
A Randomized, Double-Blind, Placebo-Controlled Trial of Quetiapine in the Treatment of Bipolar I or II Depression
Abstract
OBJECTIVE: There is a major unmet need for effective options in the treatment of bipolar depression. METHOD: Five hundred forty-two outpatients with bipolar I (N=360) or II (N=182) disorder experiencing a major depressive episode (DSM-IV) were randomly assigned to 8 weeks of quetiapine (600 or 300 mg/day) or placebo. The primary efficacy measure was mean change from baseline to week 8 in the Montgomery-Åsberg Depression Rating Scale total score. Additional efficacy assessments included the Hamilton Depression Rating Scale, Clinical Global Impression of severity and improvement, Hamilton Anxiety Rating Scale, Pittsburgh Sleep Quality Index, and Quality of Life Enjoyment and Satisfaction Questionnaire. RESULTS: Quetiapine at either dose demonstrated statistically significant improvement in Montgomery-Åsberg Depression Rating Scale total scores compared with placebo from week 1 onward. The proportions of patients meeting response criteria (≥50% Montgomery-Åsberg Depression Rating Scale score improvement) at the final assessment in the groups taking 600 and 300 mg/day of quetiapine were 58.2% and 57.6%, respectively, versus 36.1% for placebo. The proportions of patients meeting remission criteria (Montgomery-Åsberg Depression Rating Scale ≤12) were 52.9% in the groups taking 600 and 300 mg/day of quetiapine versus 28.4% for placebo. Quetiapine at 600 and 300 mg/day significantly improved 9 of 10 and 8 of 10 Montgomery-Åsberg Depression Rating Scale items, respectively, compared to placebo, including the core symptoms of depression. Treatment-emergent mania rates were low and similar for the quetiapine and placebo groups (3.2% and 3.9%, respectively). CONCLUSIONS: Quetiapine monotherapy is efficacious and well tolerated for the treatment of bipolar depression.
Depressive episodes in bipolar I and II disorder are an important source of morbidity and mortality. While symptomatic, patients with bipolar I disorder experience depressive symptoms for about threefold longer than manic symptoms, and the recovery time is considerably longer for depressive than manic episodes (1–4). Symptomatic patients with bipolar II disorder spend almost 40 times longer depressed than hypomanic patients (5). Bipolar depression is associated with high rates of disability (6) and an increased risk of suicide, which occurs in 10% to 20% of patients with bipolar disorder (7).
Although multiple agents, including several atypical antipsychotics, have demonstrated efficacy in the treatment of the manic phase of bipolar I disorder (8), the acute treatment of bipolar depression has not been as well studied (9). Lithium and lamotrigine are recommended as initial treatments for acute bipolar I depression (10, 11). However, the response of bipolar depression to lithium is often incomplete in a substantial proportion of patients (12), and the efficacy of lamotrigine in the treatment of acute bipolar I depression has only been demonstrated in one adequately powered placebo-controlled trial (13).
More recently, the atypical antipsychotic olanzapine was found to be superior to placebo in the treatment of acute bipolar I depression as monotherapy when data were pooled from two 8-week trials (14). Fixed doses of olanzapine in combination with the antidepressant fluoxetine were administered to small groups of patients in these studies and were found to be both superior to placebo and superior to olanzapine monotherapy.
Quetiapine is efficacious in the treatment of acute bipolar mania, both as monotherapy and in combination with other mood stabilizers (15, 16). Preliminary evidence for the efficacy of quetiapine in the treatment of depressive symptoms in a variety of psychotic and mood disorders (including bipolar disorder, rapid-cycling bipolar disorder, and adolescent mania) has been reported in several randomized or open-label studies (17–24).
Based on the need for new treatment options for bipolar depression, the effectiveness of atypical antipsychotics in acute mania, and the emerging evidence for their use in bipolar depression, we evaluated the efficacy and safety of quetiapine compared with placebo in the treatment of depressive episodes in patients with bipolar I or bipolar II disorder.
Method
This double-blind, randomized, fixed-dose, placebo-controlled, parallel-group monotherapy study of quetiapine versus placebo was conducted at 39 centers in the United States between September 2002 and October 2003. After a washout period of at least five half-lives of any prior psychotropic medications, subjects were treated for 8 weeks to evaluate the efficacy, safety, and tolerability of 600 and 300 mg/day of quetiapine and placebo in the treatment of depressive episodes in adult patients with bipolar I or II disorder.
The study was approved by institutional review boards for each site and performed in accordance with the current amendment of the Declaration of Helsinki and the International Conference on Harmonization/Good Clinical Practice guidelines. Written informed consent was obtained from all subjects before participation.
Patient Population
Outpatients ages 18 to 65 years who met DSM-IV criteria for bipolar I or II disorder and were experiencing a major depressive episode were eligible for inclusion in the study. The diagnosis was confirmed with the Structured Clinical Interview for DSM-IV. The patients were required to have a Hamilton Depression Rating Scale 17-item score ≥20 (25), a Hamilton depression scale item 1 score ≥2, and a Young Mania Rating Scale (26) score ≤12 at both the screening and randomization visits. Inclusion criteria were based on the Hamilton depression scale rather than the primary efficacy measure (the Montgomery-Åsberg Depression Rating Scale [27]).
Patients were excluded from the study if they were diagnosed with an axis I disorder other than bipolar disorder that was the primary focus of treatment within 6 months before the screening, if the current episode of depression exceeded 12 months or was less than 4 weeks in duration, or if they had a history of nonresponse to an adequate (6-week) trial of more than two classes of antidepressants during the current episode. Additional exclusion criteria included a diagnosis of substance dependence (DSM-IV) or substance use (except for nicotine) within 12 months before the screening or a clinically significant medical illness. Patients who posed a current serious suicidal or homicidal risk were also excluded. Patients were not permitted to take benzodiazepines during the washout period, and only limited use was permitted during the first 3 weeks after random assignment.
Random assignment was achieved in a non-center-specific manner with an interactive voice-response central randomization service. Random assignment was stratified according to bipolar type (I or II) to ensure a relative balance in the total number of patients among groups (1:1:1). The patients were randomly assigned to one of three groups: quetiapine, 600 mg/day; quetiapine, 300 mg/day; or placebo.
Study Medication
Quetiapine (600 mg/day or 300 mg/day) or placebo was administered orally, in a single dose, once a day at bedtime. Quetiapine was initiated at 50 mg/day and administered to achieve a target dose of 300 mg/day by day 4 or 600 mg/day by week 1. All packaging of treatments was identical, with placebo and active tablets identical in appearance and number.
Prior and Concomitant Medication
Nonpsychotropic medication, including over-the-counter medications taken before entry into the study could be continued. Zolpidem tartrate (5–10 mg/day at bedtime for insomnia) and lorazepam (1–3 mg/day for severe anxiety) were permitted at the discretion of the investigator and only during the first 3 weeks of treatment but were withheld for 8 hours before psychiatric assessments were conducted. The use of all other psychotropic drugs was prohibited during the study.
Efficacy Evaluations
Clinical assessments were conducted at baseline and weekly from weeks 1 to 8. The primary efficacy variable was the mean change in the Montgomery-Åsberg Depression Rating Scale total score from baseline to week 8 (27).
Additional efficacy evaluations included a change from baseline to each assessment on the Montgomery-Åsberg Depression Rating Scale, the proportion of patients who achieved a protocol-defined response (≥50% reduction from baseline score on the Montgomery-Åsberg Depression Rating Scale), the time to response, the proportion of patients who achieved remission (Montgomery-Åsberg Depression Rating Scale score ≤12), the time to remission, as well as a Montgomery-Åsberg Depression Rating Scale item analysis. The change from baseline to each assessment on the Hamilton depression scale, the Clinical Global Impression (CGI) (28) severity of illness score, and the CGI improvement score were also assessed.
The effect of quetiapine on anxiety symptoms was assessed with the Hamilton Anxiety Rating Scale (29). Mean change from baseline to each assessment and at week 8 in the Hamilton anxiety scale total score was determined.
Quality of sleep was assessed with the Pittsburgh Sleep Quality Index, which measures several dimensions of sleep, including quality, latency, duration, efficiency, use of medication, and daytime dysfunction (30).
The 16-item short form of the Quality of Life Enjoyment and Satisfaction Questionnaire was used to measure satisfaction with various areas of daily functioning, such as social relationships, living/housing, physical health, medication, and global satisfaction (31). The Pittsburgh Sleep Quality Index and the Quality of Life Enjoyment and Satisfaction Questionnaire were administered at baseline and at weeks 4 and 8.
Safety and Tolerability Evaluations
Safety and tolerability were evaluated by assessing the incidence and severity of adverse events, as well as withdrawals because of adverse events. Extrapyramidal symptoms were assessed with the Simpson-Angus Rating Scale (32), and akathisia was assessed with the Barnes Rating Scale for Drug-Induced Akathisia (33) at random assignment and at week 8. Measurements of vital signs, including weight and fasting serum glucose levels, were obtained at each study visit. Twelve-lead ECGs, clinical chemistry, and hematology assessments were performed at the screening and at week 8.
The incidence of treatment-emergent mania was evaluated by comparing the percentage of patients in each group who had a total Young Mania Rating Scale score of ≥16 on any two consecutive visits or at the final assessment, or an adverse event of mania or hypomania.
Statistical Analyses
Primary and secondary efficacy analyses were performed on the intent-to-treat population, which included all randomly assigned patients who took at least one dose of study medication and had at least one postbaseline efficacy assessment. A last-observation-carried-forward analysis was used to impute missing data for patients who withdrew during the study. All statistical tests were two-tailed. The primary analysis of change from baseline to final assessment in the Montgomery-Åsberg Depression Rating Scale total scores tested the superiority of each dose of quetiapine in the intent-to-treat group (patients with bipolar I or bipolar II disorder) with an analysis of covariance (ANCOVA) with the baseline Montgomery-Åsberg Depression Rating Scale as the covariate and included treatment and diagnosis strata as fixed effects in the model, with adjustment for multiple comparisons. Effect size (improvement of quetiapine over placebo divided by pooled standard deviation) was determined with a mixed-model repeated-measures analysis.
Differences in response rates between treatment and placebo groups and in patients with and without rapid cycling were assessed with a Cochran-Mantel-Haenszel chi-square test across diagnostic strata. Hamilton depression scale, CGI severity and improvement, Young Mania Rating Scale, Hamilton anxiety scale, Pittsburgh Sleep Quality Index, and Quality of Life Enjoyment and Satisfaction Questionnaire scores were tested with ANCOVAs. All secondary analyses were conducted at the nominal significance level of 0.05, with no adjustment for multiple comparisons.
Sample sizes were determined to provide 85% power to detect a difference of 3.6 points on the Montgomery-Åsberg Depression Rating Scale with two-tailed pairwise comparisons between treatment groups and placebo at an alpha level of 0.025 in the intent-to-treat population (patients with bipolar I or bipolar II disorder).
Exploratory analyses were carried out on the bipolar I and II subgroups whose group size was not predetermined to provide power for significance testing. Exploratory analyses were limited to descriptions of the mean changes in primary outcome measure across the three treatment groups, and effect size determinations for the groups taking 600 and 300 mg/day of quetiapine. The repeated measures mixed-effects model included terms for treatment, bipolar diagnosis, treatment-by-bipolar diagnosis, baseline Montgomery-Åsberg Depression Rating Scale total score, visit (week), and treatment-by-visit effects. Several covariance structures were examined, including autoregressive, banded Toeplitz, compound symmetry, and unstructured. The best-fitting covariance structure, the banded Toeplitz, was determined with the Bayesian information criterion.
Results
Patients and Disposition
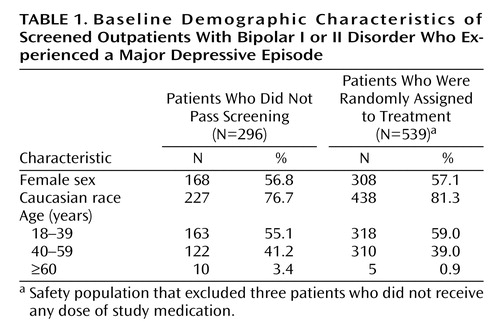
A total of 838 patients were screened, and 542 patients with bipolar I (N=360) or bipolar II (N=182) disorder were randomly assigned to receive quetiapine, 600 mg/day (N=180); quetiapine, 300 mg/day (N=181); or placebo (N=181). There were no significant differences between the baseline characteristics of patients who did not pass the screening compared with those who were randomly assigned (Table 1). The most common reason for the screening failure was failure to meet eligibility criteria. Figure 1 illustrates the disposition of patients during the study. Of the 542 randomly assigned patients, 539 received at least one dose of study medication and were included in the safety population. Of these, 511 had at least one postbaseline assessment and were analyzed for efficacy in the intent-to-treat population.
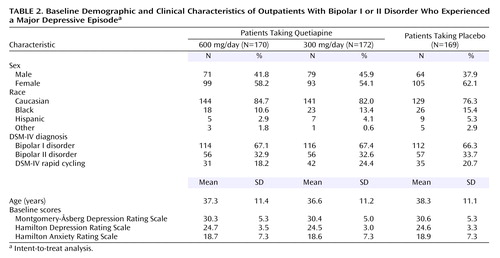
There were no statistically significant differences between treatment groups with respect to any demographic and baseline disease characteristic (Table 2). The mean age was approximately 37 years, and 58.2% of the patients were women. Mean Montgomery-Åsberg Depression Rating Scale scores at baseline were consistent with moderate to severe depression (34).
There were no statistically significant differences between the quetiapine groups and placebo in the proportion of the patients who completed the study: 54% in the 600 mg/day quetiapine group, 67% in the 300 mg/day quetiapine group, and 59% in the placebo group. The most common reasons for withdrawal were related to adverse events in the quetiapine groups (26.1% and 16.0%) and lack of efficacy in the placebo group (13.3%).
The use of lorazepam and zolpidem (permitted during the first 3 weeks of the study) was generally low across groups. Lorazepam use during the study was 5.6% and 9.5% in the 600 and 300 mg/day quetiapine groups, respectively, compared with 8.3% in the placebo group. Zolpidem use during the study was 6.7% and 4.5% in the 600 and 300 mg/day quetiapine groups, respectively, compared with 8.3% in the placebo group.
Efficacy
Montgomery-Åsberg Depression Rating Scale
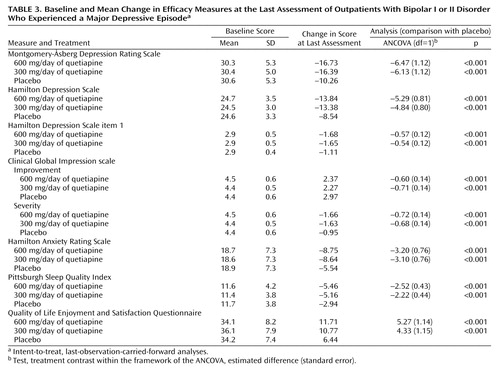
Mean baseline Montgomery-Åsberg Depression Rating Scale scores were 30.3 (SD=5.3), 30.4 (SD=5.0), and 30.6 (SD=5.3) in the 600 mg/day, 300 mg/day, and placebo groups, respectively. Quetiapine at a dose of either 600 or 300 mg/day demonstrated significantly greater mean improvement in Montgomery-Åsberg Depression Rating Scale total scores compared with placebo as early as week 1 and at all time points that followed in the intent-to-treat group of patients with bipolar I or II depression (p<0.001 for both quetiapine doses versus placebo) (Figure 2). The mean change in Montgomery-Åsberg Depression Rating Scale total score from baseline to last assessment was –16.73 in the 600 mg/day group and –16.39 in the 300 mg/day group, compared with –10.26 in the placebo group (p<0.001 for both quetiapine doses versus placebo) (Table 3, Figure 2). The effect sizes were 0.81 for 600 mg/day and 0.67 for 300 mg/day of quetiapine.
Approximately 58% of the patients treated with either dose of quetiapine were responders at the final assessment, and both doses resulted in significantly higher response rates than placebo (36.1%) (p<0.001). Notably, the percentage of patients meeting response criteria with 600 mg/day of quetiapine was significantly higher as early as week 1 (24.3%) versus placebo (10.7%) (p<0.001). In the group taking 300 mg/day of quetiapine, a significantly higher response rate (37.2%) versus placebo (19.5%) was apparent by week 2 (p<0.001). The median time to response was significantly shorter for both 600 mg/day (22 days) and 300 mg/day (22 days) of quetiapine compared with placebo (36 days) (log-rank χ2=33.1, df=2, p<0.001).
The percentage of patients meeting remission criteria at the final assessment was 52.9% in both the groups taking 600 and 300 mg/day of quetiapine, significantly higher than the placebo rate of 28.4% in each group (p<0.001). The median time to remission was significantly shorter for both 600 mg/day (27 days) and 300 mg/day (29 days) of quetiapine compared with placebo (65 days) (log-rank χ2=32.8, df=2, p<0.001).
Nine out of 10 Montgomery-Åsberg Depression Rating Scale items were significantly improved from baseline compared with placebo in the 600 mg/day quetiapine group, as were eight items in the 300 mg/day quetiapine group (p<0.05) (Figure 3). With both doses of quetiapine, these items included the core mood symptoms of apparent sadness, reported sadness, inability to feel, pessimistic thoughts, and suicidal thoughts. The core mood symptoms of apparent sadness, reported sadness, and pessimistic thoughts were significantly improved in both quetiapine groups as early as week 1 compared with placebo (p<0.05). An inability to feel and suicidal thoughts were also significantly improved by week 1 in the group taking 600 mg/day of quetiapine compared with placebo (p<0.05). Both doses of quetiapine were more effective than placebo in reducing suicidal thoughts at the final assessment (p≤0.001); the reductions with quetiapine were approximately twice that of placebo.
In the bipolar I subgroup of patients, the mean change in Montgomery-Åsberg Depression Rating Scale total score from baseline to last assessment was –18.05 in the group taking 600 mg/day group of quetiapine and –16.91 in the 300 mg/day group, compared with –9.24 in the placebo group (p<0.001 for both quetiapine doses versus placebo). The effect size in the bipolar I subgroup was 1.09 for those assigned to 600 mg/day and 0.91 for those taking 300 mg/day of quetiapine. In the subgroup of patients with bipolar II disorder, the mean change in Montgomery-Åsberg Depression Rating Scale total score from baseline to last assessment was smaller than in bipolar I patients. Although the change in Montgomery-Åsberg Depression Rating Scale total score from baseline in the patients with bipolar II disorder was statistically superior to placebo at most assessments, it did not reach statistical significance at the final assessment: –14.06 in the group taking 600 mg/day of quetiapine and –14.78 in the group taking 300 mg/day compared with –12.35 in the placebo group. The effect size in the bipolar II subgroup was 0.39 in the 600 mg/day group and 0.28 in the 300 mg/day group.
Significant improvement in Montgomery-Åsberg Depression Rating Scale total scores compared with placebo at the final assessment occurred with quetiapine treatment regardless of the presence of rapid cycling in the intent-to-treat group (patients with bipolar I or II disorder). The mean change in Montgomery-Åsberg Depression Rating Scale total score at week 8 in the patients with rapid cycling was –17.7 in the 600 mg/day quetiapine group and –18.6 in the 300 mg/day quetiapine group versus –9.9 in the placebo group (p<0.01 for both quetiapine doses versus placebo). The mean change in Montgomery-Åsberg Depression Rating Scale total score at week 8 in the patients without rapid cycling was –16.6 in the 600 mg/day group and –15.7 in the 300 mg/day group versus –10.3 in the placebo group (p<0.001 for both quetiapine doses versus placebo). A more detailed analysis of patients with and without rapid cycling in this study will be described in a separate report.
In order to explore the role of somnolence or sedation on efficacy, the mean change from baseline in Montgomery-Åsberg Depression Rating Scale total scores in the patients with and without these adverse events were compared. The number of patients in the intent-to-treat group with reported somnolence/sedation was 195 (57%) for the quetiapine groups combined and 24 (14%) for the placebo group. The mean change in the Montgomery-Åsberg Depression Rating Scale total score at week 8 in the patients with somnolence/sedation (either bipolar I or II disorder) was –18.8 in the pooled quetiapine groups (600 or 300 mg/day) versus –18.9 in the placebo group. In the patients without somnolence/sedation, the mean change in the Montgomery-Åsberg Depression Rating Scale total score was –19.3 and –11.7 for in the pooled quetiapine and placebo groups, respectively. The placebo group response was higher in the patients reporting somnolence/sedation, but the results with quetiapine were similar in the patients with or without somnolence/sedation.
Hamilton depression scale
Mean baseline Hamilton depression scale scores were 24.7 (SD=3.5), 24.5 (SD=3.0), and 24.6 (SD=3.3) in the 600 mg/day, 300 mg/day, and placebo groups, respectively (Table 3). Quetiapine at a dose of either 600 or 300 mg/day demonstrated significantly greater mean improvements in Hamilton depression scale total scores compared to placebo as early as week 1 and at all time points that followed in the patients with bipolar I or II depression (p<0.001). The mean change from baseline in Hamilton depression scale scores at week 8 was –13.84, –13.38, and –8.54 in the 600 mg/day, 300 mg/day, and placebo groups, respectively (p<0.001 for both quetiapine doses versus placebo). At the end of the study, the effect sizes for the group of patients with bipolar I or II disorder with the Hamilton depression scale was 0.93 for 600 mg/day and 0.74 for 300 mg/day of quetiapine.
Significant improvement in the Hamilton depression scale item 1 (depressed mood) was as early as week 1 (p=0.003) for both quetiapine doses and continued to be statistically superior to placebo at all time points.
Clinical Global Impression
Quetiapine-treated patients experienced a statistically significant improvement (p<0.001) on the CGI severity scale as early as week 1 that was sustained to the end of the study for both quetiapine doses versus placebo. At the final assessment, a larger percentage of patients were rated as “normal, not at all ill,” or “borderline ill” in the 600 mg/day (42.4%) and 300 mg/day quetiapine groups (38.1%) compared with the placebo group (23.7%).
A larger percentage of patients was also rated as “much” or “very much” improved on the CGI improvement scale in the 600 mg/day (55.9%) and 300 mg/day quetiapine groups (64.0%) compared with the placebo group (34.3%) at the final assessment.
Anxiety symptoms
Mean baseline Hamilton anxiety scale scores were 18.7 (SD=7.3), 18.7 (SD=7.3), and 18.9 (SD=7.3) in the 600 mg/day, 300 mg/day, and placebo groups, respectively (Table 2). By the study end, the mean Hamilton anxiety scale total score had decreased by –8.75 in the 600 mg/day group, –8.64 in the 300 mg/day group, and –5.54 in the placebo group (p<0.001 for both quetiapine doses versus placebo). A significant improvement in the Hamilton anxiety scale total scores as early as week 1 (p<0.05) was maintained to the last assessment (p<0.001 for both quetiapine doses versus placebo). Individual items of the Hamilton anxiety scale that most differentiated quetiapine-treated patients from those who received placebo included anxious mood, depressed mood, insomnia, genitourinary symptoms, and tension. A more detailed analysis of the results of the effect of quetiapine on anxiety measures in this study has been presented in a separate report (35).
Quality of sleep
The quality of sleep improved significantly among those treated with either dose of quetiapine compared with placebo. The mean improvement in Pittsburgh Sleep Quality Index scores from baseline in patients treated with 600 mg/day (–5.46) and 300 mg/day (–5.16) of quetiapine was significantly greater with both doses (p<0.001) than with placebo (–2.94).
Quality of life
Quetiapine-treated patients also experienced statistically significant improvements in quality of life during the study, as determined by the change from baseline in the Quality of Life Enjoyment and Satisfaction Questionnaire total scores. Mean Quality of Life Enjoyment and Satisfaction Questionnaire total scores improved by 11.71 by the last assessment among patients treated with 600 mg/day of quetiapine and by 10.77 among those treated with 300 mg/day of quetiapine, compared with 6.44 in the placebo group (p<0.001 for both quetiapine doses versus placebo).
Safety and Tolerability
Adverse events
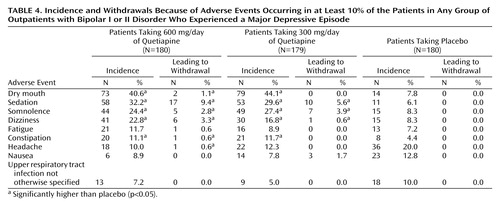
Common adverse events (whether or not considered treatment related) occurred in ≥10% of patients, and withdrawals due to common adverse events are shown in Table 4. The overall rate of study discontinuation due to adverse events was 26.1% (N=47) in the 600 mg/day group, 16.0% (N=29) in the 300 mg/day group, and 8.8% (N=16) in the placebo group (Figure 1). There were no significant differences in the rates of serious adverse events across treatment groups, and none was treatment related: 5.0% (N=9) in the 600 mg/day group and 3.4% (N=6) in the 300 mg/day group compared with 8.9% (N=16) in the placebo group. Two patients attempted suicide (one in each of the active treatment groups), but no suicides or deaths occurred during the study.
The rate of discontinuation due to adverse events in the subgroup of patients with bipolar I disorder was 23.3% (N=28) in the 600 mg/day group, 13.1% (N=16) in the 300 mg/day group, and 11.9% (N=14) in the placebo group. The incidence of serious adverse events in the subgroup of patients with bipolar I disorder was 5.0% (N=6) in the 600 mg/day group, 4.2% (N=5) in the 300 mg/day group, and 11.9% (N=14) in the placebo group.
In the subgroup of patients with bipolar II disorder, the rate of discontinuation due to adverse events was 31.7% (N=19) in the 600 mg/day group, 22.0% (N=13) in the 300 mg/day group, and 3.2% (N=2) in the placebo group. The incidence of serious adverse events in the subgroup of patients with bipolar II disorder was 5.0% (N=3) in the 600 mg/day group, 1.7% (N=1) in the 300 mg/day group, and 3.2% (N=2) in the placebo group.
The incidence of treatment-emergent mania was low and not significantly different from placebo at either quetiapine dose: 2.2% with 600 mg/day of quetiapine (Cochran-Mantel-Haenszel, odds ratio=0.57, 95% confidence interval (CI)=0.17–1.91, p=0.35), 3.9% with 300 mg/day of quetiapine (Cochran-Mantel-Haenszel, odds ratio=0.97, 95% CI=0.35–2.68, p=0.95), and 3.9% with placebo.
The mean Simpson-Angus Rating Scale total score decreased in all three groups from baseline to the final assessment by –0.1, –0.2, and –0.3 in the 600 mg/day and 300 mg/day quetiapine groups and the placebo groups, respectively. There was no statistically significant difference in the number of patients with an increase from baseline in Simpson-Angus Rating Scale scores between either of the quetiapine groups and placebo: 15% (logistic regression=0.66, df=3, p<0.08), 9% (logistic regression=0.06, df=3, p=0.89), and 9% in the 600 mg/day and 300 mg/day quetiapine and placebo groups, respectively.
At the last assessment, mean Barnes Rating Scale for Drug-Induced Akathisia scores were low and similar in all groups: 0.3 in the 600 mg/day group, 0.2 in the 300 mg/day group, and 0.1 in the placebo group. There was no statistically significant difference in the number of patients with an increase from baseline in Barnes Rating Scale for Drug-Induced Akathisia score between either of the quetiapine groups and placebo: 12% (logistic regression=0.39, df=3, p=0.31), 9% (logistic regression=0.06, df=3, p=0.89), and 9% in the 600 mg/day and 300 mg/day quetiapine and placebo groups, respectively.
Adverse events considered extrapyramidal symptoms were present in 8.9% of the 600 mg/day group, 6.7% of the 300 mg/day group, and 2.2% of the placebo group; discontinuation rates for extrapyramidal symptoms were 2.8%, 1.1%, and 0.6%, respectively.
Laboratory Results and Vital Signs
No clinically relevant differences between groups were seen in the mean change from baseline for any vital signs, ECGs, hematology, or clinical chemistry parameters.
Patients treated with 600 mg/day of quetiapine experienced a mean weight gain of 1.6 kg by the final assessment compared with 1.0 kg in the 300 mg/kg group and 0.2 kg in the placebo group. At the final assessment, 16 patients (9.0%) treated with 600 mg/day of quetiapine, 15 patients (8.5%) treated with 300 mg/day of quetiapine, and three patients (1.7%) who received placebo had a weight gain of ≥7% of their baseline measurement. No patients withdrew from the study because of weight gain.
Mean fasting serum glucose levels at baseline were 86 (SD=12), 87 (SD=13), and 87 (SD=15) mg/dl in the 600 mg/day and 300 mg/day of quetiapine and placebo groups, respectively. By the final assessment, the mean change in fasting serum glucose was 6 mg/dl (SD=17), 3 mg/dl (SD=13), and 4 mg/dl (SD=26) in the 600 mg/day and 300 mg/day of quetiapine and placebo groups, respectively.
Discussion
To our knowledge, this is the first randomized, parallel-group, placebo-controlled trial to evaluate the efficacy of quetiapine in bipolar depression. It may also be the first published large-scale, controlled study to assess the efficacy of any pharmacological treatment in a group of patients with bipolar I or II depression, and one of few studies to examine an antidepressant effect in patients with rapid cycling.
Quetiapine monotherapy has significant antidepressant efficacy in a group of patients with bipolar I or II depression based on the primary efficacy analysis (mean change in Montgomery-Åsberg Depression Rating Scale total score from baseline to last assessment). The magnitude of the clinical improvement was substantial and evident from the first assessment (week 1) and at each visit thereafter. The rates of response and remission and the time to response and remission were significantly improved in the quetiapine groups compared with placebo. Compared with placebo, evidence of early and sustained efficacy was observed consistently with both doses of quetiapine and in all secondary efficacy analyses from week 1 onward.
In the Montgomery-Åsberg Depression Rating Scale item analysis, both doses of quetiapine produced a significant and early improvement in all of the core mood symptoms of depression, including objective and reported sadness, anhedonia, and pessimistic thoughts. Notably, both doses of quetiapine were approximately twice as effective as placebo in reducing suicidal ideation. These findings provide support for the conclusion that quetiapine has specific antidepressant properties.
In this study, significant antidepressant efficacy was demonstrated for quetiapine dosed once a day in the evening. This has important clinical relevance because once-daily dosing has been associated with enhanced medication adherence (36). Dosing at bedtime may also offer a means of improving tolerability, particularly regarding somnolence or sedation that are sometimes seen with quetiapine and may help treat the sleep disturbance that often accompanies bipolar depression.
Both doses of quetiapine were associated with improvements in quality of sleep and quality of life and were effective in patients with a recent history of rapid-cycling bipolar disorder. Exploratory analyses suggest that the clinical effect of both doses of quetiapine was greater in patients with bipolar I disorder than those with bipolar II disorder.
The most common side effects of quetiapine included dry mouth, sedation, somnolence, dizziness, and constipation. The most common side effects leading to withdrawal from the study were sedation and somnolence, with most discontinuations occurring within the first week. Of importance, changes in weight observed in all three groups were relatively small and did not result in withdrawal from the study. Quetiapine treatment was not associated with treatment-emergent mania. The long-term safety of quetiapine is being explored in ongoing bipolar disorder maintenance studies. However, data from patients with schizophrenia does not suggest that unexpected adverse effects during long-term treatment should be expected (37).
Several aspects of the design of this study were innovative. First, the inclusion of patients with bipolar II disorder into a large-scale study of acute bipolar depression was novel and enhanced the generalizability of the findings, particularly since there is a higher incidence of bipolar II disorder than bipolar I disorder. The inclusion of patients with rapid cycling was also innovative and enhanced the generalizability of the findings to this difficult-to-treat subgroup. Second, rather than focusing solely on depressive symptoms, this study included sleep quality and health-related quality-of-life measures. Sleep-quality assessments (both patient- and bed-partner-rated) indicated improvements in functioning in addition to symptom severity, including several dimensions of sleep quality and daytime dysfunction. The quality-of-life scale provided novel information regarding the effect of quetiapine on social relationships, living/housing arrangements, physical health, satisfaction with medication, and global satisfaction. Improvements in these measures provide evidence for improved function and overall quality of life in addition to reduction in the symptoms of the illness.
Moreover, the inclusion of analyses that quantify the magnitude of the clinical effect through effect size determinations gives clinicians useful information. Knowing if a significant difference is caused by a small clinical effect (<0.4), a moderately sized clinical effect (0.40–0.79), or a large clinical effect (>0.79) has the potential of helping the clinician make decisions on how to use a new medication (38). The effect sizes reported in the bipolar I depression study by Tohen et al. (14) were 0.32 with olanzapine monotherapy and 0.68 with olanzapine-fluoxetine combination therapy compared with 1.09 in the bipolar I subgroup with 600 mg/day of quetiapine in this study.
This study had several limitations. First, the number of enrolled patients with bipolar II disorder was not sufficient to draw firm conclusions regarding efficacy in this subgroup. For this reason, post hoc analyses conducted in the bipolar II subgroup included effect size determinations, which are less affected by sample size than significance testing. Second, moderate rates of sedation or somnolence were observed in both quetiapine groups, which might have compromised the integrity of the double-blind design. If this were a significant factor in the assessment of efficacy, the reduction in Montgomery-Åsberg Depression Rating Scale total score in patients experiencing sedation or somnolence would have been greater than those in patients not experiencing these adverse events. However, this was not the case, and the improvements observed on the Montgomery-Åsberg Depression Rating Scale were comparable in patients with or without sedation or somnolence. Third, although the study indicated that the two doses used—chosen because of their efficacy in bipolar mania and other disorders—were effective, guidance on the best dosing for most patients or subgroups of patients should be assessed in future studies.
In conclusion, this large, randomized, double-blind, placebo-controlled study provides the first pivotal data demonstrating that quetiapine monotherapy is efficacious and well tolerated for the acute treatment of bipolar depression in a group of patients with bipolar I or II disorder.
Acknowledgments
The BOLDER Study Group is as follows: Mohammed Alam, American Med Research, Oak Brook, Ill.; Valerie Arnold, Clinical Neuroscience Solutions, Memphis, Tenn.; Charles Bailey, Clinical Neuroscience Solutions, Orlando, Fla.; Guy Brannon, Brentwood Research Institute, Shreveport, La.; David Brown, Community Clinical Research, Austin, Tex.; Joseph Calabrese, University Hospitals of Cleveland/Case University School of Medicine, Cleveland, Ohio; John Carman, Carman Research, Smyrna, Ga.; Andrew Cutler, CORE Research, Winter Park, Fla.; Bernadette D’Souza, Midwest Clinical Research, Dayton, Ohio; Naresh Emmanuel, Carolina Clinical Research Services, Columbia, S.C.; Lawrence Ginsberg, Red Oak Psychiatry Associates, Houston, Tex.; Ram Gopalan, Comprehensive Neuroscience of Northern VA, Falls Church, Va.; William Granger, Research Strategies, Inc., Reno, Nev.; Laszlo Gyulai, University of Pennsylvania Bipolar Disorder, Philadelphia; Howard Hassman, Comprehensive Clinical Research, Clementon, N.J.; Saul Helfing, Oregon Center for Clinical Investigators, Inc., Lake Oswego, Ore.; George Joseph, Clinical Neuroscience Solutions, Jacksonville, Fla.; Paul Keck, University of Cincinnati, Cincinnati, Ohio; Terrence Ketter, Stanford University Bipolar Disorder Clinic, Stanford, Calif.; Arif Khan, Northwest Medical Research Center, Bellevue, Wash.; Ari Kiev, Social Psychiatry Research Institute, New York, Irving Kolin, Kolin Research Group, Winter Park, Fla.; James Knutson, BHC Fairfax Hospital, Kirkland, Wash.; Michael Levy, Behavioral Medical Research of Staten Island, New York; H.E. Logue, Birmingham Psychiatry Pharmaceutical Services, Inc., Birmingham, Ala.; David Marks, Optimum Health Services, La Mesa, Calif.; Greg Mattingly, St. Charles Psychiatric Association, St. Charles, Mo.; Charles Merideth, Affiliated Research Institute, San Diego, Calif.; Janice Miller, Clinical Neuroscience Solutions, West Palm Beach, Fla.; Dennis Munjack, Southwestern Research, Inc., Beverly Hills, Calif.; William Privitera, Future Search Trials, Austin, Tex.; Fred Reimherr, University of Utah Medical Center, Salt Lake City, Utah; Robert Riesenberg, Atlanta Center for Medical Research, Atlanta, Ga; Leon Rosenberg, Center for Emotional Fitness, Moorestown, N.J.; Leon Rubenfaer, Pioneer Pharmaceutical Research, New Baltimore, Mich.; David Sack, Comprehensive Neuroscience Inc., Cerritos, Calif.; Abbey Strauss, Comprehensive Neuroscience Inc., Boynton Beach, Fla.; David Walling, CNS Network, Garden Grove, Calif.; Richard Weisler, Richard H. Weisler M.D. and Associates, Raleigh, N.C.
 |
 |
 |
 |
Received Aug. 4, 2004; revision received Oct. 28, 2004; accepted Dec. 10, 2004. From the University Hospitals of Cleveland/Case University School of Medicine, Cleveland, Ohio; the Psychopharmacology Research Program, Department of Psychiatry, University of Cincinnati College of Medicine, Cincinnati, Ohio; the Mental Health Care Line and General Clinical Research Center of the Cincinnati Veterans Affairs Medical Center, Cincinnati, Ohio; AstraZeneca, Wilmington, Del.; the Department of Psychiatry and Behavioral Sciences, Stanford University, Stanford, Calif.; the Department of Psychiatry and Behavioral Sciences, Duke University, Raleigh, N.C.; and the Department of Psychiatry and Behavioral Medicine, University of South Florida, Tampa. Address correspondence and reprint requests to Dr. Calabrese, 11400 Euclid Ave., Suite 200, Cleveland, OH 44106; [email protected] (e-mail). Supported by AstraZeneca Pharmaceuticals (grant 5077US/0049). The authors thank Max Brady, D.Phil., and Aruna Seth, Ph.D., (PAREXEL MMS) for editorial assistance. Financial support for their assistance was provided by AstraZeneca.

Figure 1. Disposition of Outpatients with Bipolar I or II Disorder Who Experienced a Major Depressive Episode

Figure 2. Least-Squares Mean Change From Baseline in Montgomery-Åsberg Depression Rating Scale Total Score at Each Assessment of Outpatients With Bipolar I or II Disorder Who Experienced a Major Depressive Episodea
aIntent-to-treat, last-observation-carried-forward analyses. Improvement in Montgomery-Åsberg Depression Rating Scale total score with both doses of quetiapine (600 mg/day and 300 mg/day) was significantly greater than placebo at every assessment (p<0.001).

Figure 3. Mean Percent Change From Baseline in Individual Montgomery-Åsberg Depression Rating Scale Items for Outpatients with Bipolar I or II Disorder Experiencing a Major Depressive Episodea
aIntent-to-treat, last-observation-carried-forward analyses. Nine of 10 and 8 of 10 Montgomery-Åsberg Depression Rating Scale items (including the core mood symptoms of depression [item 1: apparent sadness; item 2: reported sadness; item 8: inability to feel; item 9: pessimistic thoughts; item 10: suicidal thoughts]) were significantly improved from baseline compared to placebo in the groups taking 600 mg/day and 300 mg/day of quetiapine, respectively (p<0.05). Apparent sadness, reported sadness, and pessimistic thoughts were significantly improved in both quetiapine groups as early as week 1 compared with placebo (p<0.05). Both doses of quetiapine were approximately twice as effective as placebo in reducing suicidal thoughts at the final assessment (p≤0.01).
bp<0.001 versus placebo.
cp<0.01.
dp<0.05.
1. Hlastala SA, Frank E, Mallinger AG, Thase ME, Ritenour AM, Kupfer DJ: Bipolar depression: an underestimated treatment challenge. Depress Anxiety 1997; 5:73–83Crossref, Medline, Google Scholar
2. Judd LL, Akiskal HS, Schettler PJ, Endicott J, Maser J, Solomon DA, Leon AC, Rice JA, Keller MB: The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002; 59:530–537Crossref, Medline, Google Scholar
3. Keller MB, Lavori PW, Coryell W, Andreasen NC, Endicott J, Clayton PJ, Klerman GL, Hirschfeld RM: Differential outcome of pure manic, mixed/cycling, and pure depressive episodes in patients with bipolar illness. JAMA 1986; 255:3138–3142Crossref, Medline, Google Scholar
4. Post RM, Denicoff KD, Leverich GS, Altshuler LL, Frye MA, Suppes TM, Rush AJ, Keck PE Jr, McElroy SL, Luckenbaugh DA, Pollio C, Kupka R, Nolen WA: Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003; 64:680–690Crossref, Medline, Google Scholar
5. Judd LL, Akiskal HS, Schettler PJ, Coryell W, Endicott J, Maser JD, Solomon DA, Leon AC, Keller MB: A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003; 60:261–269Crossref, Medline, Google Scholar
6. Altshuler LL, Gitlin MJ, Mintz J, Leight KL, Frye MA: Subsyndromal depression is associated with functional impairment in patients with bipolar disorder. J Clin Psychiatry 2002; 63:807–811Crossref, Medline, Google Scholar
7. Goodwin F, Jamison K: Manic-Depressive Illness. New York, Oxford University Press, 1990Google Scholar
8. Keck PE Jr: The management of acute mania. BMJ 2003; 327:1002–1003Crossref, Medline, Google Scholar
9. Keck PE Jr, Nelson EB, McElroy SL: Advances in the pharmacologic treatment of bipolar depression. Biol Psychiatry 2003; 53:671–679Crossref, Medline, Google Scholar
10. American Psychiatric Association: Practice Guideline for the Treatment of Patients With Bipolar Disorder (Revision). Am J Psychiatry 2002; 159(April suppl)Google Scholar
11. Goodwin GM (Consensus Group of the British Association for Psychopharmacology): Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003; 17:149–173Crossref, Medline, Google Scholar
12. Zornberg GL, Pope HG Jr: Treatment of depression in bipolar disorder: new directions for research. J Clin Psychopharmacol 1993; 13:397–408Crossref, Medline, Google Scholar
13. Calabrese JR, Bowden CL, Sachs GS, Ascher JA, Monaghan E, Rudd GD (Lamictal 602 Study Group): A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. J Clin Psychiatry 1999; 60:79–88Crossref, Medline, Google Scholar
14. Tohen M, Vieta E, Calabrese J, Ketter TA, Sachs G, Bowden C, Mitchell PB, Centorrino F, Risser R, Baker RW, Evans AR, Beymer K, Dube S, Tollefson GD, Breier A: Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression. Arch Gen Psychiatry 2003; 60:1079–1088; correction, 60:176Crossref, Medline, Google Scholar
15. Vieta E, Mullen J, Brecher M, Paulsson B, Jones M: Quetiapine monotherapy for mania associated with bipolar disorder: combined analysis of two international, double-blind, randomised, placebo-controlled studies. Curr Med Res Opin 2005; 21:923–934Crossref, Medline, Google Scholar
16. Sachs G, Chengappa KN, Suppes T, Mullen JA, Brecher M, Devine NA, Sweitzer DE: Quetiapine with lithium or divalproex for the treatment of bipolar mania: a randomized, double-blind, placebo-controlled study. Bipolar Disord 2004; 6:213–223Crossref, Medline, Google Scholar
17. DelBello MP, Schwiers ML, Rosenberg HL, Strakowski SM: A double-blind, randomized, placebo-controlled study of quetiapine as adjunctive treatment for adolescent mania. J Am Acad Child Adolesc Psychiatry 2002; 41:1216–1223Crossref, Medline, Google Scholar
18. Ghaemi SN, Goldberg JF, Henry CA, Rosenquist KJ, Ko JY, Hsu DJ, Wenze SJ, Wankmuller MM: Quetiapine for rapid-cycling bipolar disorder: a long-term follow-up study (abstract). Bipolar Disord 2003; 5(suppl 1):50Google Scholar
19. Post RM, Leverich GS, Altshuler LL, Frye MA, Suppes TM, Keck PE Jr, McElroy SL, Kupka R, Nolen WA, Grunze H, Walden J: An overview of recent findings of the Stanley Foundation Bipolar Network (part I). Bipolar Disord 2003; 5:310–319Crossref, Medline, Google Scholar
20. Sajatovic M, Mullen JA, Sweitzer DE: Efficacy of quetiapine and risperidone against depressive symptoms in outpatients with psychosis. J Clin Psychiatry 2002; 63:1156–1163Crossref, Medline, Google Scholar
21. Sajatovic M, Brescan DW, Periz DE, DiGiovanni SK, Hattab H, Ray JB, Bingham CR: Quetiapine alone and added to a mood stabilizer for serious mood disorders. J Clin Psychiatry 2001; 62:728–732Crossref, Medline, Google Scholar
22. Suppes T, McElroy SL, Keck PE, Altshuler L, Frye MA, Grunze H, Leverich GS, Nolen WA, Chisholm K, Dennehy EB, Post RM: Use of quetiapine in bipolar disorder: a case series with prospective evaluation. Int Clin Psychopharmacol 2004; 19:173–174Crossref, Medline, Google Scholar
23. Vieta E, Parramon G, Padrell E, Nieto E, Martinez-Aran A, Corbella B, Colom F, Reinares M, Goikolea JM, Torrent C: Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002; 4:335–340Crossref, Medline, Google Scholar
24. Zarate CA Jr, Rothschild A, Fletcher KE, Madrid A, Zapatel J: Clinical predictors of acute response with quetiapine in psychotic mood disorders. J Clin Psychiatry 2000; 61:185–189Crossref, Medline, Google Scholar
25. Hamilton M: A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23:56–62Crossref, Medline, Google Scholar
26. Young RC, Biggs JT, Ziegler VE, Meyer DA: A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry 1978; 133:429–435Crossref, Medline, Google Scholar
27. Montgomery SA, Åsberg M: A new depression scale designed to be sensitive to change. Br J Psychiatry 1979; 134:382–389Crossref, Medline, Google Scholar
28. Guy W (ed): ECDEU Assessment Manual for Psychopharmacology: Publication ADM 76–338. Washington, DC, US Department of Health, Education, and Welfare, 1976, pp 218–222Google Scholar
29. Hamilton M: The assessment of anxiety states by rating. Br J Med Psychol 1959; 32:50–55Crossref, Medline, Google Scholar
30. Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ: The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989; 28:193–213Crossref, Medline, Google Scholar
31. Endicott J, Nee J, Harrison W, Blumenthal R: Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol Bull 1993; 29:321–326Medline, Google Scholar
32. Simpson GM, Angus JWS: A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl 1970; 212:11–19Crossref, Medline, Google Scholar
33. Barnes TRE: A rating scale for drug-induced akathisia. Br J Psychiatry 1989; 154:672–676Crossref, Medline, Google Scholar
34. Muller MJ, Himmerich H, Kienzle B, Szegedi A: Differentiating moderate and severe depression using the Montgomery-Åsberg Depression Rating Scale (MADRS). J Affect Disord 2003; 77:255–260Crossref, Medline, Google Scholar
35. Macfadden W, Calabrese JR, McCoy R, Minkwitz M, Wilson E, Mullen J: Antianxiety effects analysis of quetiapine in bipolar depression, in 2004 Annual Meeting New Research Program and Abstracts. Washington, DC, American Psychiatric Association, 2004, number 743Google Scholar
36. Bloom BS: Daily regimen and compliance with treatment (editorial). BMJ 2001; 323:647Crossref, Medline, Google Scholar
37. Kasper S, Brecher M, Fitton L, Jones AM: Maintenance of long-term efficacy and safety of quetiapine in the open-label treatment of schizophrenia. Int Clin Psychopharmacol 2004; 19:281–289Crossref, Medline, Google Scholar
38. Bowden CL, Davis J, Morris D, Swann A, Calabrese J, Lambert M, Goodnick P: Effect size of efficacy measures comparing divalproex, lithium and placebo in acute mania. Depress Anxiety 1997; 6:26–30Crossref, Medline, Google Scholar

