
Victims of Criminal Homicide in Sweden: A Matched Case-Control Study of Health and Social Risk Factors Among All 1,739 Cases During 1978–1994
Abstract
OBJECTIVE: The psychiatric and medical characteristics of victims of homicide have not been systematically studied and are often confounded by race. This study was undertaken to determine health and social factors contributing to the risk of being murdered in the Swedish, predominantly Caucasian population. METHOD: All 1,739 homicides between 1978 and 1994 in Sweden were studied in terms of variables in national case registers regarding health, crimes, immigration, and marital status. The same data were extracted for matched comparison persons in the general population, with controls for time of exposure. The data were analyzed by conditional logistic regression on matched pairs. RESULTS: Traumatic brain injury, physical abuse, alcohol dependence, and criminal recidivism conferred risk of being murdered. CONCLUSIONS: To the authors’ knowledge, this is the first report of traumatic brain injury, in both men and women, as a risk factor for being murdered. Brain injury may mark risk-taking behavior in general or may cause provocative behavior.
This study was undertaken to identify factors contributing to the risk of being murdered in Sweden. The demographic characteristics of the Nordic populations may yield factors other than those true for the United States. There are national health insurance and comprehensive social support systems, immigration is regulated, and the populations were until recently almost entirely Caucasian. Cocaine is hardly available, and handguns are not as common as in the United States. The motives for homicide are similar to those in other cultures: anger during a drunken altercation, jealousy, and revenge (1, 2). Most victims are killed by their spouses or acquaintances, and usually both the victim and perpetrator are inebriated. Homicide followed by suicide of the perpetrator seems more common than in the United States, perhaps because of the higher proportion of mentally deranged perpetrators in Sweden (3).
The annual homicide rates per 100,000 adults in 1994 were 4.1 in Finland, 2.2 in Denmark, 1.6 in Norway, and 2.7 in Sweden, compared to 9.4 in the United States (4). Wikstr�(5) reported that the higher homicide rate in Philadelphia than in Stockholm during the 1950s was due to intraracial black homicides (6). Twelve times as many homicides were committed with a weapon in Philadelphia as in Stockholm. Homicides provoked by the victim’s behavior occurred in 26% of the Philadelphia cases, compared to 11% in Stockholm (6). In a matched case-control study of all 820 cases of firearm injuries in Stockholm over 20 years, murder or attempted murder was the motive in 21% (7). The homicide rate in Sweden after 1955 has been correlated with the consumption of spirits at home; the attributable fraction has been estimated to be 50% (8).
The typical risk factors for being murdered in U.S. metropolitan areas are male sex, youth, black or Hispanic ethnicity, household crowding, homelessness, inebriation, drug dealing, handguns, and just living in an environment with these elements (9–17).
Our study was undertaken to identify health and social characteristics conferring risk of being murdered in Sweden. There are about 120 criminal homicides per year in a population of 8.6 million, i.e., 1.0 per 100,000 men and 0.5 per 100,000 women. All consecutive adult cases over 16 years were included. We hypothesized that substance abuse, criminality, and immigrant status would be independent risk factors for being murdered in Sweden.
METHOD
All 1,739 persons 18 years and older who resided in Sweden in 1978 and were murdered through 1994 were identified (criminal homicides: ICD E960–E969 as recorded in the national Cause-of-Death Register).
On the basis of sex, year, and month of birth, 1,024 strata were formed within the total Swedish population on Dec. 31, 1977, to find six comparison persons for each homicide victim. Random selection within the strata was performed by means of SAS software (SAS Institute, Cary, N.C.), resulting in a data file with 12,173 persons. Their personal identification numbers were used to retrieve data from a national crime register, from the immigration register, and from the national inpatient register (Statistics Sweden and the National Board of Health and Welfare). The means of personal identification were then removed from the file.
The variables used were sex, year and month of birth and homicide, marital status in December 1977, country of birth, number of criminal court sentences, and inpatient diagnoses between January 1978 and December 1994. The ICD diagnoses from a total of 30,855 hospital admissions were divided into 10 categories reflecting substance abuse, suicide attempts, other psychiatric disorders, brain injuries, and physical abuse.
To permit adjustment for time of exposure, i.e., time to homicide, the comparison persons had to remain alive at least as long as the homicide victims. Univariate and multivariate analyses were performed with conditional logistic regression on the matched pairs (18).
RESULTS
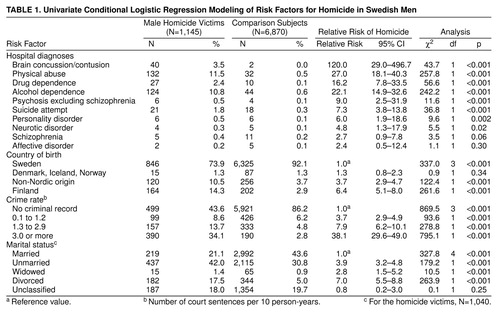
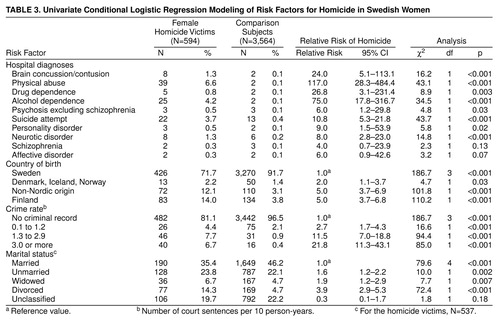
Of the 1,739 homicide victims, 1,145 were men and 594 women. The most frequent diagnoses in both sexes were physical abuse and alcohol dependence. Finland was the most common country of origin after Sweden. Only 21.1% of the men and 35.4% of the women were married when they were killed. A criminal record was found for 56.4% of the men and 18.9% of the women, as compared to 13.8% for the comparison men and 3.4% of the comparison women.
In the univariate model for male homicide victims, the highest relative risks were admission for traumatic brain injury, a high crime rate, and diagnoses of physical abuse, alcohol dependence, and drug dependence (table 1). All of these except drug dependence remained statistically significant in the multivariate model (table 2).
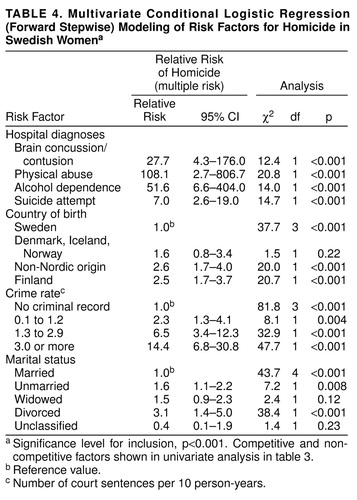
In the univariate model for female homicide victims, the highest risks were physical abuse, alcohol dependence, drug dependence, brain injury, and a high crime rate (table 3). As for the men, all of these except drug dependence remained significant in the multivariate model (table 4).
DISCUSSION
The study identified traumatic brain injury as a risk factor for being murdered. This is the first such report, to our knowledge. The study also identified other expected risks, such as crime recidivism, physical abuse, and substance abuse.
The results were not confounded by race. All homicide cases during 16 years were included, and the risks were estimated by comparing the victims with matched persons and controlling for length of exposure. Errors due to mistaken identities, missing records, or faulty entries in the registries are negligible. The diagnoses were made routinely in public inpatient settings. The diagnoses of brain injury and physical abuse were based on physical examinations, X-rays, and witness accounts in cases of such severity that inpatient care was warranted. One limitation of the study is the absence of police reports including forensic examinations.
We have no knowledge of the behavior of the victims at the time of killing. Evolutionary psychologists view homicide as an extreme manifestation of interpersonal conflict or character contest, especially within the family (19, 20). Criminologists find conflicting results in classifying victim-offender relationships (21). Tiihonen et al. (22) proposed that the seasonal variation of the homicide rate in Finland parallels that of variations in CNS serotonin transmission, an impetus for neurophysiological studies of the matter.
Why are brain injuries conducive to homicide? According to one estimate (23), 1.5 million U.S. residents, mostly young males, sustained nonfatal brain injuries in 1991. A traumatic brain injury may cause long-term irritability, agitation, belligerence, anger, episodic dyscontrol, and inappropriate social responses (24). Retrospective and prospective studies suggest that traumatic brain injury may be associated with criminal and violent behavior (25), but to our knowledge, no prior study has elucidated an association with homicide. It seems plausible that aggressive and persevering behavior, compounded by alcohol inebriation, may provoke homicidal acts for trivial reasons in an environment characterized by crime, substance abuse, and poverty.
Received Feb. 9, 1999; revision received May 4, 1999; accepted July 23, 1999. From Neurotec, Division for Psychiatry, and the Division of Cancer Epidemiology at Radiumhemmet, Karolinska Institutet, Stockholm. Address reprint requests to Dr. Allgulander, M57 Huddinge Hospital, S-141 86 Huddinge, Sweden; [email protected] (e-mail). Supported by research grants from the Karolinska Institutet and the S�str��ska Foundation. The data file was compiled by the Center for Epidemiology at the Swedish National Board of Health and Welfare and by Statistics Sweden.
 |
 |
 |
 |
1. Gudjò²³on GH, Pè³µrsson H: Homicide in the Nordic countries. Acta Psychiatr Scand 1990; 82:49–54Crossref, Medline, Google Scholar
2. Lindqvist P: Homicides committed by abusers of alcohol and illicit drugs. Br J Addiction 1991; 86:321–326Crossref, Medline, Google Scholar
3. Lindqvist P, Gustafsson L: Homicide followed by the offender’s suicide in northern Sweden. Nord J Psychiatry 1995; 49:17–24Crossref, Google Scholar
4. Yearbook of Nordic Statistics 1996. Stockholm, Statistiska Centralbyr䬬 1997Google Scholar
5. Wikstr�-O: Cross-national comparisons and context-specific trends in criminal homicide. J Crime Justice 1991; 14:71–95Crossref, Google Scholar
6. Wolfgang ME: Victim precipitated criminal homicide. J Criminal Law, Criminology, and Police Science 1957; 48:1–11Crossref, Google Scholar
7. Ponzer S, Bergman B, Brismar B: Morbidity and injury recurrence in victims of firearm injuries. Public Health 1996; 110:42–46Crossref, Medline, Google Scholar
8. Norstr�: Effects on criminal violence of different beverage types and private and public drinking. Addiction 1998; 93:689–699Crossref, Medline, Google Scholar
9. Centerwall BS: Race, socioeconomic status, and domestic homicide, Atlanta, 1971–72. Am J Public Health 1984; 74:813–815Crossref, Medline, Google Scholar
10. Goodman RA, Mercy JA, Loya F, Rosenberg ML, Smith JC, Allen NH, Vargas L, Kolts R: Alcohol use and interpersonal violence: alcohol detected in homicide victims. Am J Public Health 1986; 76:144–149Crossref, Medline, Google Scholar
11. Kellerman AL, Mercy JA: Men, women, and murder: gender-specific differences in rates of fatal violence and victimization. J Trauma 1992; 33:1–5Crossref, Medline, Google Scholar
12. Tardiff K, Marzuk PM, Leon AC, Hirsch CS, Stajic M, Portera L, Hartwell N: Cocaine, opiates, and ethanol in homicides in New York City:1990 to 1991. J Forensic Sci 1995; 40:387–390Google Scholar
13. Kennedy BP, Kawachi I, Prothrow-Stith D: Income distribution and mortality: cross sectional ecological study of the Robin Hood index in the United States. Br Med J 1996; 312:1004–1007Google Scholar
14. Rivara FP, Mueller BA, Somes G, Mendoza CT, Rushforth NB, Kellermann AL: Alcohol and illicit drug abuse and the risk of violent death in the home. JAMA 1997; 278:569–575Crossref, Medline, Google Scholar
15. Hwang SW, Orav EJ, O’Connell JJ, Lebow JM, Brennan TA: Causes of death in homeless adults in Boston. Ann Intern Med 1997; 126:625–628Crossref, Medline, Google Scholar
16. Ikeda RM, Gorwitz R, James SP, Powell KE, Mercy JA: Trends in fatal firearm-related injuries, United States, 1962–1993. Am J Prev Med 1997; 13:396–400Crossref, Medline, Google Scholar
17. Bailey JE, Kellerman AL, Somes GW, Banton JG, Rivara FP, Rushforth NP: Risk factors for violent death of women in the home. Arch Intern Med 1997; 157:777–782Crossref, Medline, Google Scholar
18. Breslow NE, Day NE: Statistical Methods in Cancer Research, vol 1: The Analysis of Case-Control Studies: International Agency for Research on Cancer Scientific Publication 32. Lyons, France, International Agency for Research on Cancer, 1980Google Scholar
19. Daly M, Wilson M: Homicide. New York, Aldine de Gruyter, 1988Google Scholar
20. Savitz LD, Kumar KS, Zahn MA: Quantifying Luckenbill. Deviant Behav 1991; 12:19–29Crossref, Google Scholar
21. Decker SH: Exploring victim-offender relationships in homicide: the role of individual and event characteristics. Justice Quarterly 1993; 10:585–612Crossref, Google Scholar
22. Tiihonen J, Rasanen P, Hakko H: Seasonal variation in the occurrence of homicide in Finland. Am J Psychiatry 1997; 154:1711–1714Google Scholar
23. Sosin DM, Sniezek JE, Thurman DJ: Incidence of mild and moderate brain injury in the United States, 1991. Brain Inj 1996; 10:47–54Crossref, Medline, Google Scholar
24. Prigatano GP: Personality disturbances associated with traumatic brain injury. J Consult Clin Psychol 1992; 60:360–368Crossref, Medline, Google Scholar
25. Volavka J: Neurobiology of Violence. Washington, DC, American Psychiatric Press, 1995Google Scholar

