
Mental Disorders and Suicide Among Young Rural Chinese: A Case-Control Psychological Autopsy Study
Abstract
Objective
The authors examined the prevalence and distribution of mental disorders in rural Chinese 15–34 years of age who committed suicide. They hypothesized that mental illness is a risk factor for suicide in this population and that the prevalence of mental illness is lower in females than in males.
Method
In this case-control psychological autopsy study, face-to-face interviews were conducted to collect information from proxy informants for 392 suicide victims and 416 living comparison subjects. Five categories of DSM-IV mental disorders (mood disorders, schizophrenia and other psychotic disorders, substance use disorders, anxiety disorders, and other axis I disorders) at the time of death or interview were assessed using the Chinese version of the Structured Clinical Interview for DSM-IV. Sociodemographic variables, social support, and life events were also assessed.
Results
The prevalence of current mental illness was 48.0% for suicide victims and 3.8% for comparison subjects. Among suicide victims, mental illness was more prevalent in males than in females (55.1% compared with 39.3%). A strong association between mental illness and suicide was observed after adjustment for sociodemographic characteristics. Other risk factors included having a lower education level, not being currently married, having a lower level of social support, and having a history of recent and long-term life events. Additive interactions were observed between mental illness and lower level of social support.
Conclusions
Although mental illness is a strong risk factor for suicide, it is less prevalent among rural Chinese young people who committed suicide, particularly females, in comparison with other populations in China and in the West.
Suicide is an important public health and mental health problem in China. The recently released Report on Injury Prevention in China revealed suicide rates to be 22.6, 22.4, 22.1, 19.3 and 19.3 per 100,000 in 1995, 1998, 2000, 2003, and 2005, respectively (1). Empirical studies in recent years have reported several unique findings on the pattern of suicide in China compared with other countries, mainly Western countries. First, unlike in most other countries, Chinese women are as likely as, or more likely than, men to commit suicide (2–4). Second, consistent with findings in many Western countries, the suicide rate among older adults is the highest among all age groups in China, but another, smaller peak occurs in the 15- to 34-year-old age group (3). Third, the suicide rate in rural areas of China is three to five times higher than that in urban areas (2, 3, 5).
Mental health has been a major area in which suicide is investigated. In the West, over 90% of suicides are associated with mental illness (6–8). In China, it has been estimated that only about 30% of suicide victims had a psychiatric diagnosis listed in official death registry data (9). In a nationally representative psychological autopsy study (N=519), Phillips and colleagues (10) reported that 40% of suicide victims were diagnosed with depression, 7% with schizophrenia, and 7% with alcohol dependence. Other risk factors—which included depression, previous suicide attempt, acute and chronic stressful life events, and lower quality of life—were similar to those seen in the West (10). Zhang et al. (11) found that 76% of rural suicide victims (N=66) had a diagnosable mental illness. However, these studies added little information to our understanding of the high suicide risk among rural Chinese and the unique patterns of distribution of suicide across age and gender because of either the use of injury deaths as controls (10) or small sample size (11).
We demonstrated in previous work (12) that it is feasible to study suicide by using the psychological autopsy method in Chinese social and cultural environments and that instruments developed in the West are reliable and valid for use in China (13). In this study, we used established psychological autopsy methods and a case-control design to examine the prevalence of mental disorders in rural Chinese 15–34 years of age who committed suicide and to examine possible interactions among mental illness, social support, and life events in suicide. To the best of our knowledge, this is the first psychological autopsy study in this specific population using living comparison subjects in China.
Method
Sampling
Three provinces in China—Liaoning, Hunan, and Shandong—were chosen for the study. Sixteen rural counties were randomly selected from the three provinces (six from Liaoning, five from Hunan, and five from Shandong). In each county, suicide victims 15–34 years of age were consecutively enrolled in the study from October 2005 through June 2008. Similar numbers of comparison subjects living in the community were recruited in the same counties during approximately the same period.
For our study, all village doctors in the research areas were briefly trained on study procedures and were required to report suicidal deaths to local Centers for Disease Control and Prevention (CDCs). For suicidal deaths that were not recognized by any health agency, our mortality registry system allowed the village treasurers, who collect fees for each burial or cremation and are aware of all deaths in the village, to notify the county CDC. Whenever necessary, an investigation with the village board and villagers was conducted by the research team to try to ensure that no cases of suicide were missed.
We used the 2005 census database of the 16 counties to randomly select a living comparison subject in the same age range (i.e., 15–34 years) and county of residence for each suicide victim.
Measures
We used the Chinese version of the Structured Clinical Interview for DSM-IV (SCID) (14) to generate current diagnoses for both the suicide group and the comparison group. Diagnoses were made by psychiatrists on each team in consensus meetings during which all responses from each informant were presented by the nonpsychiatrist interviewers. Five categories of DSM-IV axis I diagnoses were covered: mood disorders, schizophrenia and other psychotic disorders, substance use disorders, anxiety disorders, and other axis I disorders (stress-related disorders, somatoform disorder, eating disorders, pathological gambling, and adjustment disorder). Diagnoses of personality disorders and mental disorders with onset in childhood and adolescence (e.g., conduct disorder) were not included. Multiple diagnoses were made if appropriate.
The 23-item Duke Social Support Index (15; possible scores range from 11 to 45) was used to measure social support, and Paykel's Interview for Recent Life Events (16) was used to measure life events. Twenty life events were added to the original 44 life events in the instrument, so that a total of 64 events were covered in the interview. Life events that occurred no more than 1 month before death or interview were defined as recent life events, and those that occurred more than 1 month before death or interview were defined as long-term life events. Both instruments were validated in our previous study (12).
Training of Interviewers
All interviewers were mental health or public health professionals and were intensively trained for 2 weeks on determination of manner of death, psychological autopsy methods, and administration of the study instruments by U.S. and Chinese experts before beginning data collection. The interrater reliability (kappa) of mental disorder diagnoses and other instruments ranged from 0.72 to 0.90 based on the ratings of all interviewers in three mock interviews conducted after training. A 1-week midterm training of all investigators from the three research sites was carried out in 2007.
Interviewing Procedures
For suicide victims, interviews with informants were scheduled between 2 and 6 months after the suicide incident; this timing was intended to reduce the impact of acute grief on the interview while minimizing recall bias. Interviews with informants for living comparison subjects were scheduled as soon as these participants and their informants were identified. Each informant was interviewed separately by one trained interviewer. The average time for each interview was 2.5 hours.
This study was approved by the institutional review boards of State University of New York College at Buffalo; Central South University, Hunan; Provincial Center for Disease Prevention and Control, Liaoning; and Shandong University, Shandong. The research nature of the interview and the background of the research project were explained to all interviewees, and informed consent forms detailing the rights of interviewees were read and signed by both parties prior to each interview.
Selection of Information Sources
For each suicide victim and each comparison subject, we tried to interview at least two informants. To obtain parallel data between the two groups, we also used proxy information from the comparison subjects. Those individuals who were most familiar with the subject's life and circumstances and were available and consented to participate were interviewed by the research team. Although target persons could be as young as 15 years of age, informants had to be 18 or older. Characteristics of the informants for both suicide victims and comparison subjects were noted in a standardized fashion, recording most recent contact, number of contacts in the past month and past year, number of years the informant has known the target, the informant's relationship with the target, and the informant's impression of their familiarity with the target. For both suicide victims and comparison subjects, the first informant was always a parent, a spouse, or another important family member, and the second informant was always a friend, coworker, or neighbor. Of all the informants and living comparison subjects we initially contacted, only four informants for suicide victims and six living comparison subjects refused to participate in the study. We replaced them by selecting another four informants and six living comparison subjects.
Where responses of two informants differed on demographic variables or life events, we relied on the answer provided by the informant who had the best access to the information. With regard to mental illness, we recorded a symptom as present if it was endorsed by either informant because the other informant may not have had an opportunity to observe the specific characteristic or behavior.
Statistical Analysis
Descriptive analyses, t tests, and chi-square tests were carried out to describe and compare the demographic characteristics, level of social support (total score on the Duke Social Support Index), and number of recent and long-term stressful life events of the suicide and comparison groups. Adjusted odds ratios and 95% confidence intervals (CIs) derived from multivariate logistic regressions indicated associations between suicide and risk factors. Years of formal school education were categorized into three groups: <7 years, 7–9 years, and >9 years. The family's annual income in yuan (renminbi) was categorized into three groups: ≤10,000 yuan, 10,001–19,999 yuan, and ≥20,000 yuan. (During the study period, the exchange rate was approximately 7 yuan to the U.S. dollar.) Marital status was dichotomized as "not currently married" and "currently married," with the former including never married, divorced, separated, or widowed and the latter including those who were currently married or involved in a living relationship. Recent life events were categorized into three groups based on the count: 0, 1, and ≥2; and long-term life events were similarly categorized into four groups: 0, 1, 2, and ≥3. Score on the Duke Social Support Index was categorized into three social support groups based on the 33rd and 66th percentiles among case and comparison subjects: scores <32, from 32 to 37, and >37.
An additive model was used to test interactions among mental illness, social support, and recent and long-term life events (17, 18). Interaction in epidemiology refers to the extent to which the joint effect of two risk factors on a disease differs from the independent effects of each of the factors. It was argued that interaction measured on the additive scale was better correlated with biological interaction than when measured on a multiplicative scale (19) and was more related to disease prevention and intervention (20). In our study, the interactions were measured by a synergy index (18, 19) with 95% CIs based on the method described by Andersson et al. (21). Statistically significant interaction was indicated if the synergy index was >1 and the 95% CI did not include 1.
Results
Characteristics of Case and Comparison Subjects
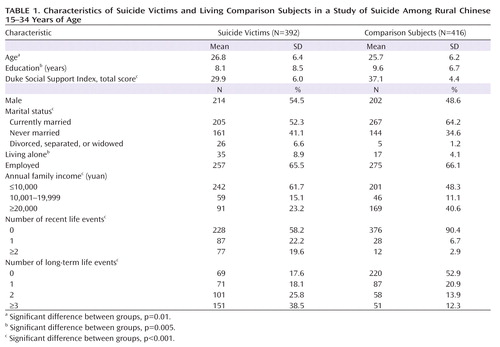
A total of 392 suicide victims and 416 living comparison subjects were enrolled in the study. No significant difference was observed in age distribution between comparison subjects and the 2005 Chinese national census data (p>0.05). The characteristics of case and comparison subjects are summarized in Table 1. Relative to comparison subjects, suicide victims were about 1 year older, were less educated, were less likely to be currently married, were more likely to live alone, and had lower income, less social support, and more recent and long-term stressful life events (all p values <0.05).
 |
Stressful Life Events
The most common recent stressful life events among suicide victims were fight with family members (N=38, 9.7%), fight with spouse/partner (N=34, 8.7%), and losing face (N=16, 4.1%); the most common long-term life events were financial difficulties (N=113, 28.8%), physical illness (N=88, 22.4%), and physical illness of a family member (N=59, 15.1%).
Diagnoses of Mental Disorders
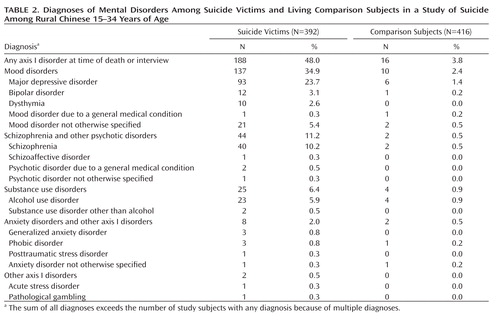
A total of 188 (48.0%) suicide victims and 16 (3.8%) comparison subjects met criteria for a diagnosis of at least one current mental disorder (Table 2); 29 suicide victims and two comparison subjects had two diagnoses. The most frequently diagnosed mental disorder category among suicide victims was mood disorders (34.9%), followed by psychotic disorders (11.2%) and substance use disorders (6.4%). Ninety-two suicide victims (23.5%) had a past history of mental illness, although of these, nine (9.8%) did not meet criteria for any current mental illness based on our SCID interview. History of past suicide attempt was significantly different between suicide victims with and without mental disorders (26.6% compared with 7.8%; χ2=24.57, p<0.001).
 |
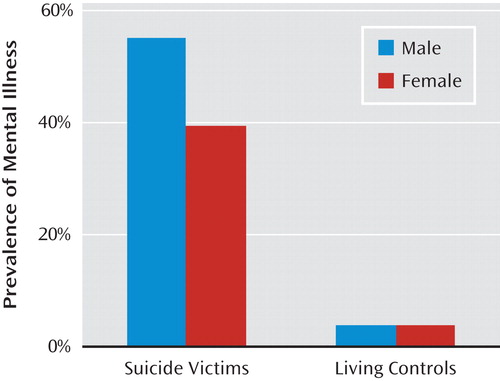
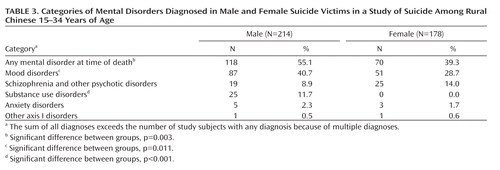
Among the suicide victims, 118 of 214 males (55.1%) and 70 of 178 females (39.3%) met diagnostic criteria for at least one mental disorder (Table 3, Figure 1). After other sociodemographic characteristics, social support, and stressful life events were controlled for in a logistic regression model, males were twice as likely as females to have a mental disorder diagnosis (odds ratio=2.06, 95% CI=1.26–3.36). The prevalence of mental illness in comparison subjects was 4.0% for males and 3.7% for females (Figure 1).
 |
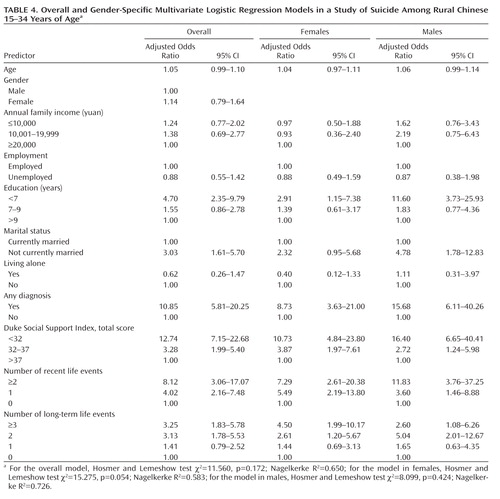
Overall and Gender-Specific Multivariate Logistic Regression Models
After adjustment for sociodemographic characteristics, social support, and life events in a logistic regression model, suicide victims were more than 10 times as likely as living comparison subjects to have a mental disorder diagnosis (odds ratio=10.85, 95% CI=5.81–20.25) (Table 4). Other risk factors included having a lower education level, not being currently married, having lower levels of social support, having one or more recent life events, and having two or more long-term stressful life events. After stratification by gender, the odds ratio of having any diagnosis of mental disorder was 8.73 (95% CI=3.63–21.00) in female suicide victims and 15.68 (95% CI=6.11–40.26) in male suicide victims (Table 4). Other risk factors were similar in both genders except that not being currently married was a risk factor in male but not female suicide victims.
 |
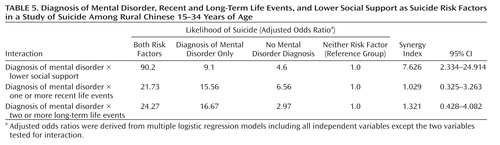
Interaction Among Mental Disorder Diagnoses, Social Support, and Life Events
To simplify interpretation of odd ratios, social support was dichotomized along the median for all case and comparison subjects, number of recent stressful life events was dichotomized as "0" and "at least 1," and number of long-term life events was dichotomized as "0 or 1" and "at least 2" because increased risk was observed only in those who experienced at least two long-term life events. As shown in Table 5, significant interaction was observed only between mental disorder diagnosis and lower social support (synergy index=7.626, 95% CI=2.334–24.914).
 |
Discussion
In this study, we used consecutive sampling to enroll suicide victims in 16 randomly selected counties in three provinces in China. Because there is no comprehensive vital reporting system in China, we relied mainly on village doctors and local CDC health professionals to identify eligible cases. To minimize false classifications or missed suicide cases, we trained village doctors in reliable determinations of manner of death and, where the case was ambiguous, arrived at consensus based on consideration of additional information from multiple resources, including village heads and village treasurers. Using these techniques, we identified 392 suicide victims over the 2.5-year study period.
Although suicide rates for women have been reported to be higher than those for men in rural China (3), a more recent estimate showed that the rural male-to-female ratio for suicide increased from 0.77 in 1991 to 0.94 in 2000 (2). Our study indicated that the suicide rate for men was slightly higher than that for women in this population. With the continuing improvement in quality of life in rural areas and increased opportunities for rural young women, including easier rural-urban migration in China, the male-to-female ratio for suicide may become closer to that in the West, although it would still be much lower.
The epidemiological assumption is that comparison subjects are representative of the general population in terms of probability of exposure (22). To optimize validity, we did not use accidental deaths for our comparison group because they might be biased in certain ways (e.g., a higher likelihood of substance misuse or impulsive, risk-taking behavior). The fact that proxy informants for comparison subjects were not affected by bereavement must, however, be taken into consideration in interpreting the results.
There was no significant difference in age or gender distributions between the comparison group and 2005 Chinese national census data, supporting the representativeness of comparison subjects in our study. Our results on the prevalences of mood disorders and psychotic disorders in our comparison group were comparable to those of previous studies in China, while the prevalences of alcohol use disorders and anxiety disorders were lower. For example, in a survey of 5,201 adults in Beijing and Shanghai, the authors reported a 1-year prevalence of 2.2% for mood disorders, 2.7% for any anxiety disorders, and 1.6% for alcohol abuse and dependence (23). In a large study (N=24,992), Hao and colleagues (24) reported a prevalence of current alcohol dependence of 3.8% in China. Our primary explanations for the lower prevalence of alcohol use disorders and anxiety disorders in our comparison group are the lower prevalence of alcohol use disorders in the younger population in China (25, 26) and the limitations of the psychological autopsy method in detecting these disorders (27).
The prevalence of mental illness among our suicide victims was 48.0%, lower than previously reported prevalences of suicides among all age groups in China (10, 11) but similar to the prevalence (44.7%) reported in a recent study of suicide victims in the 15- to 24-year-old age group (28). We compared our results to those of a systematic review of psychiatric diagnoses in suicide victims under 30 years of age (29), a meta-analysis that reviewed 13 reports, most from the West. The prevalence of all psychiatric diagnoses is not comparable with our data because we did not include personality disorders or disruptive behavior disorders, which were highly prevalent in younger suicide victims in the West. Compared to the meta-analysis, our results indicated a moderately lower rate of mood disorders (34.9% compared with 42.1%), a substantially lower rate of substance-related disorders (6.4% compared with 40.8%), and a slightly higher rate of psychotic disorders (11.2% compared with 7.2%). Studies in China have shown that substance-related disorders are less common than in the West (30) and that Chinese young people have a lower risk of alcohol use disorders (25, 26) and are less likely to engage in heavy drinking (31, 32). Thus, this lower prevalence of substance use disorders among suicide victims probably does not reflect different relationships between substance use and suicide in the East and West.
Because the prevalence of mental disorders in both suicide victims and comparison subjects in our study was lower than rates reported for samples from the West, we also compared odds ratios for mental disorders among suicide victims. A systematic review that included 24 psychological autopsy case-control studies reported a crude odds ratio of 5.24 for substance-related disorders and 13.42 for mood disorders (33). These ratios are similar to or lower than those in our study, which suggests that the lower prevalence of mental illness we observed in young Chinese rural suicide victims may be due to the difference in prevalence of mental illness in the general population in China.
The prevalence of mental illness was significantly higher in male than in females suicide victims, and the difference remained significant after controlling for other characteristics. This result is consistent with that of a study on suicide victims 15–24 years of age in China (28). No alcohol- or substance-related disorders were diagnosed in female suicide victims, which is consistent with the previously reported low prevalence of alcohol use disorder (0.2%) among women in China (24). After stratification by gender, the odds ratio for having a mental disorder diagnosis was substantially higher among males than among females. This finding suggests that specific suicide prevention and intervention programs targeting Chinese rural females other than identification and treatment of mental illness are needed.
Consistent with previous reports (10, 11), we found that stressful life events and lower levels of social support were important risk factors. Our findings indicate that besides mental illness as a major risk factor for suicide among young people in rural China, other psychological, social, and cultural factors must play important roles, particularly in women. Future studies should explore the effects of constructs such as social integration (34), cultural values and norms such as face and impulsivity (35), and psychological strain (36, 37) on Chinese suicide.
The lower prevalence of mental illness among Chinese suicide victims provides a unique opportunity to explore possible interactions between mental disorders and other risk factors in suicide. Additive interactions were found between mental illness and lower levels of social support, but not with recent or long-term life events. Mental illness may increase an individual's vulnerability through damage to the ability to maintain existing social relationships, to develop new relationships, or to utilize social support.
One of the limitations of this study was size of the living comparison sample. The total number of living comparison subjects was too small for a detailed examination of the association between suicide and certain categories of mental disorders. For instance, only two comparison subjects were diagnosed as having schizophrenia. This is probably also a major challenge in other psychological autopsy studies of suicide. In a recent similar study in Pakistan, only six of 100 living comparison subjects were diagnosed as having mental illness (38). Our suggestion for future studies would be to enroll multiple living comparison subjects for each suicide victim (e.g., using a 1:2 or 1:3 case-control design) to increase the number of comparison subjects with mental disorders.
Second, there are several methodological concerns in a case-control psychological autopsy study. The use of proxy informants, the retrospective data collection, the lack of blinding regarding case and comparison subjects, and the potential impact of bereavement and stigma against suicide and mental illness on reporting may have an impact on the reliability of the data. Also, our strategy of scheduling interviews with proxy informants for suicide victims 2 to 6 months after suicide clearly differed from our strategy with informants for living comparison subjects and could increase the risk of recall bias.
Third, because different groups of interviewers and psychiatrists had been working on data collection and diagnoses of mental disorder separately at various research sites for more than 2 years, the reliability of diagnoses across investigators, time, and location was a major challenge. However, the diagnoses made in this study are very likely reliable because of the efforts we put into training for all interviewers and psychiatrists, the excellent interrater reliability of diagnoses, and the fact that the prevalence of mental illness among suicide victims and comparison subjects did not differ significantly across research sites and across time.
1 Disease Prevention and Control Bureau of the Ministry of Health, Statistical Information of the Ministry of Health, Chinese Center for Disease Prevention and Control: [Report on Injury Prevention in China]. Beijing, People's Medical Publishing House, 2007 (
2 : Suicide rates in China during a decade of rapid social changes. Soc Psychiatry Psychiatr Epidemiol 2005; 40:792–798 Crossref, Medline, Google Scholar
3 : Suicide rates in China, 1995–99. Lancet 2002; 359:835–840 Crossref, Medline, Google Scholar
4 : Suicide in contemporary China: a review of China's distinctive suicide demographics in their sociocultural context. Harv Rev Psychiatry 2001; 9:1–12 Crossref, Medline, Google Scholar
5 : [The trend and geographic distribution of suicide in the Chinese population]. Zhonghua Liu Xing Bing Xue Za Zhi 2004; 25:280–284 (
6 : Relationships of age and axis I diagnoses in victims of completed suicide: a psychological autopsy study. Am J Psychiatry 1996; 153:1001–1008 Link, Google Scholar
7 American Psychiatric Association: Practice Guideline for the Assessment of Patients With Suicidal Behaviors. Am J Psychiatry 2003; 160(Nov suppl) Google Scholar
8 : Suicide prevention strategies: a systematic review. JAMA 2005; 294:2064–2074 Crossref, Medline, Google Scholar
9 : [Current issues in China's suicide research and prevention]. Chinese Journal of Psychiatry 2003; 36:129–131 (
10 : Risk factors for suicide in China: a national case-control psychological autopsy study. Lancet 2002; 360:1728–1736 Crossref, Medline, Google Scholar
11 : Culture, risk factors, and suicide in rural China: a psychological autopsy case control study. Acta Psychiatr Scand 2004; 110:430–437 Crossref, Medline, Google Scholar
12 : Studying Chinese suicide with proxy-based data: reliability and validity of the methodology and instruments in China. J Nerv Ment Dis 2003; 191:450–457 Crossref, Medline, Google Scholar
13 : Measuring Chinese psychological well-being with Western developed instruments. J Pers Assess 2002; 79:492–511 Crossref, Medline, Google Scholar
14 : Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-I/P). New York, New York State Psychiatric Institute, Biometrics Research, 2002 Google Scholar
15 : Alternative models of the stress buffering hypothesis. Am J Community Psychol 1989; 17:625–642 Crossref, Medline, Google Scholar
16 : The Interview for Recent Life Events. Psychol Med 1997; 27:301–310 Crossref, Medline, Google Scholar
17 : Modern Epidemiology, 3rd ed. Philadelphia, Lippincott Williams & Wilkins, 2008 Google Scholar
18 : Concepts of interaction. Am J Epidemiol 1980; 112:467–470 Crossref, Medline, Google Scholar
19 : Interaction as departure from additivity in case-control studies: a cautionary note. Am J Epidemiol 2003; 158:251–258 Crossref, Medline, Google Scholar
20 : On the estimation of additive interaction by use of the four-by-two table and beyond. Am J Epidemiol 2008; 168:212–224 Crossref, Medline, Google Scholar
21 : Calculating measures of biological interaction. Eur J Epidemiol 2005; 20:575–579 Crossref, Medline, Google Scholar
22 : An Introduction to Epidemiology, 3rd ed. Boston, John & Bartlett Publishers, 2002 Google Scholar
23 : Twelve-month prevalence, severity, and unmet need for treatment of mental disorders in metropolitan China. Psychol Med 2006; 36:257–267 Crossref, Medline, Google Scholar
24 : Drinking and drinking patterns and health status in the general population of five areas of China. Alcohol Alcohol 2004; 39:43–52 Crossref, Medline, Google Scholar
25 : [Alcohol drinking and drinking related problems in six areas in China, part IV: the risk factors of alcohol dependence]. Chinese Journal of Clinical Psychology 1999; 7:4–7 (
26 , et al: [An analysis of alcohol consumption status and alcohol related-factors in the Pearl River Delta area in China]. Chinese Journal of Behavioral Medical Science 2005; 14:730–732 (
27 : The validity of proxy-based data in suicide research: a study of patients 50 years of age and older who attempted suicide, II: life events, social support, and suicidal behavior. Acta Psychiatr Scand 2001; 104:452–457 Crossref, Medline, Google Scholar
28 : Risk factors for suicide in China's youth: a case-control study. Psychol Med 2008; 38:397–406 Crossref, Medline, Google Scholar
29 : Completed suicide and psychiatric diagnoses in young people: a critical examination of the evidence. Am J Orthopsychiatry 2005; 75:676–683 Crossref, Medline, Google Scholar
30 : Drug addiction in China. Ann NY Acad Sci 2008; 1141:304–317 Crossref, Medline, Google Scholar
31 : Increased drinking in a metropolitan city in China: a study of alcohol consumption patterns and changes. Addiction 2008; 103:416–423 Crossref, Medline, Google Scholar
32 : A comparative survey on alcohol and tobacco use in urban and rural populations in the Huaihua District of Hunan Province, China. Alcohol 2006; 39:87–96 Crossref, Medline, Google Scholar
33 : Suicidal risk factors and completed suicide: meta-analyses based on psychological autopsy studies. Environ Health Prev Med 2008; 13:243–256 Crossref, Medline, Google Scholar
34 : Suicide: A Study in Sociology. New York, Free Press, 1951 (original work published in 1897) Google Scholar
35 : Low-planned suicides in China. Psychol Med 2005; 35:1197–1204 Crossref, Medline, Google Scholar
36 : Psychological strains found from in-depth interviews with 105 Chinese rural youth suicides. Arch Suicide Res 2009; 13:185–194 Crossref, Medline, Google Scholar
37 : Characteristics of young rural Chinese suicides: a psychological autopsy study. Psychol Med 2010; 40:581–589 Crossref, Medline, Google Scholar
38 : Case-control study of suicide in Karachi, Pakistan. Br J Psychiatry 2008; 193:403–405 Crossref, Google Scholar

