
Gender Differences in Panic Disorder: Findings From the National Comorbidity Survey
Abstract
OBJECTIVE: Several epidemiological studies have demonstrated a higher prevalence of panic disorder in women than in men. This study explored whether the prevalence of specific panic symptoms differs by gender. METHOD: National Comorbidity Survey data from 609 respondents who met DSM-III-R criteria for panic disorder or panic attacks were analyzed to test for gender differences across 18 panic symptoms. RESULTS: Among National Comorbidity Survey respondents with panic disorder or panic attacks, female respondents were more likely than male respondents to experience respiration-related difficulties during panic attacks. CONCLUSIONS: Specific symptoms occurring during panic attacks differ by gender. The pathophysiology of these symptom differences may involve gender differences in sensitivity to CO2 and in the threshold for panic attacks during hypoxic and hypercapnic states.
Panic disorder is an anxiety disorder consisting of recurrent, unexpected panic attacks usually accompanied by a variety of somatic and cognitive symptoms. According to DSM-IV, panic attacks are characterized by discrete periods of fear or discomfort accompanied by at least four somatic or cognitive symptoms (e.g., shortness of breath, increased heart rate, trembling, sweating, fear of dying) that reach a crescendo within 10 minutes. Typically, panic attacks may be accompanied by an urge to flee, as well as apprehensions that escape or help will not be possible.
The National Comorbidity Survey (1) examined the presence of psychiatric morbidity, including panic disorder, in a large national sample. Findings from the National Comorbidity Survey suggested that panic disorder occurs more frequently in women than in men. In a study based on data from the survey, Eaton et al. (2) found that a DSM-III-R diagnosis of lifetime panic disorder was about 2.5 times more common in female than in male respondents. Among female respondents age 15–24 years, the rate of panic disorder was 2.5% (SE=0.7%), compared with 1.3% (SE=0.6%) for male respondents age 15–24 years. The gender difference increased by age, so that among 35–44-year-old female respondents the rate was 2.1% (SE=0.8%), compared to 0.6% (SE=0.2%) for same-age male respondents. Other epidemiological studies have also found gender differences for panic disorder. Joyce et al. (3) found that panic disorder was almost four times as frequent in female than in male subjects. In a sample of 1,498 urban adults, 3.4% (SE=0.7%) of female subjects received a diagnosis of panic disorder, compared with 0.9% (SE=0.6%) of male subjects. These population estimates consistently indicate that panic disorder seems to occur more frequently in women than in men. In addition, women may be more likely than men to have more severe and chronic forms of panic disorder with agoraphobia (4). Also, in a study of patients who had panic disorder with agoraphobia, women reported having more agoraphobic avoidance symptoms, especially when they were alone, than did men (5).
The study reported here initiated an exploratory investigation of gender differences in specific symptoms of panic attacks and panic disorder, as reflected in the empirical data from the National Comorbidity Survey. We sought to determine if gender differences occurred, and, if so, whether they could be understood in light of our current knowledge of physiological differences between genders.
Method
Sample
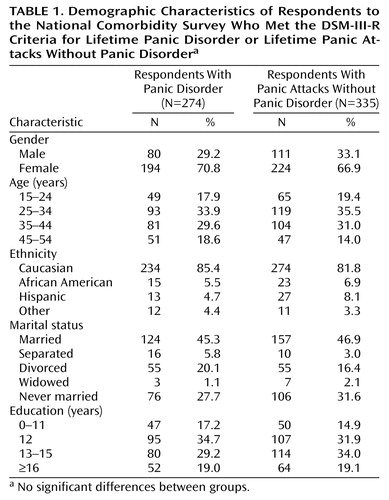
The National Comorbidity Survey was a nationally representative, epidemiological study that included stratified, multiple-stage probability samples of individuals between ages 15 and 54 years throughout the mainland United States. Data were collected between September 1990 and February 1992. More information about the sampling methods and the characteristics of the overall sample is available from other sources (1). Of the 8,098 original respondents in the National Comorbidity Survey, 274 individuals (3.4% of the total sample) met diagnostic criteria for lifetime panic disorder and 335 individuals (4.1% of the total sample) had lifetime panic attacks without panic disorder. Of the respondents in the panic disorder sample, 194 (70.8%) were female and 80 (29.2%) were male. In the sample with panic attacks only, 224 respondents (66.9%) were female and 111 (33.1%) were male. The mean ages were 34.8 years (SD=10.2, range=15–54) for the respondents with panic disorder and 33.8 years (SD=9.5, range=15–54) for the respondents with panic attacks only. The average age at onset of panic attacks was 20.7 years (SD=9.7) for male respondents and 22.0 years (SD=10.2) for female respondents. The average age at onset of panic disorder was 23.7 years (SD=9.5) for male respondents and 25.0 years (SD=10.0) for female respondents. Table 1 presents additional demographic characteristics of the sample. In both diagnostic groups, there were no significant differences between male and female respondents in age, education, marital status, or ethnicity.
Assessment of Mental Disorders
Panic attacks were defined in the National Comorbidity Survey as the patient’s “worst spells or attacks of suddenly feeling very frightened or very uneasy” accompanied by at least four cognitive or somatic symptoms. This definition reflects both ICD-10 and DSM-III-R criteria. To meet the diagnostic criteria, the panic attack must reach a crescendo, that is, have a rapid escalation and plateau, within a few minutes of its onset. The criteria for a diagnosis of panic disorder were the presence of four or more panic attacks in a 1-month period and an accompanying feeling of being “constantly frightened” about future attacks. Additional information about the assessment of psychiatric conditions in the National Comorbidity Survey is available from other sources (1, 2). Since minimal changes occurred between the DSM-III-R and DSM-IV criteria sets of panic symptoms, findings from the National Comorbidity Survey regarding the clinical features of this disorder reflect the current diagnostic standard.
Statistical Analyses
We examined gender differences in the frequency of all panic-related symptoms. First, panic disorder and panic attack data were analyzed separately. For each diagnostic group, descriptive and frequency analyses (gender by individual symptoms) were computed across all 18 panic symptoms. We completed a series of two-by-two cross-tabulations with analysis of proportions to compute chi-square statistics with Yates’s correction. Next, a binary logistic regression analysis with a forward-entry, likelihood-ratio statistic was conducted with the 18 panic symptoms as the indicator variables and gender as the dependent variable. Associated statistics, including chi-square and Wald statistics, partial correlations, odds ratio, and confidence intervals, are presented for the final model. The significance level chosen for a two-tailed test was p<0.05.
Results
Table 2 presents the results of the frequency analyses of panic symptoms for male and female respondents who met criteria for panic disorder or panic attacks. For both diagnostic categories and for both sexes, heart pounding was the most frequently experienced panic symptom. Between 94% and 97% of all respondents with panic disorder or panic attacks reported increased heart pounding during a panic attack. In the panic disorder group, female respondents experienced some symptoms more frequently than male respondents. For instance, a significantly greater proportion of female than male respondents complained of shortness of breath (72% versus 50%; χ2=10.8, df=1, p=0.001), feeling faint (59% versus 45%; χ2=3.7, df=1, p=0.05), and feeling smothered (60% versus 43%; χ2=5.9, df=1, p=0.02). Similarly, in the panic attack group, female respondents were more likely than male respondents to complain of shortness of breath (65% versus 50%; χ2=6.9, df=1, p=0.009), choking or difficulty swallowing (37% versus 25%; χ2=3.8, df=1, p=0.05), and feeling smothered (50% versus 38%; χ2=4.5, df=1, p=0.03). In the panic attack group female respondents were more likely than male respondents to report nausea, but the difference was not significant (40% versus 29%; χ2=3.6, df=1, p=0.06). Male respondents in both diagnostic groups endorsed pain in the stomach more often than female respondents, but the differences did not reach the level of significance (panic disorder group: 60% versus 48%; χ2=2.9, df=1, p=0.09) (panic attack group: 41% versus 40%; χ2<0.1, df=1, p=1.00).
Table 3 and Table 4 present the results of the logistic regression models specified for the panic disorder group and the panic attack group (i.e., those with history of panic of panic attacks who did not fulfill the criteria for panic disorder), respectively. These analyses confirmed that similar indicators were significant for predicting gender, including shortness of breath and nausea. Finally, scores from both groups were pooled. Five somatic symptoms entered the logistic model (Table 5). Three symptoms predicted female gender: shortness of breath (odds ratio=1.9, 95% CI=1.3–2.8), nausea (odds ratio=1.8, 95% CI=1.2–2.8), and feeling smothered (odds ratio=1.5, 95% CI=1.0–2.2). Two symptoms predicted male gender: sweating (odds ratio=0.6, 95% CI=0.4–0.9) and pain in the stomach (odds ratio=0.6, 95% CI=0.4–0.9).
Discussion
Overall, the results of this study indicate that gender differences in specific symptoms exist both for subjects who meet the criteria for panic attacks and for those who meet the criteria for panic disorder. Specifically, a significantly greater proportion of female subjects experienced respiration-related symptoms (difficulty breathing, feeling faint, and feeling smothered) during panic attacks. Certain pathophysiological mechanisms may be relevant in elucidating these gender differences in respiratory symptoms during panic attacks.
To demonstrate how respiration potentially mediates bodily symptoms in panic, several experimental studies have used CO2 inhalation and lactate infusion to induce hypocapnic states in panic-prone individuals. These two challenge techniques are perhaps the most reliable experimental panic-onset stimulants; furthermore, the potential physiological significance of the two techniques, which produce a shortage of oxygen, may be similar. Of particular relevance to our findings is the study by Papp et al. (6), who found that the physiological response to CO2 in female panic disorder patients differed significantly across multiple indicators, including at-rest breathing rate and end-tidal CO2. In addition, in the same study, female panic disorder patients, compared to male patients, showed greater CO2 sensitivity, as illustrated by their higher respiratory rate. These findings suggest that female panic disorder patients may have a low threshold for panic attacks during hypoxic and hypercapnic states and are consistent with suggestions that a hypersensitive suffocation false alarm may be particularly implicated in panic disorder in female patients (7).
Our findings are limited by the retrospective nature of assessments in this epidemiological study. Additional studies are necessary to test the finding that female subjects experience more breathing problems during panic attacks, compared with male subjects. In addition, a potentially interesting group is female patients with premenstrual dysphoric disorder. To our knowledge, these patients constitute the only diagnostic group to show parallel panic and respiration responses to challenges with CO2 and lactate (8, 9). Prospective studies with panic disorder and premenstrual dysphoric disorder patients may shed further light on gender-based differences in panic symptoms.
 |
 |
 |
 |
 |
Received Nov. 9, 2000; revision received May 1, 2001; accepted June 1, 2001. From Stanford University and the VA Palo Alto Health Care System; and Columbia University and New York State Psychiatric Institute, New York. Address reprint requests to Dr. Sheikh, VA Palo Alto Health Care System (116A-MP), 795 Willow Rd., Menlo Park, CA 94025; [email protected] (e-mail). The National Comorbidity Survey was supported by NIMH grants MH-46376 and MH-49098, a supplement to grant MH-46376 from the National Institute on Drug Abuse, and grant 90135190 from the W.T. Grant Foundation.
1. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen H-U, Kendler KS: Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8-19Crossref, Medline, Google Scholar
2. Eaton WW, Kessler RC, Wittchen HU, Magee WJ: Panic and panic disorder in the United States. Am J Psychiatry 1994; 151:413-420Link, Google Scholar
3. Joyce PR, Bushnell JA, Oakley-Browne MA, Wells JE, Hornblow AR: The epidemiology of panic symptomatology and agoraphobic avoidance. Compr Psychiatry 1989; 30:303-312Crossref, Medline, Google Scholar
4. Yonkers KA, Zlotnick C, Allsworth J, Warshaw M, Shea T, Keller MB: Is the course of panic disorder the same in women and men? Am J Psychiatry 1998; 155:596-602Link, Google Scholar
5. Turgeon L, Marchand A, Dupuis G: Clinical features in panic disorder with agoraphobia: a comparison of men and women. J Anxiety Disord 1998; 12:539-553Crossref, Medline, Google Scholar
6. Papp LA, Martinez JM, Klein DF, Coplan JD, Norman RG, Cole R, de Jesus MJ, Ross D, Goetz R, Gorman JM: Respiratory psychophysiology of panic disorder: three respiratory challenges in 98 subjects. Am J Psychiatry 1997; 154:1557-1565Abstract, Google Scholar
7. Klein DF: False suffocation alarms, spontaneous panics, and related conditions: an integrative hypothesis. Arch Gen Psychiatry 1993; 50:306-317Crossref, Medline, Google Scholar
8. Harrison WM, Sandberg D, Gorman JM, Fyer M, Nee J, Uy J, Endicott J: Provocation of panic with carbon dioxide inhalation in patients with premenstrual dysphoria. Psychiatry Res 1989; 27:183-192Crossref, Medline, Google Scholar
9. Sandberg D, Endicott J, Harrison W, Nee J, Gorman J: Sodium lactate infusion in late luteal phase dysphoric disorder. Psychiatry Res 1993; 46:79-88Crossref, Medline, Google Scholar

