Google Scholar
5. Peterson KC, Prout MF, Schwarz RA: Post-Traumatic Stress Disorder: A Clinician’s Guide. New York, Plenum, 1991Google Scholar
6. Card JJ: Epidemiology of PTSD in a national cohort of Vietnam veterans. J Clin Psychol 1987; 43:6–17Crossref, Medline, Google Scholar
7. Schnurr PP, Friedman MJ, Rosenberg SD: Preliminary MMPI scores as predictors of combat-related PTSD symptoms. Am J Psychiatry 1993; 150:479–483Link, Google Scholar
8. Luteijn F, Kok AR: [NVM: The Dutch Short Version of the MMPI Manual.] Lisse, the Netherlands, Swets & Zeitlinger, 1985 (Dutch)Google Scholar
9. Hovens JE, Van der Ploeg HM, Bramsen I, Klaarenbeek MTA, Schreuder JN, Rivero VV: The development of the Self-Rating Inventory for Posttraumatic Stress Disorder. Acta Psychiatr Scand 1994; 90:172–183Crossref, Medline, Google Scholar
10. Tabachnick BG, Fidell LS: Using Multivariate Statistics, 2nd ed. New York, HarperCollins, 1989Google Scholar
11. Southwick SM, Morgan CA III, Nicolaou AL, Charney DS: Consistency of memory for combat-related traumatic events in veterans of Operation Desert Storm. Am J Psychiatry 1997; 154:173–177Link, Google Scholar
12. Henry B, Moffit TE, Caspi A, Langley J, Silva PA: On the “remembrance of things past”: a longitudinal evaluation of the retrospective method. Psychol Assess 1994; 6:92–101Crossref, Google Scholar
13. Wagenaar WA, Groeneweg J: The memory of concentration camp survivors. Applied Cognitive Psychol 1990; 4:77–87Crossref, Google Scholar
14. Lazarus RS: Emotion and Adaptation. New York, Oxford University Press, 1991Google Scholar
15. Sharpe M, Mayou R, Bass C: Concepts, theories, and terminology, in Treatment of Functional Somatic Symptoms. Edited by Mayou R, Bass C, Sharpe M. New York, Oxford University Press, 1995, pp 3–16Google Scholar
16. Krystal H: Integration and Self-Healing: Affect, Trauma, and Alexithymia. Hillsdale, NJ, Lawrence Erlbaum Associates, 1988Google Scholar
17. Foy DW, Resnick HS, Sipprelle RC, Carroll EM: Premilitary, military, and postmilitary factors in the development of combat-related stress disorders. Behavior Therapist 1987; 10:3–9Google Scholar

