
Cigarette Smoking and Panic: The Role of Neuroticism
Abstract
OBJECTIVE: The authors sought to determine the relationship of panic attacks, cigarette smoking, and neuroticism. METHOD: Data were drawn from the Midlife Development in the United States Survey, a representative household survey of the adult population of the United States (N=3,032). Multivariate logistic regression analyses were used to determine the association between panic attacks and cigarette smoking and to determine whether neuroticism was an independent predictor of the co-occurrence of cigarette smoking and panic attacks. RESULTS: The majority of individuals with panic attacks had been regular smokers during their lifetime (81.1%), a significantly higher rate than seen among subjects without panic attacks (69.4%). Regular cigarette smoking was associated with a significantly greater risk of current panic attacks. This significant association persisted after analyses controlled for demographic characteristics, depression, and alcohol/substance use disorders but was no longer evident after analyses adjusted for neuroticism. Neuroticism independently predicted the co-occurrence of regular cigarette smoking and panic attacks but did not predict either panic attacks or cigarette smoking in the absence of the other. CONCLUSIONS: Consistent with previous findings, these data suggest that panic attacks are associated with greater risk of cigarette smoking but provide new evidence that neuroticism may play an essential role in this relationship. These data are preliminary but, if replicated, suggest that neuroticism may reflect a shared vulnerability for the co-occurrence of cigarette smoking and panic attacks. Future studies are needed to further explore the mechanism of this association.
Previous data have suggested that panic attacks and cigarette smoking co-occur more frequently than would be expected by chance. While the mechanism of this association remains unknown (1–5), several hypotheses have been offered. It is possible that cigarette smoking, which some believe has anxiolytic properties, is an attempt to self-medicate anxiety (6, 7). It is also conceivable that the use of cigarettes leads to the onset of anxiety (e.g., panic attacks) through respiratory changes or nicotine-induced effects (1, 8–10). Alternatively, it has been hypothesized that this co-occurrence reflects an underlying shared etiologic vulnerability for both cigarette smoking and panic.
Previous epidemiologic studies have found a higher risk of panic disorder in early adulthood among those who smoke cigarettes during adolescence (1–3), offering support for the hypothesis that cigarette smoking may increase the risk of the development of panic and other anxiety disorders (2, 3). In contrast, other population-based studies have shown that anxiety and depression increase the risk of cigarette smoking among adolescents, potentially reflecting self-medication (5). Previous studies, however, have focused relatively little direct attention on the alternative hypothesis that there is a third factor, a possible shared (genetic or environmental) vulnerability for both panic and cigarette smoking that underlies their association. Personality traits are one factor that might contribute to the risk of both panic attacks and cigarette smoking (11, 12). For instance, neuroticism, and its relationship to cigarette smoking, has been examined in several clinical, epidemiologic, and genetic studies (13–18). Epidemiologic study data on adults (17) and adolescents (18) support a connection between smoking and neuroticism, as have data from clinical samples (14) and twin studies (19). Other unrelated studies have found that both panic disorder and infrequent panic attacks are associated with neuroticism as well (20, 21).
To date, no previous study to our knowledge has investigated the relationship between panic attacks, cigarette smoking, and neuroticism. Given that previous studies have suggested a two-way link between each of these three potential factors, the current study was undertaken to investigate whether neuroticism is associated with a higher risk of the co-occurrence of panic attacks and cigarette smoking. The three main objectives of this investigation were to determine 1) the relationship between cigarette smoking and panic attacks among adults in the population, 2) whether neuroticism acts as an effect modifier in the relationship between panic attacks and cigarette smoking, and 3) whether neuroticism is an independent predictor of the co-occurrence of cigarette smoking and panic attacks. We hypothesized that cigarette smoking would be associated with a higher risk of panic attacks in the presence, but not in the absence, of a high level of neuroticism. We also predicted that neuroticism would be an independent predictor of the co-occurrence of cigarette smoking and panic attacks among adults in the general population.
Method
Sample
The Midlife Development in the United States Survey is a nationally representative survey of 3,032 persons aged 25–74 years in the noninstitutionalized civilian population of the 48 coterminous United States (22, 23). The survey was carried out by the John D. and Catherine T. MacArthur Foundation Research Network on Successful Midlife Development between January 1995 and January 1996. All respondents completed a 30-minute telephone interview (70.0% response rate) and filled out two mailed questionnaires estimated to take a total of about 90 minutes to complete. Among the subgroup of telephone respondents, there was an 86.8% response rate for an overall response rate of 60.8%. The data reported here were weighted to adjust for differential probabilities of selection and nonresponse. More details on the survey design, field procedures, and sampling weights are available elsewhere (22, 23).
Assessment
Diagnoses
Psychopathology among the survey respondents was assessed by using the Composite International Diagnostic Interview Short Form scales, a series of diagnostic-specific scales that were developed from item-level analyses of the Composite International Diagnostic Interview questions in the National Comorbidity Survey (24). The short form was designed to reproduce the full Composite International Diagnostic Interview as well as possible with only a small subset of the original questions. Diagnoses (occurring in the preceding 12 months) assessed in the Midlife Development in the United States Survey included major depression, panic attacks, generalized anxiety disorder, alcohol abuse and dependence, and drug abuse and dependence. High sensitivity and specificity have been reported for Composite International Diagnostic Interview Short Form diagnostic classifications (panic attacks: 90.0 and 99.5, respectively; major depression: 89.6 and 93.9; generalized anxiety disorder: 96.6 and 99.8; alcohol dependence: 93.6 and 96.2; substance dependence: 77.0 and 99.9) (25).
Personality factors
Personality traits were assessed by using the Midlife Development Inventory (unpublished 1997 instrument of M.E. Lachman and S.L. Weaver), which was developed from the results of a pilot study that had a probability sample of 1,000 men and women aged 30–70 (574 valid cases were usable for item analysis) (26–30). Items with the highest item-to-total correlations and factor loadings were selected for the instrument. Forward regressions were also run to determine the smallest number of items needed to account for over 90% of the total scale variance. The Midlife Development Inventory assesses five personality traits: agreeableness (scale items: helpful, warm, caring, softhearted, and sympathetic; alpha=0.80); openness to experience (scale items: creative, imaginative, intelligent, curious, sophisticated, and adventurous; alpha=0.77); conscientiousness (scale items: organized, responsible, hardworking, and [not] careless; alpha=0.57); extroversion (scale items: outgoing, friendly, lively, active, and talkative; alpha=0.78); and neuroticism (scale items: moody, worrying, nervous, and [not] calm; alpha=0.74). The alphas are based on the Midlife Development in the United States Survey national sample.
Cigarette smoking
All subjects were asked about current and past smoking habits. A history of regular cigarette smoking was defined by an affirmative response to the question, “Have you ever smoked cigarettes regularly—that is, at least a few cigarettes every day?”
Analyses
First, Pearson’s chi-square tests were used to determine differences in demographic characteristics and rates of comorbid major depression, generalized anxiety disorder, and alcohol/substance use disorders among four mutually exclusive groups: 1) individuals who had never been regular smokers and had not experienced a panic attack (past 12 months), 2) those who reported having panic attacks but had never been regular smokers, 3) those who had been regular smokers but had never had a panic attack, and 4) those who had been regular smokers and reported having panic attacks. All tests were two-sided, and significance was set at 0.01. Next, multivariate logistic regression analyses were used to calculate odds ratios (with 95% confidence intervals [CIs]) of the association between panic and cigarette smoking after we adjusted for demographic characteristics, comorbid disorders, and neuroticism. Third, the relationship between neuroticism as an independent predictor of co-occurring cigarette smoking and panic attacks, compared with the risk of either without the other, after we controlled for demographic characteristics and comorbid mental disorders, was determined by using multivariate logistic regression analyses. Odds ratios (with 95% CIs) were calculated to assess the measure of association between neuroticism and each of these three conditions. Multivariate logistic regression analyses were then used to produce crude and adjusted odds ratios (with 95% CIs) describing the relationship between panic attacks and regular cigarette smoking after we controlled for sociodemographic characteristics, psychiatric comorbidity, and neuroticism. Interaction terms were included in separate models and the Breslow-Day test for homogeneity was used to examine evidence for interaction on the multiplicative scale. In order to evaluate whether the relationship between neuroticism, panic, and cigarette smoking is unique or a general personality effect, the other four of the “big five” personality factors were also tested. Additional analyses were run in order to determine whether these results were consistent with the use of current, rather than lifetime, cigarette smoking. Analyses were performed by using the statistical software package SPSS for Windows (31). Only p<0.01 results are reported as significant in order to account for the large number of statistical comparisons.
Results
In terms of age, the subjects with no history of panic attacks or smoking (mean=44.5 years, SD=13.1), those who never smoked but experienced panic attacks (mean=48.8 years, SD=13.1), those who smoked but never experienced panic attacks (mean=47.7 years, SD=13.0), and those who smoked and experienced panic attacks (mean=42.7 years, SD=10.3) were significantly different (F=13.5, df=3, 2271, p<0.0001). Of the individuals with a history of panic attacks (N=146), the majority (81.1%) had been regular smokers at some point during their lifetime, which was significantly different from the smoking rate of those who never experienced panic attacks (69.4%) (χ2=9.0, df=1, p=0.002). Individuals with panic attacks who were smokers were more likely to be female and were less likely to be married compared with those without panic attacks (Table 1). Individuals who were smokers and had panic attacks also had significantly higher odds of having comorbid major depression than did those who smoked but never had a panic attack (F=72.1, df=1, 1594, p<0.01). Of interest, all individuals with co-occurring panic attacks and alcohol/substance use disorders had been cigarette smokers.
Relationship Between Panic Attacks and Cigarette Smoking
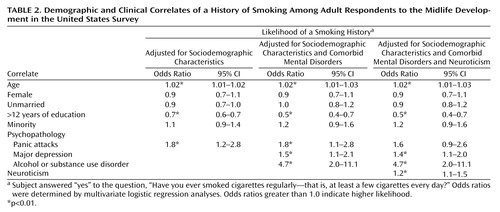
Panic attacks were associated with a significantly higher likelihood of cigarette smoking (odds ratio=1.9, 95% CI=1.3–2.9). The association between panic attacks and higher odds of cigarette smoking persisted even after analyses controlled for sociodemographic characteristics (Table 2). The relationship remained significant after analyses controlled for comorbid mental disorders but was no longer evident after adjusting for neuroticism.
Neuroticism as a Predictor of Cigarette Smoking and Panic Attacks
Results of three separate multivariate logistic regression analyses, with neuroticism as the independent variable and the three indicator variables (panic without smoking, smoking without panic, co-occurring panic and smoking) as dependent variables revealed that neuroticism was not significantly associated either with panic attacks without smoking or with cigarette smoking in the absence of panic attacks. Neuroticism was an independent predictor of the co-occurrence of cigarette smoking and panic, even after we controlled for differences in sociodemographic characteristics and psychiatric comorbidity (Table 3). In other words, with every 1-point increase in neuroticism, the odds of co-occurring panic and cigarette smoking increased four-fold. None of the other personality traits showed similar effects. When these analyses were rerun using current rather than lifetime smoking, results of each analysis were consistent with those presented. Also, there was no statistically significant difference in neuroticism between those who were current and lifetime smokers.
Interaction Between Cigarette Smoking and Panic Attacks
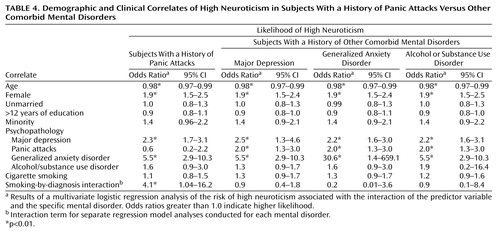
Four additional multivariate logistic regression analyses were used to investigate the possible interaction between panic attacks, neuroticism, and cigarette smoking. Separate multivariate logistic regression analyses were run, each with an interaction term testing for interaction between regular cigarette smoking and each mental disorder. High neuroticism was the dependent variable in these models. Results showed evidence of interaction on the multiplicative scale for the relationship between cigarette smoking and panic in the odds of high neuroticism (Table 4). In contrast, there was no interaction between major depression, generalized anxiety disorder, or alcohol or substance use and cigarette smoking in the odds of high neuroticism.
Discussion
Consistent with previous findings, these data suggest that panic attacks are associated with a higher odds of cigarette smoking. They also introduce new evidence documenting this association in the absence of depression and alcohol/substance use disorders. Our results also revealed that the relationship between panic attacks and cigarette smoking was no longer evident after we controlled for neuroticism, indicating that there may be a synergistic relationship between high neuroticism and the likelihood of the co-occurrence of panic attacks and cigarette smoking. These results provide preliminary evidence suggesting that neuroticism may reflect an underlying shared vulnerability to the co-occurrence of cigarette smoking and panic attacks.
The mechanism for the observed association of neuroticism, panic, and cigarette smoking is not known. It might be that panic and smoking lead to a higher risk of the development of neuroticism, although most studies of personality would not support this hypothesis. Alternatively, it is possible that panic leads to a higher risk of cigarette smoking, or cigarette smoking to a higher risk of panic attacks, but only in the presence of a high level of neuroticism. It may also be that neuroticism reflects a separate trait (genetic or otherwise) that independently predicts the co-occurrence of panic and cigarette smoking through an unknown mechanism. While it is not possible to determine causality from these analyses, neuroticism is generally considered a lifelong, underlying trait and, as previous studies have suggested, may even have genetically determined influences. The results of our analyses, therefore, tend to support the hypotheses of self-medication or shared vulnerability rather than causality (i.e., that cigarette smoking and panic increase the risk of neuroticism).
One considerable limitation of our investigation is the use of cross-sectional data, which does not allow us to test for interaction on the additive scale because of lack of inability to calculate risk ratios. These data are also limited by the lack of information on age at onset of panic attacks, which would be of interest in examining the temporal relationship between onset of panic and initiation of cigarette smoking. The “onset,” per se, of neuroticism is a variable unlikely to be considered objectively quantifiable, since the initiation of personality development onset may not be observable in the outbreak of symptoms, which is the usual manner that the onset of mental disorders is evaluated currently. The relationship between panic and cigarette smoking, which showed evidence of interaction on the multiplicative scale, reveals the possibility that a future study that is able to test for interaction on an additive scale could provide evidence of biologic synergism between these variables. The use of a large, nationally representative sample of adults, who were assessed with reliable instruments on a variety of characteristics, is a strength of this study. The lack of available information on other mental disorders that have been associated with cigarette smoking (e.g., schizophrenia [32]) is another shortcoming of this study. Also, lack of data on lifetime panic attacks is a limitation of our analyses, since this necessitated the comparison of cigarette smoking (lifetime) and neuroticism (usually conceived of as lifetime [33]) with current panic attacks (past 12 months), which may influence results. The consistency of our findings with the use of either lifetime or current smoking provides further support for these conclusions. However, it should be noted that this difference in time period could have an influence on our results.
Future studies that investigate this relationship in a prospective, longitudinal epidemiologic sample, throughout the lifespan, may be able to more directly address and provide answers to the remaining questions about the mechanism of association. Family and genetic studies looking at the association between neuroticism, panic, and cigarette smoking may also be useful in providing clues to a possible underlying inherited contribution to both smoking and panic. In light of previous data showing evidence of synergistic relationships between personality, smoking, and risk of various types of cancer and associated mortality (34, 35), future studies that compare physical morbidity and mortality estimates and rates of cigarette smoking, panic, and neuroticism may also be of interest, especially in view of the higher-than-expected prevalence of cardiovascular disease-related mortality among panic disorder patients (36), which may be associated with effects of cigarette smoking. Further work is needed to determine the mechanism of these associations.
 |
 |
 |
 |
Received May 8, 2001; revision received Sept. 24, 2001; accepted March 5, 2002. From the Department of Psychiatry, New York State Psychiatric Institute; and the Joseph L. Mailman School of Public Health, Columbia University, New York. Address reprint requests to Dr. Goodwin, Department of Psychiatry, New York State Psychiatric Institute, 1051 Riverside Dr., Unit 43, New York, NY 10032; [email protected] (e-mail). The authors thank Peter M. Lewinsohn, Ph.D., for his comments on an earlier version of this manuscript.
1. Breslau N, Klein DF: Smoking and panic attacks: an epidemiologic investigation. Arch Gen Psychiatry 1999; 56:1141-1147Crossref, Medline, Google Scholar
2. Johnson JG, Cohen P, Pine DS, Klein DF, Kasen S, Brook JS: Association between cigarette smoking and anxiety disorders during adolescence and early adulthood. JAMA 2000; 284:2348-2351Crossref, Medline, Google Scholar
3. Kandel DB, Johnson JG, Bird HR, Canino G, Goodman SH, Lahey BB, Regier DA, Schwab-Stone M: Psychiatric disorders associated with substance use among children and adolescents: findings from the Methods for the Epidemiology of Child and Adolescent Mental Disorders (MECA) Study. J Abnorm Child Psychol 1997; 25:121-132Crossref, Medline, Google Scholar
4. Amering M, Bankier B, Berger P, Griengl H, Windhaber J, Katsching H: Panic disorder and cigarette smoking behavior. Compr Psychiatry 1998; 40:35-38Crossref, Google Scholar
5. Patton GC, Hibbert M, Rosier MJ, Carlin JB, Caust J, Bowes G: Is smoking associated with anxiety and depression in teenagers? Am J Public Health 1996; 86:225-230Crossref, Medline, Google Scholar
6. Breslau N, Kilbey MM, Andreske P: DSM-III-R nicotine dependence in young adults: prevalence, correlates, and associated psychiatric disorders. Addiction 1990; 89:743-754Crossref, Google Scholar
7. Kessel JD, Shiffman S: Attentional mediation of cigarette smoking’s effect on anxiety. Health Psychol 1997; 16:359-368Crossref, Medline, Google Scholar
8. Pohl P, Yeragani VK, Balon R, Lycaki H, McBride R: Smoking in patients with panic disorder. Psychiatry Res 1992; 43:253-262Crossref, Medline, Google Scholar
9. Dilsaver SC: Nicotine and panic attacks. Am J Psychiatry 1987; 144:1245-1246Medline, Google Scholar
10. West R, Hajek P: What happens to anxiety levels on giving up smoking? Am J Psychiatry 1997; 154:1589-1592Link, Google Scholar
11. McCrae RR, Costa PT: Validation of the five-factor model of personality across instruments and observers. J Pers Soc Psychol 1997; 52:81-90Crossref, Google Scholar
12. Costa PT, McCrae RR: Personality in adulthood: a six-year longitudinal study of self-reports and spouse ratings on the NEO Personality Inventory. J Pers Soc Psychol 1998; 54:853-863Crossref, Google Scholar
13. Patton D, Barnes GE, Murray RP: A personality typology of smokers. Addict Behav 1997; 22:269-273Crossref, Medline, Google Scholar
14. Herran A, de Santiago A, Sandoya M, Fernandez MJ, Diez-Manrique JF, Vasquez-Barquero JL: Determinants of smoking behavior in outpatients with schizophrenia. Schizophr Res 2000; 21:373-381Crossref, Google Scholar
15. Kawakami N, Takai A, Takatsuka N, Shimizu H: Eysenck’s personality and tobacco/nicotine dependence in male ever-smokers in Japan. Addict Behav 2000; 25:585-591Crossref, Medline, Google Scholar
16. Hu S, Brody CL, Fisher C, Gunzerath L, Nelson ML, Greenberg BD, Murphy DL, Hames DH: Interaction between the serotonin transporter gene and neuroticism in cigarette smoking behavior. Mol Psychiatry 2000; 5:181-188Crossref, Medline, Google Scholar
17. Yoshimura K: The psychological characteristics of tobacco dependence in a rural area of Japan. J Epidemiol 2000; 10:271-279Crossref, Medline, Google Scholar
18. Byrne DG, Byrne AE, Reinhart MI: Personality, stress, and the decision to commence cigarette smoking in adolescence. J Psychosom Res 1995; 39:53-62Crossref, Medline, Google Scholar
19. Kendler KS, Neale MC, Sullivan P, Corey LA, Gardner CO, Prescott CA: A population-based twin study in women of smoking initiation and nicotine dependence. Psychol Med 1999; 29:299-308Crossref, Medline, Google Scholar
20. Katon W, Hollifield M, Chapman T, Mannuzza S, Ballenger J, Fyer AJ: Infrequent panic attacks: psychiatric comorbidity, personality characteristics, and functional disability. J Psychiatr Res 1997; 29:121-131Crossref, Google Scholar
21. Hollifield M, Katon W, Skipper B, Chapman T, Ballenger JC, Mannuzza S, Fyer AJ: Panic disorder and quality of life: variables predictive of functional impairment. Am J Psychiatry 1997; 154:766-772Link, Google Scholar
22. Kessler RC, Mickelson KD, Zhao S: Patterns and correlates of self-help group membership in the United States. Soc Policy 1997; 27:27-46Google Scholar
23. Kessler RC, DuPont RL, Berglund P, Wittchen HU: Impairment in pure and comorbid generalized anxiety disorder and major depression at 12 months in two national surveys. Am J Psychiatry 1999; 156:1915-1923Link, Google Scholar
24. Kessler RC, Andrews G, Mroczek D, Ustun B, Wittchen H-U: The World Health Organization Composite International Diagnostic Interview Short Form (CIDI-SF). Int J Methods in Psychiatr Res 1998; 7:171-185Crossref, Google Scholar
25. Wittchen H-U: Reliability and validity studies of the WHO Composite International Diagnostic Interview(CIDI): a critical review. J Psychiatr Res 1994; 28:57-84Crossref, Medline, Google Scholar
26. Bem SL: Bem Sex-Role Inventory Manual. Palo Alto, Calif, Consulting Psychologists Press, 1981Google Scholar
27. Trapnell PD, Wiggins JS: Extension of the Interpersonal Adjective Scales to include the big five dimensions of personality. J Pers Soc Psychol 1990; 59:781-790Crossref, Google Scholar
28. John OP: The “big five” factor taxonomy: dimensions of personality in the natural language and in questionnaires, in Handbook of Personality Theory and Research. Edited by Pervin LA. New York, Guilford, 1990, pp 66-100Google Scholar
29. Goldberg LR: The development of markers for the big-five factor structure. Psychol Assess 1992; 4:26-42Crossref, Google Scholar
30. Digman JM: Personality structure: emergence of the five-factor model. Annu Rev Psychol 1990; 41:417-440Crossref, Google Scholar
31. SPSS 9.0 for Windows. Chicago, SPSS, 1998Google Scholar
32. Kelly C, McCreadie RG: Smoking habits, current symptoms, and premorbid characteristics of schizophrenic patients in Nithsdale, Scotland. Am J Psychiatry 1999; 156:1751-1757Link, Google Scholar
33. Costa PT Jr, Herbst JH, McCrae RR, Siegler IC: Personality at midlife: stability, intrinsic maturation, and response to life events. Assessment 2000; 7:365-378Crossref, Medline, Google Scholar
34. Eysenck HJ, Grossarth-Maticek R, Everitt B: Personality, stress, smoking, and predisposition as synergistic risk factors for cancer and coronary heart disease. Integr Physiol Behav Sci 1991; 20:309-322Crossref, Google Scholar
35. Grossarth-Maticek R, Eysenck HJ: Personality, smoking, and alcohol as synergistic risk factors for cancer of the mouth and pharynx. Psychol Rev 1990; 67:1024-1026Google Scholar
36. Coryell W, Noyes R, Clancy J: Excess mortality in panic disorder: a comparison with unipolar depression. Arch Gen Psychiatry 1982; 39:701-703Crossref, Medline, Google Scholar

