
Gender Differences in Violent Behaviors: Relationship to Clinical Symptoms and Psychosocial Factors
Abstract
OBJECTIVE: Men are more violent than women in the general population, but this has not been found to be the case among psychiatric inpatients. The reason for this exception is poorly understood. The present study investigated gender differences in violent behaviors among patients with major psychiatric disorders. It examined various clinical symptoms and psychosocial factors to determine their differential impact on violence in men and women. METHOD: Physical assaults and verbal assaults committed by psychiatric inpatients were recorded prospectively. Patients whose violent incident occurred during their first 2 months of hospitalization were eligible for the study. Patient history of community violence was also obtained. Psychiatric symptoms and ward behaviors were assessed upon entry into the study and after 4 weeks. RESULTS: A similar percentage of women and men had an incident of physical assault in the hospital. Among the patients entered into the study, the women had a much higher level of verbal assaults throughout the evaluation period and a higher level of early physical assaults (i.e., within the first 10 days of the 4-week study period). Positive psychotic symptoms were more likely to result in assaults in women than in men. Physical assaults in the community, on the other hand, were more common in men and were associated with substance abuse, property crime, and a history of school truancy. CONCLUSIONS: There are gender differences in the patterns of violent behavior among patients with major psychiatric disorders. Furthermore, psychiatric symptoms and psychosocial risk factors have a different impact on this behavior in men and women. This has important implications for the prediction and differential treatment of violent behavior.
In the general population, men are more physically aggressive than women on numerous measures of aggression (1), including arrests for homicide and violent crimes (2). Several studies, however, have suggested that psychiatric disorders reduce the gender difference and in some cases eliminate it altogether. In studies of large unselected birth cohorts (3), the presence of major mental disorders increased the risk for violent offending in both men and women but relatively more so in the women. One study (4) assessed the prevalence of self-reported violent behavior over 1 year among adults living in the community. Among persons with no psychiatric disorder, violence was much greater in men than in women. This gender difference was much reduced among patients with major psychiatric disorders.
A more detailed analysis of violence was undertaken in one study (5). Male subjects had a greater prevalence of more serious violence involving weapons or injury in the 4 months preceding hospitalization, but there were no gender differences when measures of violence that were more inclusive (incorporating threats as well as fights not involving weapons or injuries) were used.
Male overrepresentation among violent patients disappears completely in studies of inpatient populations (6, 7). In one study (7), violence preceding hospital admission and during hospitalization were compared in the same patients. The men were more violent than the women in the 2 weeks before hospitalization, but women were more violent than men in the 3 days following admission.
In order to understand better the occurrence of violence in male and female patients, it is important to investigate clinical symptoms and psychosocial factors that accompany violence in these patients and to see how these factors vary in men and women. A positive relationship between violence and various positive psychotic symptoms has been repeatedly demonstrated in psychiatric patients (8, 9).
Various historical factors have been associated with increased community violence and antisocial behavior. These include substance abuse (10), nonviolent crime, and school truancy (11). These variables have also been associated with adult antisocial behavior and a diagnosis of DSM-IV antisocial personality disorder.
The present study investigated gender differences in various parameters of inpatient assaults and community violence and their association with psychiatric symptoms and historical variables.
Method
Subjects
The subjects were 18–55-year-old inpatients with major psychiatric illness in two psychiatric state hospitals. Patients with neurological illness or mental retardation were excluded from the study. These inclusion/exclusion criteria were selected because the study focused on the relationship of violence to psychotic symptoms; 96% of the violent patients who met the other inclusion/exclusion criteria had a DSM-III-R diagnosis of schizophrenia, schizoaffective disorder, or bipolar disorder, and the study was therefore further limited to these three diagnoses for greater homogeneity. Diagnosis was established through the Structured Clinical Interview for DSM-III-R (SCID) (12).
Patients with an incident of physical assault during their first 2 months of hospitalization were eligible for the study. After complete description of the study to the subjects, written informed consent was obtained.
Study Design and Evaluations
The subjects received an initial evaluation of psychiatric symptoms and ward behaviors within 3 days of the first physical assault. They were then followed for 4 weeks; all physical and verbal assaults were recorded, and all administered medications were monitored. At the end of 4 weeks, psychiatric symptoms and ward behaviors were again assessed. Demographic and historical data, including history of psychiatric illness, drug/alcohol abuse, and head trauma, were obtained through patient interview and review of medical records.
To establish interrater reliability, joint rating sessions that included all raters were conducted before the study. Raters’ performance was tested by additional sessions; those who had an intraclass correlation coefficient (ICC) (13)—a measure of interrater reliability—of at least 0.80 participated in the study.
Measures
Assessment of violence
Inpatient assault for the purpose of this study was defined as actual physical contact (striking, kicking, pushing). These physical assaults were assessed on a prospective basis by two licensed research nurses through daily review of nursing reports (ward journals), patient charts, and interviews with ward staff present at the time of the incidents. These incidents were then recorded by using the Modified Overt Aggression Scale (14), which is based on the Overt Aggression Scale (15). Severity of assault is also recorded on this scale and varies from swinging at people all the way to serious injury. Verbal assaults, including curses, insults, and threats of violence, were also recorded. Raters were trained before the study. Interrater reliability, determined before the study with three raters, was high for both physical assaults (ICC=0.94) and verbal assaults (ICC=0.89).
We were interested in the frequency and course of physical and verbal assaults over the 4-week study period. In patients with two or more assaults, subsequent assaults often occurred in close chronological proximity to the first. They were clustered such that 50% of subsequent assaults occurred within 10 days of the first assault. On the basis of these data, we divided the 4 weeks into two periods, the first 10 days and the subsequent 18 days. In the subsequent text we refer to “early assaults” for those occurring during the first 10 days and “late assaults” for those in the subsequent 18 days.
Community violence was a discrete variable. Patients were classified as violent or nonviolent on the basis of presence or absence of physical assaults in the community, as obtained through patient interviews and chart reviews. This information contained also data on arrests and convictions for violent crimes committed in the community.
Psychiatric symptoms
The Brief Psychiatric Rating Scale (BPRS) (16) was used to evaluate psychiatric symptoms. It provides an assessment of positive psychotic symptoms through three of its subscales: psychosis/thought disturbance, activation, and hostility/suspiciousness. It includes also the anergia factor, which is highly correlated with overall measures of negative symptoms (17). The latter was therefore used as a measure of negative symptoms.
The BPRS was administered by research doctors who were blind to the extent of patients’ violence. The raters were instructed not to inquire about actual violence. The BPRS hostility item, therefore, was limited to an assessment of hostile attitude. ICCs for interrater reliability were obtained before the study; the range was between 0.87 and 0.98 for BPRS total score.
Ward behaviors
Three subscales from the Nurses’ Observation Scale for Inpatient Evaluation (NOSIE) (18) that assess behaviors relevant to the occurrence of assaults and do not overlap with the information obtained through the BPRS were administered. The “irritability,” “routine,” and “social” subscales assess, respectively, ability to control temper, compliance with ward routines and regulations, and social interest. The ICCs for interrater reliability were obtained before the study and were above 0.80 for all three subscales.
Data Analysis
The purpose of this study was to characterize the gender differences in various violent behaviors and to relate these to differences in symptoms and historical factors that are associated with violence.
Random regression hierarchical linear modeling (19) was used to assess longitudinally the gender differences in the total number of verbal and physical assaults over the 4-week period. Gender, time (first 10 days and subsequent 18 days), diagnosis, and their interactions were used as the independent variables.
Gender differences in clinical variables were investigated through hierarchical linear modeling. The relationship between inpatient assaults and the clinical variables and the impact of gender on this relationship were also investigated through hierarchical linear modeling. Frequency of assaults was the dependent variable. The independent variables included the clinical factor, gender, and the interaction between gender and the clinical factor. Similar to the above analyses for assaults, diagnosis and time were also introduced as additional independent variables. Diagnosis was introduced as a covariate. The focus of these analyses was on the interaction between gender and the clinical factors. When it was significant, least square means were calculated to interpret this interaction further.
We also investigated gender differences in historical variables. Because of the possibility that these results were confounded by diagnosis, we conducted a multivariate logistic regression analysis in which the relationship between gender and the historical variables was investigated using diagnosis as a covariate. Odds ratios were used to characterize the effect size of each association.
In addition to the main analyses, which were conducted for patients with incidents of physical assault over a 4-year period, we gathered information about the general hospital population over a 30-month period (the first 30 months of this 4-year study) in order to assess gender differences in the ratio of violent to nonviolent patients in the hospital. We obtained basic demographic and diagnostic information on all hospital admissions over this 30-month period. Chart diagnosis was used for these analyses, since the SCID diagnosis was not available for the overall hospital population.
Results
Gender Differences in Violence in the General Hospital Population
For the first 30 months of this 4-year study, we gathered information on all hospital admissions. There were 1,487 patients (459 women and 1,028 men) who met the inclusion criteria for the study. Of these, 189 patients (64 women and 125 men) engaged in one or more physical assaults during their first 2 months of hospitalization. The percentage of violent women (13.9%) in the hospital was similar to that of the violent men (12.2%).
We compared the violent and the nonviolent patients with regard to other demographic and diagnostic characteristics. The groups did not differ in ethnic background. The violent patients were younger than the nonviolent patients (mean age=33.0 years [SD=8.2] versus 36.5 years [SD=8.5], respectively; t=4.88, df=1486, p<0.0001). There was a significant difference in the number of patients who were violent in the different diagnostic categories based on chart diagnosis (χ2=5.36, df=2, p<0.05). There were more schizoaffective patients in the violent group relative to their number in the nonviolent hospital population. There was also a difference in the number of men and women in each diagnostic category, with more women in the schizoaffective and bipolar group and relatively fewer in the schizophrenia group. We conducted a multiple logistic regression analysis in which diagnosis was entered as a covariate; no difference was found in the proportion of violent male and female patients.
Overall Characteristics of the Violent Male and Female Patients
Over the 4-year duration of the study, 253 patients (174 men and 79 women) were eligible for the study. These patients had committed a physical assault during their first 2 months of hospitalization and met the inclusion criteria. Seven of these refused to participate, while 246 provided informed consent and underwent the initial evaluation within 3 days of the first incident. Of these, 24 did not complete the 4-week study period. Therefore, there were 222 patients (155 men and 67 women) who completed the 4-week study period with all evaluations. These 222 patients were used in the final data analyses reported here. They did not differ in demographic characteristics or diagnosis from the 31 patients who were not included in these analyses. There were no significant differences in violence between these two groups.
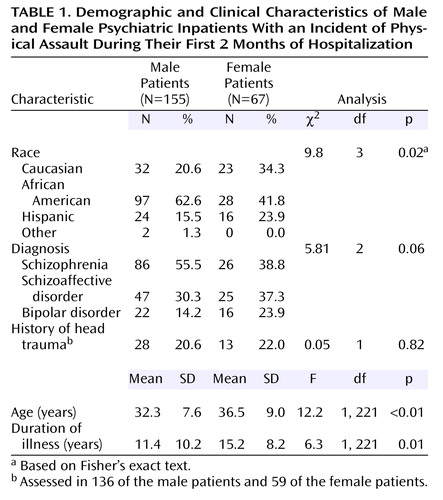
Table 1 shows the demographic, diagnostic, and other characteristics of the men and the women in the final sample. The men and women differed significantly in ethnic background, age, and duration of illness. The women were older and had a longer duration of illness. There were proportionately more African Americans in the male than in the female group. There was a marginal difference in diagnosis, with proportionately more women diagnosed with schizoaffective disorder and bipolar disorder than with schizophrenia. We entered these variables in the various analyses; the inclusion of age, duration of illness, and ethnic background did not have an impact on the results; diagnosis, however, did affect the results and was therefore entered as a covariate in all analyses.
There were no gender differences in head trauma. The average antipsychotic daily doses (in chlorpromazine equivalents) for the first and last weeks of the study were also calculated; there were no significant gender differences.
Gender Differences in Violent Behaviors
Gender differences in the frequency and course of physical and verbal assaults over the 4-week period were analyzed through hierarchical linear modeling (with diagnosis as a covariate). ANCOVA was then used to compare the number of assaults in men and women cross-sectionally during the two time periods. The number of inpatient assaults in the early and late periods is indicated in Table 2.
Women tended to have a higher total number of physical assaults than the men during the 4-week period (F=3.45, df=1, 217, p=0.06). There was a statistically significant interaction between gender and change in physical assaults (F=5.20, df=1, 217, p=0.02), with a greater decrease in physical assaults for the women than for the men. Actual gender comparisons for the two time periods indicate that the women had significantly more physical assaults in the early period but not in the late period, where there was no difference (Table 2).
Similar to the physical assaults, the total number of verbal assaults was higher in women than in men during the 4 weeks (F=12.98, df=1, 217, p<0.001). There was also a statistically significant interaction between gender and change in verbal assaults over the 4 weeks (F=3.93, df=1, 217, p<0.05), with a greater decrease for the women. ANCOVA indicated that the women presented with significantly more verbal assaults than the men both in the early period and in the late period (Table 2).
There were gender differences in the severity of inpatient physical assaults. A higher proportion of men than women inflicted physical injury to their victim (i.e., assaults that were rated as “3” or higher on the Modified Overt Aggression Scale) (Table 2).
History of physical assaults in the community was evaluated as a discrete variable (presence or absence of such assaults). As indicated in Table 2, a significantly higher proportion of men (41%) than women (25%) were physically assaultive in the community. Six of the patients committed homicides; they were all men.
Clinical Differences in Violent Behaviors
There were no significant overall gender differences in BPRS positive or negative symptom scores or in NOSIE subscale scores.
Physical assaults and clinical symptoms
In both men and women, frequency of physical assaults was related to BPRS positive symptom score (F=5.39, df=1, 216, p=0.02). It was also related to the NOSIE irritability (F=11.42, df=1, 199, p<0.01), routine (F=20.17, df=1, 199, p<0.01), and social (F=8.22, df=1, 199, p<0.01) subscale scores, indicating that greater impairment on these scales was associated with a greater number of physical assaults.
There were no significant interactions between gender and BPRS factors in determining physical assaults. There was, however, a significant interaction between gender and score on the NOSIE routine subscale (F=3.92, df=1, 199, p<0.05), indicating that the impact of routine on physical assaults differed in men and women. There was also a tendency for gender to interact with score on the NOSIE social subscale (F=3.54, df=1, 199, p=0.06).
In order to interpret the direction of these two interactions, we computed least square means. At high impairment on the routine subscale, the women had much higher physical assaults than the men, whereas at low impairment, there were only small gender differences. Similar results were obtained for the NOSIE social subscale. Thus, impairments in the ability to follow ward routines and in social interactions are more likely to result in physical assaults in the women than in the men.
Verbal assaults and clinical symptoms
In both men and women, frequency of verbal assaults was related to positive symptom score (F=52.72, df=1, 216, p<0.01) and negative (BPRS anergia factor) symptom score (F=9.71, df=1, 216, p<0.01). Frequency of verbal assaults was also related to scores on the NOSIE irritability (F=50.79, df=1, 199, p<0.01), routine (F=27.60, df=1, 199, p<0.01), and social (F=4.08, df=1, 199, p=0.04) subscales, indicating that a greater impairment on these clinical scales was associated with a greater total number of verbal assaults.
For the verbal assaults, there was a significant interaction between positive symptoms and gender (F=6.85, df=1, 216, p=0.01). There were also significant interactions between gender and scores on the NOSIE irritability (F=17.48, df=1, 199, p<0.001), routine (F=12.36, df=1, 199, p<0.001) and social (F=6.91, df=1, 199, p<0.01) subscales.
The aforementioned clinical variables had a different impact on verbal assaults for women than for men. Similar to the analyses for physical assaults, the interactions between gender and these variables in determining verbal assaults were further interpreted through least square means. When these symptoms were more severe, the women were more verbally aggressive than were the men, whereas when the symptoms were not severe, there were essentially no gender differences in verbal assaults.
Course of inpatient physical assaults in men and women
In order to understand better the high level of physical assaults among women in the early period and its rapid decrease over time, we integrated the data in a multivariate model that allowed us to identify complex relationships among variable sets. First, canonical correlation analysis was performed in order to investigate the relative importance of clinical symptom configurations in relation to particular patterns of violent behaviors. This method can be thought of as extension of factor analysis for two sets of variables. Its objective is to obtain as high a correlation as possible between the two sets of variables (factors). This technique is an optimal linear method for studying interset associations: components (factors) from the two sets are extracted jointly in a way maximizing the correlation between the components. In our study, the two sets of variables that were used comprised the violence parameters and the clinical symptoms. The violence parameters consisted of early and late physical assaults as well as change in assaults over time. The clinical symptoms included baseline and endpoint measures of positive symptoms (BPRS psychosis/conceptual disorganization, activation, and hostility/suspiciousness) and negative symptoms (BPRS anergia).
Second, an additional analysis was performed to investigate how men differed from women in terms of the relationship between the basic dimensions of violence and the basic clinical correlates (identified through the canonical correlation analyses).
Canonical correlation analyses assessed the degree of association between the violence parameters and the clinical measures. The three violence parameters formed one side of the model, and the measures of positive and negative symptoms formed the other side.
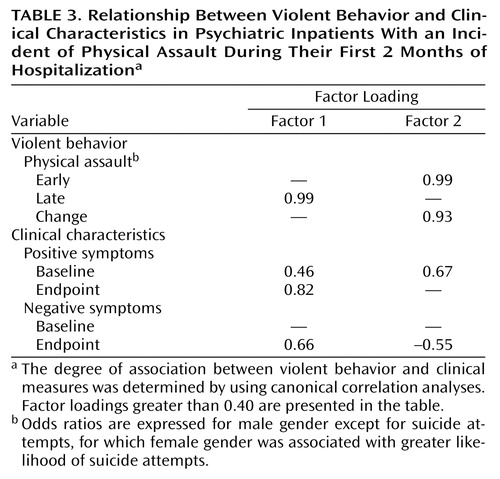
Two significant dimensions (canonical factors) of inpatient physical assaults were identified in relation to clinical symptoms (Table 3).
As indicated by the canonical factor loadings, the first dimension (canonical factor 1) was characterized by late physical assaults and represents a more persistent form of violence associated with more enduring symptoms; it was positively related to both endpoint positive and negative psychotic symptoms. The second dimension (canonical factor 2) was characterized by early physical assaults and marked decrease in assaults over time. It was positively associated with early positive symptoms and negatively with late negative symptoms. Thus, it represents a transient form of violence that is accompanied by remitting positive symptoms and absence of enduring negative symptoms.
We looked at the difference in the above dimensions of violence (canonical factors) as a function of gender. There was no gender difference for the first dimension, but women had a significantly higher value than the men on the second dimension (F=6.14, df=1, 208, p=0.01). Thus, this early and remitting violence, which is strongly influenced by the symptom configuration of acute positive psychotic symptoms and absence of enduring negative symptoms, is more prominent in the women than in the men.
Psychosocial Factors
In the literature, factors such as drug abuse, school truancy, and property crime were related to community violence. We examined the relationship of these factors to community violence in our sample. We also investigated the contribution of gender to the risk factor with diagnosis as a covariate. Community violence was significantly related to substance abuse (odds ratio=2.2, 95% confidence interval [CI]=1.04–4.7; Wald χ2=4.2, df=1, p=0.04), theft and property crime (odds ratio=4.8, CI=2.4–10.0; Wald χ2=18.4, df=1, p<0.001), and to school truancy in childhood (odds ratio=2.9, CI=1.6–5.5; Wald χ2=11.4, df=1, p<0.001). There was no relationship, however, between community violence and a history of suicide attempts.
There were significant gender differences in these psychosocial factors (Table 4). The men had a higher prevalence of substance abuse, theft and property crime, and school truancy in childhood than the women. The women, on the other hand, had a higher prevalence of suicide attempts than the men (Table 4).
Discussion
Violent Behaviors in Patients With Major Psychiatric Disorders
In order to understand better gender differences in violence, we must take into consideration the complexity of the phenomenon and differentiate among its multiple manifestations. It is important, for example, to distinguish between physical and verbal assaults. The finding in our study that the women were more verbally abusive and threatening than the men throughout the 4 weeks is consistent with the predominance of verbal aggression reported in women (1). In the general population, women, throughout life, are more likely to use verbal than physical aggression (20, 21).
The contrast between men and women in physical assaults is more intricate. Gender differences in physical assaults vary depending on their severity, course, and setting (i.e., hospital versus community). The ratio of violent to nonviolent patients in the overall hospital population, as defined by presence of one or more physical assaults, was the same in both genders. This is consistent with the studies mentioned above that report that women are as violent as men in inpatient settings (6, 7).
Patients with an incident of physical assault were followed for 4 weeks. The women had a higher frequency of early physical assaults (i.e., during the first 10 days of the study period), with marked reduction subsequently, such that the number of assaults in the later period was similar to the men. A higher ratio of men than women, however, perpetrated assaults that resulted in injury. Our results correspond to those of the aforementioned study (5) in which male patients had a greater prevalence of more severe violence. A meta-analytic review of studies on gender differences in the general population (21) also indicated that the male overrepresentation in aggression is more pronounced for severe physical aggression.
There was a higher ratio of men than women who had a history of physical assaults in the community. Thus, the same women who had a higher frequency of assaults than the men early in the course of their hospitalization were not as assaultive as the men in the community. These results are consistent with the report that the higher rate of physical assaults in men before hospitalization is reversed early on during hospitalization (7).
Clinical Correlates of Assaults
Several previous studies have found positive symptoms to be associated with violence in psychiatric patients (8, 9). This was the case in our study as well. Positive psychotic symptoms and behavioral disturbances were associated with higher frequency of assaults in both men and women.
There were no overall gender differences in psychotic symptoms or ward behaviors; the gender differences in violent behavior, therefore, could not be attributed to more severe symptoms. There were, however, gender differences in the degree of association between clinical symptoms and violence. When certain symptoms were present, women were more prone to become aggressive than men. Thus, difficulties in following ward regulations and social impairments were more likely to result in physical assaults in the women. This gender difference in the impact of symptoms on violent behavior was greater for verbal aggression. Severe positive psychotic symptoms, irritability, and difficulties with ward routines and with social interactions were strongly associated with verbal aggression in the women but not in the men.
In order to understand better the high frequency of physical assaults in the women early on and its subsequent decrease over time, we investigated early and late assaults in relation to early and late psychotic symptoms. A transient type of violence, which was strongly associated with early remitting positive psychotic symptoms and negatively related to enduring negative symptoms, was more characteristic of the women than of the men.
Psychosocial Risk Factors
Various psychosocial variables associated with community violence in the literature were related to this variable in our study as well. We also found gender differences in these variables. A higher proportion of men than women presented with a history of school truancy, nonviolent property crime, and substance abuse. These problems are often indicative of antisocial predispositions and these, then, appear to be stronger in men than women. The higher incidence of physical violence in the community in men may be indicative of their more pervasive antisocial tendencies.
In summary, there is an overlap in the expression of violence and in the factors that contribute to its emergence in men and women; psychotic symptoms and behavioral disturbances play an important role for both genders. Yet, these symptoms interact with other predispositions that vary according to gender. In women, a transient flare up in physical violence may be indicative of high arousal and excitation associated with acute psychotic symptoms. In men, acute symptoms play a lesser role in the emergence of violence, but psychotic symptoms may enhance more chronic predispositions to violence that reflect in part antisocial tendencies.
Limitations and Conclusions
One limitation of this study is the retrospective investigation of community violence. This selects for more salient violent acts, since more severe physical assaults or incidents that resulted in arrest are more likely to be reported. A prospective longitudinal design would allow for a better investigation of the gender differences. Another limitation is the lack of information about some parameters that are important in the study of gender differences, such as possible hormonal influences, which could explain the more time-limited physical assaults in women.
Strengths of the study include a large sample size, a prospective study of the inpatient assaults, measures of violence and clinical symptoms that have demonstrated good reliability, and a multidimensional assessment of violence. This study also investigated possible mechanisms for the gender differences. Earlier studies did not examine the relationship between the gender differences and underlying clinical and historical factors.
 |
 |
 |
 |
Received Nov. 15, 2002; revision received Aug. 5, 2003; accepted Aug. 11, 2003. From the Nathan Kline Institute for Psychiatric Research and the Department of Psychiatry, New York University School of Medicine, New York. Address reprint requests to Dr. Krakowski, Nathan Kline Institute for Psychiatric Research, 140 Old Orangeburg Rd., Building 35, Orangeburg, NY 10962. Supported by NIMH grant MH-58341. The authors thank Henry Glickman, Ph.D., for critical comments that improved this report and also thank the staff and administration at the Rockland and Manhattan Psychiatric Centers for their help with this project.
1. Maccoby EE, Jacklin CN: The Psychology of Sex Differences. Stanford, Calif, Stanford University Press, 1974Google Scholar
2. Pastore AL, Maguire K (eds): Sourcebook of Criminal Justice Statistics, 1999. http://www.albany.edu/sourcebook/Google Scholar
3. Hodgins S: Mental disorder, intellectual deficiency and crime: evidence from a birth cohort. Arch Gen Psychiatry 1992; 49:476–483Crossref, Medline, Google Scholar
4. Swanson J, Holzer C, Ganju V: Violence and psychiatric disorder in the community: evidence from the Epidemiological Catchment Area Survey. Hosp Community Psychiatry 1990; 41:761–770Abstract, Google Scholar
5. Hiday VA, Swartz MS, Swanson JW, Borum R, Wagner HR: Male-female differences in the setting and construction of violence among people with severe mental illness. Soc Psychiatry Psychiatr Epidemiol 1998; 33(suppl 1):S68-S74Google Scholar
6. Lam JN, McNiel DE, Binder RL: The relationship between patients’ gender and violence leading to staff injuries. Psychiatr Serv 2000; 51:1167–1170Link, Google Scholar
7. Binder RL, McNiel DE: The relationship of gender to violent behavior in acutely disturbed psychiatric patients. J Clin Psychiatry 1990; 51:110–114Medline, Google Scholar
8. McNiel DE, Binder RL: The relationship between acute psychiatric symptoms, diagnosis, and short-term risk of violence. Hosp Community Psychiatry 1994; 45:133–137Abstract, Google Scholar
9. Tardiff K, Sweillam A: Assault, suicide and mental illness. Arch Gen Psychiatry 1980; 37:164–169Crossref, Medline, Google Scholar
10. Steadman HJ, Mulvey EP, Monahan J, Clark Robbins P, Appelbaum PS, Grisso T, Roth LH, Silver E: Violence by people discharged from acute psychiatric inpatient facilities and by others in the same neighborhoods. Arch Gen Psychiatry 1998; 55:393–401Crossref, Medline, Google Scholar
11. Berg I: When truants and school refusers grow up. Br J Psychiatry 1982; 141:208–210Crossref, Medline, Google Scholar
12. Spitzer RL, Williams JBW, Gibbon M, First MB: Structured Clinical Interview for DSM-III-R—Patient Version (SCID-P). New York, New York State Psychiatric Institute, Biometrics Research, 1990Google Scholar
13. Bartko JJ, Carpenter WT: On the methods and theory of reliability. J Nerv Ment Dis 1976; 163:307–317Crossref, Medline, Google Scholar
14. Kay S, Wolkenfeld F, Murrill L: Profiles of aggression among psychiatric patients, I: nature and prevalence. J Nerv Ment Dis 1988; 176:539–546Crossref, Medline, Google Scholar
15. Yudofsky SC, Silver JM, Jackson W, Endicott J, Williams D: The Overt Aggression Scale for the objective rating of verbal and physical aggression. Am J Psychiatry 1986; 143:35–39Link, Google Scholar
16. Overall JE, Gorham DR: The Brief Psychiatric Rating Scale. Psychol Rep 1962; 10:799–812Crossref, Google Scholar
17. Czobor P, Bitter I, Volavka J: Relationship between the Brief Psychiatric Rating Scale and the Scale for the Assessment of Negative Symptoms: a study of their correlation and redundancy. Psychiatry Res 1991; 36:129–139Crossref, Medline, Google Scholar
18. Honigfeld G, Klett CJ: The Nurses’ Observation Scale for Inpatient Evaluation: a new scale for measuring improvement in chronic schizophrenia. J Clin Psychol 1965; 21:65–71Crossref, Medline, Google Scholar
19. Bryk AS, Raudenbush SW: Hierarchical Linear Models: Applications and Data Analysis Methods. Newbury Park, Calif, Sage Publications, 1992Google Scholar
20. Crick NR, Grotpeter JK: Relational aggression, gender, and social-psychological adjustment. Child Dev 1995; 66:710–722Crossref, Medline, Google Scholar
21. Eagly AH, Steffen VJ: Gender and aggressive behavior: a meta-analytic review of the social psychological literature. Psychol Bull 1996; 100:309–330Crossref, Google Scholar

