
Clozapine-Induced Lymphocytic Alveolitis
To the Editor: Drug-induced lung disease is often nonspecific and represents a diagnostic challenge. We present the rare case of pulmonary toxicity associated with clozapine in a patient with a history of psychiatric illness.
“Mrs. A” was a 41-year-old, Hispanic woman with a history of schizoaffective disorder who was transferred from the psychiatric ward to medical service for evaluation of pulmonary infiltrates. Chest x-ray (Figure 1) and chest computerized tomography (CT) showed diffuse bilateral ground-glass opacities (Figure 2). The patient complained of only mild dyspnea and was able to ambulate without difficulty. She had no cough, chest pain, fever, or chills. She denied any sick contacts or environmental exposures and had stopped smoking several months prior. Her physical examination was unremarkable, and oxygen saturation on room air was 95%.
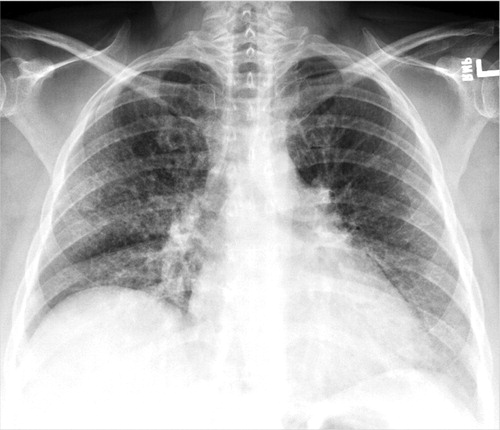

aThe images depict diffuse bilateral ground-glass opacities (A) and confirmed resolution of infiltrates (B).
The patient had a medical history of diabetes, hypertension, and hypothyroidism. Her medications included clozapine, oxcarbazepine, atorvastatin, metformin, and levothyroxine. Two months prior, she had an episode of refractory psychosis and was initiated on clozapine and titrated to a dose of 650 mg/day.
Laboratory data revealed thrombocytosis (689 × 103/μl), elevated liver function (aspartate transaminase level: 75 U/l; alanine transaminase level: 103 U/l), and an increased erythrocyte sedimentation rate (130 mm per hour). There was no peripheral eosinophilia. Rheumatologic serologies and urine toxicology findings were negative, and echocardiogram results were normal. The patient was unable to provide reliable pulmonary function data.
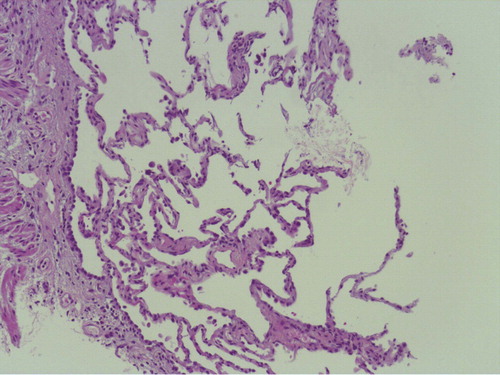
Bronchoalveolar lavage and lung biopsies were performed. Bronchoalveolar lavage showed a predominance of lymphocytes at 54% and eosinophils at 2%. Flow cytometry demonstrated a cluster of differentiation (CD)4/CD8 cell ratio of 0.7. Viral, bacterial, and mycobacterial cultures were negative. Lung biopsies revealed mild chronic inflammation without granulomas (Figure 3).
As a result of the temporal relationship between the initiation of clozapine and abnormal pulmonary findings and the absence of alternative diagnoses, a presumptive diagnosis of clozapine-induced pulmonary toxicity (lymphocytic alveolitis) was made. Clozapine was tapered and discontinued. There were no other changes made to the patient's medication regimen, and she did not receive antibiotics. Two months after discontinuation of clozapine, a repeat chest CT confirmed resolution of infiltrates (Figure 2).
The diagnosis of drug-induced lung disease is dependent upon the following three main elements: 1) appropriate temporal relationship between exposure and clinical presentation, 2) exclusion of other etiologies, and 3) resolution after drug withdrawal. In the present case, clozapine was the most recent drug exposure. We did not identify any environmental exposures, infections, or rheumatologic processes that could account for the patient's infiltrates. Finally, these infiltrates resolved after clozapine was discontinued.
There is only one other report, to our knowledge, of extrinsic alveolitis attributed to clozapine (1), and important similarities between our patient and the patient in the other case report are worth mentioning. In both cases, the patients are described as relatively well appearing, without respiratory distress but with diffuse infiltrates on chest imaging and an elevated erythrocyte sedimentation rate. However, unlike the patient in the previously reported case, our patient did not have significant peripheral eosinophilia, which suggests that clozapine may cause alveolitis via more than one mechanism in susceptible individuals. Clinicians should consider clozapine-induced lymphocytic alveolitis in patients who develop pulmonary infiltrates while receiving clozapine treatment.
1. : Clozapine-induced extrinsic allergic alveolitis. Br J Psychiatry 1998; 173:440–441 Crossref, Medline, Google Scholar

