
Efficacy and Tolerability of Vardenafil in Men With Mild Depression and Erectile Dysfunction: The Depression-Related Improvement With Vardenafil for Erectile Response Study
Abstract
OBJECTIVE: Erectile dysfunction and depression are highly associated. Previous studies have shown benefits of phosphodiesterase-5 inhibitor treatment for erectile dysfunction associated with antidepressant therapy or subsyndromal depression. The present study assessed the safety and efficacy of vardenafil in men with erectile dysfunction and untreated mild depression. METHOD: In this 12-week, multicenter, randomized, flexible-dose, parallel-group, double-blind study, 280 men with erectile dysfunction for at least 6 months and untreated mild major depression received placebo or vardenafil, 10 mg/day, for 4 weeks, with the option to titrate to 5 mg/day or 20 mg/day after each of two consecutive 4-week intervals. Endpoints included International Index of Erectile Function erectile function domain and 17-item Hamilton Depression Rating Scale (HAM-D) scores. RESULTS: Vardenafil produced statistically significant and clinically meaningful improvement in all erectile function parameters. The International Index of Erectile Function erectile function domain score was 22.9 with vardenafil compared to 14.9 with placebo. The HAM-D score was lower in the vardenafil group (7.9) than in the placebo group (10.1). Treatment with vardenafil was the most important predictor for return to normal erectile function. Improvement in International Index of Erectile Function erectile function domain score was the most important predictor of remission in depressive symptoms. CONCLUSIONS: Vardenafil was well tolerated and highly efficacious in men with erectile dysfunction and untreated mild major depression. Significant improvements in erectile function and depression were observed in patients treated with vardenafil versus placebo. Erectile dysfunction treatment should be considered a component of therapy for men with depression and erectile dysfunction.
Erectile dysfunction is highly prevalent among men between 40 and 70 years of age, and the estimated lifetime prevalence of major depression (6% to 10%) is considerable (1). A loss of interest in and withdrawal from all regular and pleasurable activities are often associated with depression (2). Sexual disorders are also common in association with depression; however, the mechanisms underlying the link between depression and sexual dysfunction are complex. Erectile dysfunction may contribute to, or be a consequence of, depression. Several factors can be involved, including loss of self-esteem, performance anxiety, and a reduced quality of life (3).
The Massachusetts Male Aging Study showed that men with untreated depression had a 1.8-fold greater chance of experiencing erectile dysfunction than men without depression, and erectile dysfunction increased with increasing degree of depression (4, 5). Phosphodiesterase-5 (PDE-5) inhibitors have been used to effectively and safely treat erectile dysfunction in patients with depression, including patients treated with antidepressant therapy (6–10). To our knowledge, none of the studies reported to date has investigated the potential mental health benefits of PDE-5 inhibitor therapy in men with erectile dysfunction and untreated mild major depressive disorder. Because this population represents a large cohort of men, many of whom are reluctant to use antidepressant therapies, treatment for erectile dysfunction that has a positive impact on depressive symptoms may be an attractive therapeutic option (5–9).
Vardenafil is a potent selective PDE-5 inhibitor that has been shown to be highly efficacious in men with erectile dysfunction, irrespective of severity or disease classification (organic, psychogenic, or mixed) (11) or underlying etiology (12). The drug is well tolerated and is associated with a rapid and reliable treatment response. The objective of the Depression-Related Improvement With Vardenafil for Erectile Response Study was to evaluate the efficacy of vardenafil in the treatment of men with erectile dysfunction and clinically diagnosed but untreated mild major depressive disorder.
Method
Study Participants
This 12-week, flexible-dose, parallel-group, double-blind study was conducted in 44 centers comprising the disciplines of urology, psychiatry, general practice, and endocrinology in the United States, Canada, France, Spain, and Italy between Dec. 3, 2002, and Nov. 27, 2003. Of a total of 488 men screened, 280 were subsequently randomly assigned. The subjects were ≥18 years of age and had experienced erectile dysfunction for >6 months according to National Institutes of Health criteria (13). Inclusion criteria were participation in a stable heterosexual relationship for more than 6 months and having diagnosed but untreated mild major depressive disorder. During the early part of the investigation, the subjects were included if they had a 17-item Hamilton Depression Rating Scale (HAM-D) score between 13 and 23 at visits 1 and 2 and a Center for Epidemiologic Studies Depression Scale (CES-D Scale) (14) score >13 at visit 1. HAM-D rating was performed by an interview with a blinded expert who was generally not aware of the response to treatment. At the request of the steering committee but in the absence of any treatment-related serious adverse events, entry criteria for depression severity in the study were modified. The protocol was amended while the study was in progress to include only subjects with HAM-D scores between 11 and 17 rather than between 13 and 23. The subjects were not in psychotherapy or taking antidepressant medication. The subjects made at least four attempts at sexual intercourse on 4 separate days during the untreated baseline period. For inclusion in the study, at least 50% of the attempts at sexual intercourse failed because of partial erections, unsuccessful penetration, or unsuccessful intercourse. Written informed consent was obtained from the subjects after a complete description of the study had been given to them.
Exclusion criteria included any unstable medical condition or substance abuse; a serious suicidal or homicidal risk (patients who scored >0 on item 3 of the HAM-D or who made a suicide attempt in the 12 months before screening); or a history of bipolar disorder, schizophrenia, schizoaffective disorder, delusional disorder, panic disorder, posttraumatic stress disorder, or personality disorder. Three patients were excluded because of dysthymia. Subjects were also excluded based on the presence of penile anatomical abnormalities, primary hypoactive sexual desire, erectile dysfunction related to spinal cord injury, prior nonresponse to sildenafil, retinitis pigmentosa, or radical prostatectomy.
Study Design
After a 4-week run-in period without medication, the subjects were randomly assigned to receive placebo or vardenafil, 10 mg/day, for 4 weeks. Erectile function was assessed based on subjective patient diary responses to questions evaluating each sexual experience. At week 4, the investigator and each patient reviewed the efficacy and tolerability of the initial dose, and a clinical decision was made as to whether the initial dose was maintained, increased to 20 mg/day, or decreased to 5 mg/day for the next 4 weeks. At week 8, the investigator and each patient again discussed and evaluated the efficacy and tolerability and adjusted the dose by one step or maintained the previous dose for the final 4 weeks of the study.
Primary endpoints were the International Index of Erectile Function erectile function domain score (15), in which a clinically significant improvement was defined as a change of 5 points, and a HAM-D total score at last observation carried forward if the erectile function analysis was successful. In this study, a significant improvement in mood was considered to be a decrease of 3.5 points on the HAM-D scale in vardenafil-treated patients compared to placebo. Secondary erectile function endpoints included the Sexual Encounter Profile Questionnaire (available from the first author), in which patients responded “yes” or “no” to the following questions after each sexual attempt: “Were you able to insert your penis into your partner’s vagina?” (question 2), and “Did your erection last long enough for you to have successful intercourse?” (question 3). Other erectile function indices included additional domains from the International Index of Erectile Function, including orgasmic function, sexual desire, intercourse satisfaction, overall satisfaction, and response to a global assessment question in which patients responded “yes” or “no” to the question, “Has the treatment you have been taking over the past 4 weeks improved your erections?” Other assessments included the CES-D Scale and the Rosenberg Self-Esteem Scale (16). The magnitude of HAM-D improvement was summarized by the following: HAM-D responses corresponding to remission (final HAM-D score ≤7), response (a decrease in HAM-D score ≥50%), or improvement (a decrease in HAM-D score >3.5 points). A 24-hour follow-up after the last dose of study drug was performed to monitor for serious adverse events.
Statistical Analysis
The number of subjects required in this study was based on the primary efficacy variables, which were tested in a hierarchical fashion. The International Index of Erectile Function erectile function domain score was analyzed first, and if the analysis was successful, then the HAM-D score was assessed. Because of the predefined testing sequence of the primary variables, no alpha adjustment was made. The group size calculations assumed a standard deviation of 10.0 for erectile function domain scores on the International Index of Erectile Function and 7.5 for HAM-D total scores. With approximately 86 (International Index of Erectile Function erectile function domain) and 98 (HAM-D) subjects per treatment group with data for the primary analyses, this study had a power of approximately 90%. On the basis of an estimated postrandomization dropout rate of 25%, 131 subjects per treatment group were needed for random assignment.
The intent-to-treat group included patients who took at least one dose of study medication and who had baseline and any postbaseline efficacy data. Analysis of the International Index of Erectile Function erectile function domain score, HAM-D score, and other efficacy variables was based on the intent-to-treat group by using the last-observation-carried-forward method to account for dropouts. Analysis of the diary variables was also based on this group, as was the overall postbaseline per-patient success rate for each variable.
The International Index of Erectile Function erectile function domain and HAM-D scores were analyzed with analysis of covariance (ANCOVA), with baseline response as a covariate and terms for center and treatment. The difference in least squares means between vardenafil-treated patients and patients receiving placebo at p<0.05 was considered to be significant.
Responses to the second and third questions of the Sexual Encounter Profile were analyzed with an ANCOVA on a per-patient success rate and included baseline as a covariate. The per-patient success rate was calculated as the number of successes divided by the number of sexual attempts with the number of responses for the question. The global assessment question was analyzed with logistic regression analysis.
To explore which parameters may be predictive of a return to normal erectile function (International Index of Erectile Function erectile function domain score ≥26 or HAM-D score ≤7), retrospective stepwise logistic regression analyses were performed. Entry-level criteria for each predictor of p<0.10 were stipulated, and each predictor was removed from the model if the p value exceeded 0.15. For exploration of the factors predictive of a return to normal erectile function, independent variables included the International Index of Erectile Function erectile function domain baseline score, the HAM-D baseline score, age, duration of erectile dysfunction, treatment, HAM-D change in score, and HAM-D return to normal score. For exploration of factors predictive of a return to normal HAM-D score, independent variables included International Index of Erectile Function erectile function domain baseline score, HAM-D baseline score, age, duration of erectile dysfunction, treatment, International Index of Erectile Function erectile function domain change in score, and International Index of Erectile Function erectile function domain return to normal score.
Results
Study Design
After a 4-week untreated run-in period, this 12-week, multicenter, flexible-dose, parallel-group, double-blind study randomly assigned 280 men to treatment with placebo (N=143) or 10 mg/day of vardenafil (N=137) for 4 weeks. At the end of weeks 4 and 8, the subjects, in collaboration with their physicians, had the option to titrate their dose to 5 mg/day or 20 mg/day of vardenafil or the equivalent of placebo. The majority of patients taking placebo (N=122, 93.8%) or vardenafil (N=95, 73.1%) opted to titrate to the 20 mg/day dose by the end of treatment; 111 of the subjects in the placebo group (78%) and 118 in the vardenafil group (86%) completed the study. Premature discontinuation was most commonly attributed to adverse events (2 of 143, 1%, in the placebo group versus 4 of 137, 3%. in the vardenafil group), insufficient therapeutic effect (N=10, 7%, versus N=2, 1%), withdrawn consent (N=9, 6%, versus N=3, 2%), or loss to follow-up (N=10, 7%, versus N=5, 4%).
Patient Group Profile
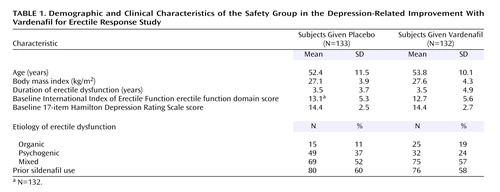
Baseline International Index of Erectile Function erectile function domain scores indicated moderate erectile dysfunction, with safety group scores of 12.7 (SD=5.6) in the vardenafil group and 13.1 (SD=5.3) in the placebo group. The subjects were diagnosed with erectile dysfunction an average of 3.5 years (SD=4.3) before the screening. Erectile dysfunction was of organic, psychogenic, or mixed etiology, with mixed etiology being the most common. Approximately 75% of the patients were Caucasian, 8% were black, 2% were Asian, <1% were American Indian, <1% were Hispanic, and 14% were patients from France, where race was not reported. In general, the patients were overweight (mean weight=85 kg, SD=15), as assessed by body mass (mean=27 kg/m2, SD=4) and Broca (mean=1.1, SD=0.2) indices. Mean age was 53 years (SD=11). Approximately 49% of the patients were nonsmokers, and 51% were past or present smokers. Twenty-nine percent of the group suffered from vascular hypertensive disorders, 15% had diabetes mellitus, 12% had elevated cholesterol, and all had mild major depressive disorder. Depression was diagnosed or confirmed by trained and qualified clinicians according to DSM-IV criteria with a structured interview (the Mini International Neuropsychiatric Interview [17] or the Structured Clinical Interview for DSM-IV). About 59% of the patients had previously used sildenafil, which improved erections in all of the patients. Sildenafil nonresponders were excluded from this study. During the study, the protocol was amended so that baseline entry-level criteria scores for the HAM-D decreased from 13–23 to 11–17. Consequently, 25% of the subjects were enrolled under the initial criteria, and as a result, <9% of the total patient group had HAM-D scores that were above the 11–17 range at baseline. Overall, the treatment groups were balanced with respect to these demographic and disease variables (Table 1).
Efficacy for Erectile Function
Erectile function domain scores
Vardenafil treatment resulted in statistically significant and clinically meaningful improvement in all erectile function parameters. A statistically significant difference in International Index of Erectile Function erectile function domain scores between the vardenafil-treated and placebo groups was seen at the 12-week endpoint and at the last observation carried forward (Figure 1). The International Index of Erectile Function domain scores for erectile function at the last observation carried forward showed a least squares mean improvement of 10.0 for vardenafil-treated subjects compared to 2.0 for the placebo group (t=8.78, df=215, p<0.0001). The results were similar for those who completed the treatment period. Other International Index of Erectile Function domain scores evaluating intercourse satisfaction (10.9 for vardenafil versus 7.8 for placebo) (t=7.43, df=214, p<0.0001), orgasmic function (7.7 versus 5.9) (t=4.93, df=214, p<0.0001), overall satisfaction (7.1 versus 4.9) (t=6.87, df=214, p<0.0001), and sexual desire (7.3 versus 6.4) (t=4.39, df=215, p<0.0001) all showed statistically significant differences between vardenafil- and placebo-treated patients (Table 2).
Diary measures
Question 2: vaginal penetration
The insertion success rate on the first attempt was approximately 1.5 times higher with vardenafil treatment than with placebo. If insertion was successful on the first attempt, the patients taking vardenafil were successful on approximately 89% of their subsequent attempts. Among patients who did not achieve insertion on the first attempt, the patients taking vardenafil were successful on approximately 49% of their subsequent attempts. A statistically significant difference in penetration rates between the vardenafil-treated and placebo groups was seen at the 12-week endpoint, at the last observation carried forward, and overall (Figure 1). Overall, the least squares mean penetration success rate in the vardenafil-treated group was 76.7% compared to 52.4% for the placebo-treated group (t=6.64, df=214, p<0.0001).
Question 3: erection maintenance to completion of intercourse
The success rate for maintaining an erection to completion of intercourse on the first medicated attempt was 1.8 times higher with vardenafil compared to placebo. If intercourse was completed successfully on the first attempt, the patients taking vardenafil were able to maintain their erection to successful completion on approximately 83% of their subsequent attempts. Among patients who were not able to successfully complete intercourse on their first attempt, the patients taking vardenafil were able to maintain their erection to successful completion on approximately 47% of their subsequent attempts. A statistically significant difference in intercourse success rates between the vardenafil-treated and placebo groups was seen at the 12-week endpoint, at the last observation carried forward, and overall (Figure 1). Overall, the least squares mean intercourse success rate was 66.4% with vardenafil treatment and 38.1% with placebo (t=7.40, df=214, p<0.0001). Overall, per-patient diary “yes” responses to questions concerning satisfaction with erection hardness (55.2% versus 25.0%) (t=7.40, df=214, p<0.0001) and sexual experience (60.0% versus 27.5%) (t=8.15, df=214, p<0.0001) also showed statistically significant efficacy in the vardenafil-treated group (Table 2).
Global assessment question
A statistically significantly greater proportion of vardenafil-treated patients responded “yes” to the global assessment question at the 12-week endpoint and at the last observation carried forward compared to the placebo-treated patients (Figure 1). At the last observation carried forward, the estimated rate of positive responses was 83% (N=130) for vardenafil and 30% (N=130) for placebo (χ2=51.96, df=1, p<0.0001).
Efficacy for Depression Variables
HAM-D overall score
Baseline HAM-D scores indicated mild major depressive disorder, with mean scores of 14.3 (SE=0.23) and 14.4 (SE=0.24) for placebo and vardenafil groups, respectively. The HAM-D total score at the last observation carried forward was only evaluated if the International Index of Erectile Function erectile function domain analysis was successful. The difference between vardenafil treatment and placebo was statistically significant at the last observation carried forward for the following HAM-D questions: question 1: depressed mood, question 2: feelings of guilt, question 4: early insomnia, question 5: middle insomnia, question 8: psychomotor retardation, question 10: psychic anxiety, and question 14: genital symptoms. HAM-D total scores showed statistically significant differences at week 12 (t=–4.12, df=182, p<0.0001) and at the last observation carried forward (t= –3.90, df=215, p=0.0001) (Figure 2). Least squares mean HAM-D scores at the last observation carried forward were 7.9 (SE=0.47) in the vardenafil-treated group versus 10.1 (SE=0.45) with placebo and were similar for patients who completed treatment.
HAM-D remission, treatment response, and treatment improvement rates
A decrease to a total score of 7 points or less in HAM-D total score was considered to be a complete remission of depressive symptoms (remitters). A positive response to treatment was defined as a decrease in HAM-D total score ≥50% compared to baseline (responders), and treatment improvement was defined as a decrease >3.5 points (improvers). According to these criteria, a significant difference was observed in remission of depressive symptoms with vardenafil compared to placebo (75 of 130, 58%, versus 41 of 130, 32%) (χ2=17.99, df=1, p<0.0001) (Figure 2). A decrease of more than 3.5 points was achieved by approximately 1.4 times more patients in the vardenafil treatment condition than with placebo (94 of 130, 72%, versus 66 of 130, 51%). The decrease of at least 50% (responders) was achieved by almost twice as many patients in the vardenafil group as in the placebo group (72 of 130, 55%, versus 39 of 130, 30%). Results for patients in North America and Europe were similar for the two primary endpoints.
Other psychometric outcomes
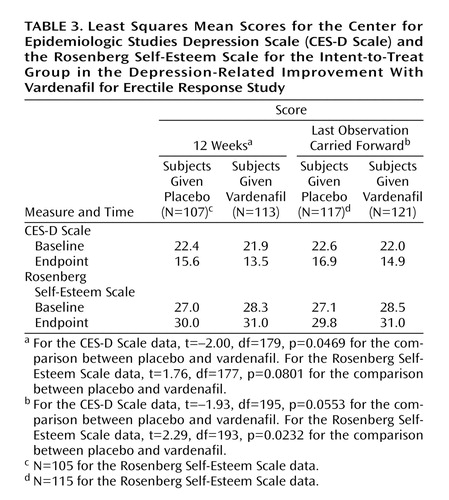
Other efficacy variables for depression showed improvements in depressive symptoms with vardenafil treatment compared to placebo. Improvements in depressive symptoms were evidenced by improvements in CES-D Scale ratings, with a statistically significant difference between placebo and vardenafil at week 12, with least squares mean scores of 13.5 (SE=0.86) for the vardenafil-treated group and 15.6 (SE=0.88) for the placebo group (t=–2.00, df=179, p=0.0469). Baseline scores were 21.9 (SE=0.83) and 22.4 (SE=0.85) for the vardenafil and placebo groups, respectively, indicating depressive symptoms. The Rosenberg Self-Esteem Scale showed a statistically significant difference between the least squares mean total score for vardenafil (31.0, SE=0.43) and placebo (29.8, SE=0.43) at the last observation carried forward (t=2.29, df=193, p=0.0232) but not at week 12 (p<0.09) (Table 3).
Correlation between improvement in erectile function and depressive symptoms
The association between changes in sexual function and depression status was examined, and a positive correlation between remission of depression and normalization of erection was observed. A return to normal was considered to be an International Index of Erectile Function erectile function domain score ≥26 and a HAM-D score ≤7 (remitters); 38% of vardenafil-treated subjects versus 13% of subjects in the placebo group showed a return to normal according to both criteria (χ2=21.90, df=1, p<0.0001). Patients treated with vardenafil or in the placebo group who achieved normal erectile function (International Index of Erectile Function erectile function domain score ≥26) had a mean HAM-D total score of 6.4 (SE=0.52) after treatment compared to 10.3 (SE=0.40) for those who failed to achieve a normalization of erectile function.
Predictors of normalization of erection and depression remission
Results of stepwise logistic regression analyses revealed that treatment with vardenafil was the most significant predictor of erection normalization (International Index of Erectile Function erectile function domain score ≥26). In descending order of importance, other significant predictors included a reduction in HAM-D score, a higher baseline International Index of Erectile Function erectile function domain score, a shorter erectile dysfunction duration, and younger age (Table 4). The most significant predictor of a normalization of depressive symptoms, as measured by HAM-D total score, was improvement in the International Index of Erectile Function erectile function domain score, followed by the International Index of Erectile Function erectile function domain baseline score and the HAM-D score at baseline (Table 4).
Safety
Vardenafil was generally well tolerated by this patient group. The most frequently reported adverse events included headache, nasal congestion, and flushing (Table 5), events consistent with the mechanism of action of agents of the PDE-5 inhibitor class. Symptoms were mild to moderate and transient in nature.
No placebo patients and one vardenafil-treated patient reported severe adverse events; this patient reported severe depression that was considered unrelated to study medication. There were no treatment-related psychiatric events and no deaths during the study. The overall rate of adverse events leading to discontinuation of study drug was <1% in the placebo group compared to 3% in the patients receiving vardenafil. No single adverse event led to discontinuation of the study drug in more than one patient per treatment group.
Discussion
A strong association has been observed among erectile dysfunction, overall lack of life satisfaction, and symptoms of depression (18–21). Improvements in life satisfaction may result from positive changes in self-confidence, mood, and family and sexual relationships, and improved erectile function in men with erectile dysfunction may play a decisive role in the complex network of factors that contribute to overall quality of life (22). The results presented here strongly support the hypothesis that improvements in sexual function in men with erectile dysfunction are associated with a lessening of depressive symptoms, which may have clinical implications for the management of a broad population of men with mild depression who may also suffer from erectile dysfunction.
Although previous studies have demonstrated the benefits of PDE-5 inhibitor therapy in men with both treated (7–10) and untreated symptoms of depression (6), this study is the first, to our knowledge, to evaluate PDE-5 inhibitor therapy for erectile dysfunction in men with untreated mild major depressive disorder. A robust and clinically significant improvement in essentially all sexual function variables was seen after active treatment, and vardenafil administration was also associated with a marked reduction in depressive symptoms. More than half of the patients receiving vardenafil achieved depressive symptom remission according to the usual severity criteria (HAM-D ≤7), supporting the clinical significance of the results. In addition, treatment with vardenafil resulted in improvements in CES-D Scale and Rosenberg Self-Esteem Scale scores relative to placebo. Thus, improvements in all depression efficacy variables were consistent, regardless of the outcome variable or type of measure employed.
The correlation between improvement in erectile dysfunction and HAM-D score remission provides further evidence that treatment of sexual dysfunction in these patients can affect other areas of patient function. The subjects treated with vardenafil were more likely to achieve normalization of erection than those treated with placebo, as would be expected from treatment with a PDE-5 inhibitor. Notable, however, was that improvement in HAM-D scores was a significant predictor of normalization of erectile function. This study also showed that improvement in erectile function was the most significant predictor of depression remission, followed in significance by the International Index of Erectile Function erectile function domain baseline and the HAM-D baseline scores. These results have important implications for the treatment of erectile dysfunction in patients with comorbid depression and support the concept that reducing residual symptoms, such as erectile dysfunction, may result in a more robust recovery from major depression.
These results also extend the body of literature in which PDE-5 inhibition has been shown to improve erectile dysfunction in patients with subsyndromal (6) or treated major depression (7, 8, 10). The study group investigated in the present study is unique in that it consisted of subjects with untreated mild major depressive disorder. Such patients may not use health care resources to the same extent as patients with more severe depressive symptoms and may therefore represent a larger group than that evaluated in previous studies (6). Because subjects were untreated for depressive illness, there were no confounding factors associated with pharmacologically induced sexual dysfunction (3, 5). Despite concerns at the outset of the study about potential psychiatric safety issues, it is noteworthy that no increases were observed in serious adverse events—either medical or psychiatric—during the course of the study. These results suggest that erectile dysfunction therapy could be offered to all male patients with comorbid depression, regardless of their depression treatment status. For patients with mild or subsyndromal depression, erectile dysfunction therapy may be undertaken prior to, or in conjunction with, antidepressant therapy. PDE-5 inhibitors may also be used in combination with antidepressant therapy in patients with more severe depression (10).
Vardenafil was well tolerated in this study, with few discontinuations due to adverse events. Similar low adverse event rates were observed in other flexible-dose studies conducted with vardenafil (23). Collectively, these results demonstrate that when vardenafil is used in accordance with product labeling (titration from the 10 mg/day starting dose), treatment with vardenafil for erectile dysfunction is easily optimized with respect to both efficacy and tolerability.
A limitation of this study is the relatively short duration of treatment (12 weeks). Further studies are needed to evaluate the durability or maintenance of change in both erectile dysfunction and depressive symptoms. Long-term studies with vardenafil demonstrate its efficacy and tolerability for up to 2 years in patients with erectile dysfunction and other comorbid medical conditions; however, there are no long-term studies of changes in depressive symptoms associated with erectile dysfunction therapy, to our knowledge. Additionally, the results of this study should not be generalized to patients with more severe depression, where primary therapy usually consists of antidepressive medication and/or psychotherapy. For patients suffering from both mild major depressive disorder and erectile dysfunction, concomitant use of serotonin reuptake inhibitors and PDE-5 inhibitors can be beneficial (10).
No attempt was made in the present study to determine the primacy or causal relationship between symptoms of erectile dysfunction and depression. The subjects were not queried as to whether their depressive symptoms preceded their erectile dysfunction or vice versa. The patients were diagnosed with erectile dysfunction and comorbid mild major depressive disorder, but the two syndromes may or may not have been causally related. It could be hypothesized that improvement in mood or quality of life improvement would have been greater in patients who identified erectile dysfunction as an important underlying factor in the genesis of their depression. The results presented here suggest that vardenafil treatment can improve depressive symptoms in men with comorbid erectile dysfunction and mild major depressive disorder, independent of whether erectile dysfunction was causally related to their depression. It is highly unlikely that vardenafil exerts direct antidepressant effects because it is not known to penetrate the blood-brain barrier. Improvement in symptoms of depression is more likely attributable to increased self-esteem and quality of life associated with improved sexual function and satisfaction with the partner, family, and relationship (22). This reinforces the concept that treatment of physical symptoms in depression can enhance treatment outcomes and overall quality of life and reduce the risk of relapse (22, 24, 25).
 |
 |
 |
 |
 |
Presented in part at the 14th European Association of Urology Congress in Vienna, March 24–27, 2004; an abstract was published in Eur Urol 2004; 3:235. Received Oct. 14, 2004; revision received Feb. 24, 2005; accepted April 13, 2005. From the Department of Psychiatry, University of Medicine and Dentistry of New Jersey–Robert Wood Johnson Medical School. Address correspondence and reprint requests to Dr. Rosen, Department of Psychiatry, UMDNJ–Robert Wood Johnson Medical School, 675 Hoes Lane, Piscataway, NJ 08854; [email protected] (e-mail). Funded by Bayer Healthcare Pharmaceuticals and GlaxoSmithKline. See the online version of this article for additional information on the Vardenafil Study Site Investigators.

Figure 1. Efficacy of Vardenafil for Erectile Dysfunction at 12-Week Endpoint, Last Observation Carried Forward, and Overall for Sexual Encounter Profile Questions 2 and 3 in the Depression-Related Improvement With Vardenafil for Erectile Response Studya
aSignificant difference between groups. Intent-to-treat group.

Figure 2. Efficacy of Vardenafil for Depression at 12-Week Endpoint and Last Observation Carried Forward in the Depression-Related Improvement With Vardenafil for Erectile Response Studya
aSignificant difference between groups. Intent-to-treat group.
1. Kessler RC, McGonagle KA, Swartz M, Blazer DG, Nelson CB: Sex and depression in the National Comorbidity Survey, I: lifetime prevalence, chronicity and recurrence. J Affect Disord 1993; 29:85–96Crossref, Medline, Google Scholar
2. Sadock BJ, Sadock VA (eds): Kaplan and Sadock’s Comprehensive Textbook of Psychiatry, 7th ed. Philadelphia, Lippincott Williams & Wilkins, 2000Google Scholar
3. Ferguson JM: The effects of antidepressants on sexual functioning in depressed patients: a review. J Clin Psychiatry 2001; 62(suppl 3):22-34Google Scholar
4. Araujo AB, Durante R, Feldman HA, Goldstein I, McKinlay JB: The relationship between depressive symptoms and male erectile dysfunction: cross-sectional results from the Massachusetts Male Aging Study. Psychosom Med 1998; 60:458–465Crossref, Medline, Google Scholar
5. Rosen RC, Marin H: Prevalence of antidepressant-associated erectile dysfunction. J Clin Psychiatry 2003; 64(suppl 10):5-10Google Scholar
6. Seidman SN, Roose SP, Menza MA, Shabsigh R, Rosen RC: Treatment of erectile dysfunction in men with depressive symptoms: results of a placebo-controlled trial with sildenafil citrate. Am J Psychiatry 2001; 158:1623–1630Link, Google Scholar
7. Nurnberg HG, Gelenberg A, Hargreave TB, Harrison WM, Siegel RL, Smith MD: Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001; 158:1926–1928Link, Google Scholar
8. Nurnberg HG, Hensley PL: Sildenafil citrate for the management of antidepressant-associated erectile dysfunction. J Clin Psychiatry 2003; 64(suppl 10):20-25Google Scholar
9. Labbate LA, Croft HA, Oleshansky MA: Antidepressant-related erectile dysfunction: management via avoidance, switching antidepressants, antidotes, and adaptation. J Clin Psychiatry 2003; 64(suppl 10):11-19Google Scholar
10. Nurnberg HG, Hensley PL, Gelenberg AJ, Fava M, Lauriello J, Paine S: Treatment of antidepressant-associated sexual dysfunction with sildenafil: a randomized controlled trial. JAMA 2003; 289:56–64Crossref, Medline, Google Scholar
11. Donatucci C, Eardley I, Buvat J, Gittleman M, Kell P, Segerson T, Homering M, Montorsi F, Vardenafil Study Group: Vardenafil improves erectile function in men with erectile dysfunction irrespective of disease severity and disease classification. J Sex Med 2004; 1:301–309Crossref, Medline, Google Scholar
12. Porst H, Young JM, Schmidt AC, Buvat J: Efficacy and tolerability of vardenafil for treatment of erectile dysfunction in patient subgroups. Urology 2003; 62:519–523Crossref, Medline, Google Scholar
13. National Institutes of Health Consensus Development Panel on Impotence: NIH consensus conference: impotence. JAMA 1993; 270:83–90Crossref, Medline, Google Scholar
14. Radloff LS: The CES-D Scale: a self-report depression scale for research in the general population. J Applied Psychol Measurement 1977; 1:385–401Crossref, Google Scholar
15. Cappelleri JC, Rosen RC, Smith MD, Mishra A, Osterloh IH: Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999; 54:346–351Crossref, Medline, Google Scholar
16. Rosenberg M: Society and the Adolescent Self-Image. Princeton, NJ, Princeton University Press, 1965Google Scholar
17. Sheehan DV, Lecrubier Y, Sheehan KH, Amorium P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC: The Mini International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998; 59(suppl 20)22-33Google Scholar
18. Shabsigh R, Klein LT, Seidman S, Kaplan SA, Lehrhoff BJ, Ritter JS: Increased incidence of depressive symptoms in men with erectile dysfunction. Urology 1998; 52:848–852Crossref, Medline, Google Scholar
19. Althof SE: Quality of life and erectile dysfunction. Urology 2002; 59:803–810Crossref, Medline, Google Scholar
20. Seidman SN: Exploring the relationship between depression and erectile dysfunction in aging men. J Clin Psychiatry 2002; 63(suppl 5):5-12Google Scholar
21. Seidman SN, Roose SP: Sexual dysfunction and depression. Curr Psychiatry Rep 2001; 3:202–208Crossref, Medline, Google Scholar
22. Rosen RC, Seidman SN, Menza MA, Shabsigh R, Roose SP, Tseng LJ, Orazem J, Siegel RL: Quality of life, mood, and sexual function: a path analytic model of treatment effects in men with erectile dysfunction and depressive symptoms. Int J Impot Res 2004; 16:334–340Crossref, Medline, Google Scholar
23. Hatzichristou D, Cuzin B, Martin-Morales A, Buvat J, Porst H, Laferriere N, Bandel TJ, Montorsi F, Vardenafil Study Group: Vardenafil improves satisfaction rates, depressive symptomatology, and self-confidence in a broad population of men with erectile dysfunction. J Sex Med 2005; 2:109–115Crossref, Medline, Google Scholar
24. Paykel ES: Remission and residual symptomatology in major depression. Psychopathology 1998; 31:5–14Crossref, Medline, Google Scholar
25. Sadovsky R: Integrating erectile dysfunction treatment into primary care practice. Am J Med 2000; 109(suppl 1):22-28Google Scholar

