
Suicide Rates Among Physicians: A Quantitative and Gender Assessment (Meta-Analysis)
Abstract
OBJECTIVE: Physicians’ suicide rates have repeatedly been reported to be higher than those of the general population or other academics, but uncertainty remains. In this study, physicians’ suicide rate ratios were estimated with a meta-analysis and systematic quality assessment of recent studies. METHOD: Studies of physicians’ suicide rates were located in MEDLINE, PsycINFO, AARP Ageline, and the EBM Reviews: Cochrane Database of Systematic Reviews with the terms “physicians,” “doctors,” “suicide,” and “mortality.” Studies were included if they were published in or after 1960 and gave estimates of age-standardized suicide rates of physicians and their reference population or reported extractable data on physicians’ suicide; 25 studies met the criteria. Reviewers extracted data and scored each study for quality. The studies were tested for heterogeneity and publication bias and were stratified by publication year, follow-up, and study quality. Effect sizes were pooled by using fixed-effects (women) and random-effects (men) models. RESULTS: The aggregate suicide rate ratio for male physicians, compared to the general population, was 1.41, with a 95% confidence interval (CI) of 1.21–1.65. For female physicians the ratio was 2.27 (95% CI=1.90–2.73). Visual inspection of funnel plots from tests of publication bias revealed randomness for men but some indication of bias for women, with a relative, nonsignificant lack of studies in the lower right quadrant. CONCLUSIONS: Studies on physicians’ suicide collectively show modestly (men) to highly (women) elevated suicide rate ratios. Larger studies should help clarify whether female physicians’ suicide rate is truly elevated or can be explained by publication bias.
Long-standing evidence suggests that those who choose medicine for a career are at greater risk for suicide: the suicide rate among physicians in the United States has been described as nearly twice that seen among white American men (1). In a 2000 national study on causes of death, Frank et al. (2) found a 70% higher rate of mortality due to suicide and self-inflicted injury among white male U.S. physicians than among other professionals. Female physicians’ suicide rate, however, far exceeds that of the general population, in the range of three- to fourfold (2, 3). In a systematic review, Lindeman et al. (4) estimated physicians’ relative suicide risk at 1.1 to 3.4 for men and 2.5 to 5.7 for women when the rates were compared with those for the general population and at 1.5 to 3.8 for men and 3.7 to 4.5 for women when the rates were compared with those for other professionals. However, the authors did not perform any quantitative summary of the results in their systematic review. Instead, they simply summarized the main results of the studies by presenting the range of the relative risks and their 95% confidence intervals (CIs). Furthermore, they did not perform a quantitative evaluation of publication bias and did not estimate the extent to which quality issues explained potential heterogeneity in the suicide rates in their review.
Despite consistent findings, concerns about methodological limitations of previous studies (5, 6) have made suicide studies subject to considerable controversy. We therefore decided to appraise the evidence concerning physician suicide that has been accumulated to date. We report a quantitative analysis of several independent studies, a meta-analysis, which to our knowledge is the first in the literature. We present overall suicide rate ratios for male and female physicians and describe reasons for variations in study results.
Method
Identification of Studies
We searched for studies on the rates of physicians’ mortality and suicide using electronic searches of MEDLINE (from 1966 to July 2003), PsycINFO (from 1984 to July 2003), the AARP Ageline (from 1978 to July 2003), and the EBM (Evidence-Based Medicine) Reviews: Cochrane Database of Systematic Reviews. “Physicians,” “doctors,” “mortality,” and “suicide” were entered as medical subject heading terms and text words and then connected through Boolean operators. We also manually searched reviews and the reference list of each article to locate additional reports published before 1966. We placed no constraints on the language in which the reports were written, the region of the study subjects’ residence, or their age group. We were careful, however, to minimize overlapping time periods and geographic regions among the included studies to avoid duplicate counting of events and the bias this can introduce into a quantitative summary of the evidence.
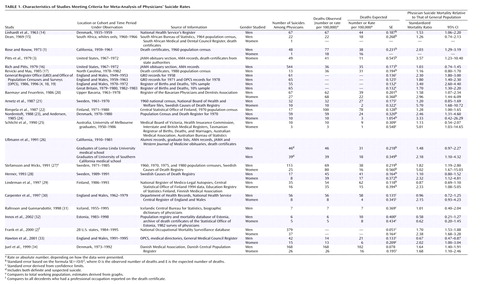
Our search yielded 454 studies, mainly from MEDLINE and PsycINFO. We excluded studies that did not provide any suicide numbers and those that dealt only with attitudes toward suicidal behavior or suicidal risk, suicidal tendency, suicidal thoughts, methods of suicide, physicians’ health in general, prevention of suicide, burnout and stress, experiences of family members after suicide, or therapy of suicidal doctors. We also excluded editorials, case studies, and letters on physician suicide. We included only age-standardized findings in our meta-analysis; thus, studies published before 1960 had to be excluded. Only reports about completed suicides were included; data on attempted suicides were not considered. From the remaining 32 studies we excluded those with overlapping time periods and geographic regions (7), those dealing only with certain medical specialties (8–10), and those without sufficient information from which to calculate suicide rates (11–13). Twenty-five sets of data on physicians’ suicide rates from articles published between 1960 and July 2003 met the inclusion criteria and were entered into our meta-analysis (Table 1).
Data Extraction
The data extraction was done by two reviewers (including E.S.S.) using a standardized form. Where necessary, the standardized mortality ratio (SMR) was calculated on the basis of the numbers of observed (O) and expected (E) deaths reported (SMR=O/E). For one study the standardized mortality ratios had to be approximated from graphs. Standard errors were derived from confidence limits (27). If no confidence limits were provided, we applied the formula SE=√O/E2 to derive the standard error. We used duplicate extraction and checks for errors to ensure accuracy.
Quality Assessment Instrument
Because standard, accepted quality scales for studies on proportions, such as standardized mortality rates, are not available, we developed our own simple quality assessment instrument, to which all 25 articles were subjected. We based the design of this quality assessment instrument on some principal issues in appraising quality, similar to those for controlled trials and interventions. Specifically, we sought to address whether selection bias was minimized, follow-up for final outcomes was adequate, and misclassification bias was minimized. The same two investigators who had extracted the data independently read each article and scored the following items: check of suicides by death registers to avoid misclassification (all, some, or none of the reported suicides were checked), duration of the evaluated time period in years (>10 years, 4–10 years, 2–3 years), age standardization (standardized by using more than one age group, standardized for age >25 years only, no age standardization), and detail of reported inclusion criteria or definition of study group (very detailed, some detail, inaccurate). The quality assessment instrument was used to assign scores in the range of 0 to 2 for each of these four distinct aspects of quality, so that the potential total scores could range from 0 to 8. The simplicity of our quality scoring instrument eliminated any need to train the reviewers. Consistency in quality scores between the two reviewers reached almost 100%. Final consistency was achieved through consensus. Articles published in languages other than English or German were scored with the help of students fluent in these languages (Danish, Swedish, and Finnish). The reviewers separately reported the exact length of follow-up in each study.
Statistical Approach
We performed separate meta-analyses for male and female physicians, using the statistical software STATA (35). We calculated rate ratios for each study and for men and women separately, on the basis of the suicide mortality rate (per 100,000 person-years) among physicians divided by the suicide mortality rate of the general population, during the time period under study. If not provided, 95% CIs were derived under the assumption of an approximate Gaussian distribution of the logarithm of the proportions. We pooled suicide rates by using a random-effects model for male doctors and a fixed-effects model for the female doctors (36).
Because small numbers of trials limit the power of tests for publication bias, we chose to use two different tests to evaluate the possibility of publication bias among the studies. First, we conducted the Begg and Mazumdar adjusted rank correlation test for publication bias (37) and generated a Begg plot. Second, we performed the regression asymmetry test of Egger et al. (38) and generated an Egger plot. Significant test statistics and asymmetry in the plot, especially an empty lower right quadrant (where one would expect to find studies with small effects and high variances), suggest bias. The shape of a funnel plot is largely determined by the arbitrary choice of axes (39). However, the standard error is likely to be the best choice for the vertical axis (40), and we therefore chose the standard error as the measure of study size and the ratio measures for effect sizes.
Results
Studies
We identified 25 studies with suicide rate ratios that met the inclusion criteria. Our meta-analysis is based on 24 rate ratios for male physicians and on 13 suicide rate ratios for female physicians. The characteristics of the studies are presented in Table 1; the assigned quality scores ranged between 4 and 8 for the data on male physicians and between 2 and 8 for the data on female physicians.
Meta-Analysis
We found a moderately and significantly higher risk of suicide among male physicians than among the general population; the overall suicide rate ratio was 1.41 (95% CI=1.21–1.65) (Figure 1). The results of the test for heterogeneity were significant (p<0.001), and we therefore based our analyses on a random-effects model. To further explore heterogeneity, we examined the role of quality score, length of follow-up, and year of publication. There was no significant (p=0.20) interaction between publication year and suicide rate in the meta-regression. The length of follow-up in the individual studies and the study quality were also not significantly (p=0.98 and p=0.72, respectively) related to suicide rate. Publication year (τ2=0.357), length of follow-up (τ2=0.345), and study quality (τ2=0.400) could explain only some of the variation between the studies, with differences in the tau-square values ranging between 3% and 13%. Length of follow-up and study quality combined explained 18% of the variation between the studies. When we limited the meta-analysis to studies with higher quality scores (>5), the suicide rate ratio for male physicians thus remained virtually the same (1.41, 95% CI=1.20–1.66) and heterogeneity among study results persisted. Conversely, studies with low quality scores (1 to 5) showed a slightly attenuated suicide rate ratio (1.28, 95% CI=0.88–1.86). Neither country nor time period of observation added information when we further explored heterogeneity by sorting and eyeballing. The cumulative meta-analysis showed a relatively stable accumulation of evidence for an approximately 40% higher risk of suicide among male physicians throughout the study period.
In the fixed-effects model we found a significantly higher risk of suicide among female physicians than among the general population; the suicide rate ratio was 2.27 (95% CI=1.90–2.73) (Figure 2). Although the studies appeared fairly homogeneous (test for heterogeneity, p=0.14), we hypothesized some amount of variability among the studies. To explore this further we assessed the impact of study quality on the observed suicide rate ratio. When we limited the analysis to high-quality studies (with scores of 6 or 7), the suicide rate ratio for female physicians remained virtually unchanged (2.15, 95% CI=1.68–2.77). The data from the low-quality studies (scores <6) showed a slightly higher suicide rate ratio (2.71, 95% CI=1.52–4.83). Study quality was negatively but not significantly (β=–0.236, p=0.40) associated with the suicide rate ratio. The difference in the tau-square value was 5%, explaining only little of the heterogeneity of the studies on female physicians’ suicide rates. We further stratified the data by length of follow-up and publication year. In the meta-regression, publication year was strongly inversely related (β=–0.148, p<0.01) and length of follow-up was positively related (β=0.041, p=0.36) to the suicide rate of female physicians. Each of the two covariates further explained 5% to 14% of the variance among studies. We observed no apparent difference in risk of suicide due to country or time period of observation. The cumulative meta-analysis showed varying relative risks of suicide among the female physicians, in the range of 5.0 to 2.3, before 1999 and a stable risk of 2.3 after 1999.
Evaluation for Publication Bias
The Egger test for publication bias showed no significant evidence for bias in the data from studies on male physicians’ suicide (intercept estimate=–1.13, p=0.27), and the funnel plot did not reflect asymmetry. The result of the Begg and Mazumdar test (p=0.96) was also not strongly suggestive of publication bias. The funnel plot for the data on female physicians showed some asymmetry, reflecting a relative scarcity of studies with large numbers. Analysis by regressing standardized suicide rates with the inverse of study variance (Egger’s test) revealed some evidence for publication bias (intercept estimate=0.89, p=0.26). The positivity of the intercept indicates that small studies are likely to overestimate the standardized suicide rate.
Discussion
In this meta-analysis, physicians showed modestly higher (men) to much higher (women) suicide rates than the general population.
After assessment of the methodologic aspects of the studies, the results from our meta-analysis confirm previously reported physicians’ suicide rate ratios and suggest that the actual suicide rate ratio of female physicians is substantially higher than that of male physicians.
Evaluation with several methods suggests that publication bias is unlikely to have influenced the results for male physicians. However, there are other methods for testing the presence of publication bias (41), and we cannot completely rule out publication bias, because statistical tests are generally of limited power when small numbers of studies are tested. Furthermore, although the tests we used did not suggest that publication bias influenced the results for female physicians, the visual inspection of the funnel plot revealed asymmetry. The underreporting of suicides in official statistics has been well documented (42). Several suicides will have been recorded as open verdicts or accidents, owing to a coroner’s reluctance to enter suicide as the cause of death because of some, even minimal, doubt. Despite the fact that some studies, in response to this concern, have adopted wider definitions of suicide, such as including accidental poisoning by drugs, we kept the definition narrow in this meta-analysis. However, misclassification in the form of underreporting would bias the suicide rates only toward the null.
The limited number of female physicians is a long-standing source of concern in suicide studies. Despite the recent increase in numbers of female physicians, data on female physicians’ suicides are still few. Because small numbers have often been a major limitation in previous studies, and because even more recent studies have still had to deal with small numbers of suicides by female physicians (2), we used meta-analysis to overcome this limitation. However, tests of publication bias indicated that only small studies of female physicians have been reported to date.
Our study population was fairly homogeneous, reflecting mainly northern European and North American countries. This limits the generalizability of our data with regard to race and sociocultural background. Another possible limitation of our analysis is that we pooled studies of varying quality. We explored study quality by performing analyses on only the trials with low quality scores and on those with high quality scores and did not observe a substantial difference in the risk of suicide among female physicians between the high-quality studies (rate ratio=2.15) and low-quality studies (rate ratio=2.71). However, our score for study quality had a limited range, indicating that study size (which was not captured by the quality score) but not the aspects that were evaluated with this instrument varied between studies.
Few authors have investigated risk factors relating to the working environment, stress factors, or specific personality traits of doctors. There has been some evidence that depression, drug abuse, and alcoholism are often associated with suicides of physicians (43, 44). Simon (44), for instance, reported an incidence of alcoholism and drug addiction of more than 50% among physicians admitted to psychiatric hospitals. Female physicians in particular have been shown to have a higher frequency of alcoholism than women in the general population (45). The literature also suggests that physicians who kill themselves are more critical of others and of themselves and are more likely to blame themselves for their own illnesses (46). Furthermore, there is some, albeit scanty, evidence that physicians feel uncomfortable in turning to colleagues for help (47, 48) and instead resort to alcohol or drugs and isolation. Once they seek help, it appears likely that they are not taken seriously enough by their fellow colleagues: in one study it was found that among suicidal physicians who sought help, more than 50% who later committed suicide had been diagnosed with psychiatric conditions (49) but were not hospitalized before death (20). Finally, while the elevated rates of suicide among physicians, and in particular female physicians, may be much lower than the rates of other groups, such as elderly people or young adults of some ethnic groups, they may well be of special importance: the underlying risk factors for female physicians’ suicides seem to be more obvious (44, 50–54), thus easier to target through prevention programs, than may be the case for other high-risk groups. For example, a higher incidence of psychiatric disorders, particularly more depression (55), has been reported. Furthermore, additional strain imposed on female physicians by their social roles (56), oftentimes leading to excessive drug use (52), has been associated with suicide. However, more research is still needed to further explore these risk factors.
In light of media reports of a nationwide annual suicide toll of 30,000 Americans (57) and the finding that suicide was the 13th leading cause of death worldwide in 2002 (ICD-10), efforts should be undertaken to target early-intervention programs at populations at high risk for suicide. We recommend the recognition of a higher risk of suicide among physicians, particularly female physicians, and the pursuit of further studies to explore potential risk factors and possible avenues of intervention. Such interventions could be modeled after a highly successful U.S. Air Force plan that made the suicide rate in the Air Force drop from 16.4 suicides per 100,000 members to 9.4 by 1998. The program was implemented in 1996 and emphasized early intervention and support services (58). To enhance discrete and confidential access to psychotherapeutic assistance, programs similar to the Canadian assessment and referral service for stressed and impaired physicians (59, 60) can further improve support systems for physicians. Finally, an open discussion of the stress encountered in medical careers is critical in the successful early recognition of impairment and suicide among physicians. Furthermore, given that many studies were conducted more than a generation ago, risk profiles and causal associations may have changed and warrant further investigation.
 |
Received July 30, 2002; revision received Aug. 11, 2003; accepted Feb. 23, 2004. From the Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School; the Department of Epidemiology, Harvard School of Public Health, Boston; the Harvard Center for Cancer Prevention, Boston; the Epidemiology Program, Dana Faber/Harvard Cancer Center, Boston; and the 3rd Medical Department-Oncology, Kaiser Franz Josef-Spital, Vienna. Address reprint requests to Dr. Schernhammer, Channing Laboratory, 181 Longwood Ave., Boston, MA 02115; [email protected] (e-mail). The authors thank Michelle Mazur-Kary for help with data extraction and quality assessment of the studies and the librarians from Countway Library, particularly Suzy Conway, for their help with the literature search.

Figure 1. Meta-Analysis of Male Physicians’ Suicide Rate Ratios in 24 Studiesa
aThe dashed vertical line represents the combined estimate, and the diamond-shaped box represents the confidence interval from the random-effects model. The estimates are plotted with boxes; the area of each box is inversely proportional to the estimated effect’s variance in the study, hence giving more visual prominence to studies where the effect is more precisely estimated.
bLoma Linda University or University of Southern California.

Figure 2. Meta-Analysis of Female Physicians’ Suicide Rate Ratios in 13 Studiesa
aThe dashed vertical line represents the combined estimate, and the diamond-shaped box represents the confidence interval from the fixed-effects model. The estimates are plotted with boxes; the area of each box is inversely proportional to the estimated effect’s variance in the study, hence giving more visual prominence to studies where the effect is more precisely estimated.
1. Rose KD, Rosow I: Physicians who kill themselves. Arch Gen Psychiatry 1973; 29:800–805Crossref, Medline, Google Scholar
2. Frank E, Biola H, Bunrett CA: Mortality rates and causes among US physicians. Am J Prev Med 2000; 19:155–159Crossref, Medline, Google Scholar
3. Pitts FN, Schuller AB, Rich CL: Suicide among US women physicians, 1967–1972. Am J Psychiatry 1979; 136:694–696Link, Google Scholar
4. Lindeman S, Laara E, Hakko H, Lonnqvist J: A systematic review on gender-specific suicide mortality in medical doctors. Br J Psychiatry 1996; 168:274–279Crossref, Medline, Google Scholar
5. von Brauchitsch H: The physician’s suicide revisited. J Nerv Ment Dis 1976; 162:40–45Crossref, Medline, Google Scholar
6. Holmes VF, Rich CL: Suicide among physicians, in Suicide Over the Life-Cycle: Risk Factors, Assessment, and Treatment of Suicidal Patients. Edited by Blumenthal SJ, Kupfer DJ. Washington, DC, American Psychiatric Press, 1990, pp 599–618Google Scholar
7. Steppacher RC, Mausner JS: Suicide in male and female physicians. JAMA 1974; 228:323–328Crossref, Medline, Google Scholar
8. Lew EA: Mortality experience among anesthesiologists, 1954–1976. Anesthesiology 1979; 51:195–199Crossref, Medline, Google Scholar
9. Linde HW, Mesnick PS, Smith NJ: Causes of death among anesthesiologists: 1930–1946. Anesth Analg 1981; 60:1–7Crossref, Medline, Google Scholar
10. Rich CL, Pitts FN: Suicide by psychiatrists: a study of medical specialists among 18,730 consecutive physician deaths during a five-year period, 1967–1972. J Clin Psychiatry 1980; 41:261–263Medline, Google Scholar
11. Asp S, Hernberg S, Collan Y: Mortality among Finnish doctors, 1953–1972. Scand J Soc Med 1979; 75:55–62Google Scholar
12. Crawshaw R, Bruce JA, Eraker PL, Greenbaum M, Lindemann JE, Schmidt DE: An epidemic of suicide among physicians on probation. JAMA 1980; 243:1915–1917Crossref, Medline, Google Scholar
13. Physician mortality and suicide. Conn Med 1986; 50:37–43Medline, Google Scholar
14. Linhardt M, Frandsen E, Hamtoft H: Causes of death among the medical profession in Denmark. Dan Med Bull 1963; 10:59–64Google Scholar
15. Dean G: The causes of death of South African doctors and dentists. S Afr Med J 1969; 43:495–500Medline, Google Scholar
16. Rich CL, Pitts FN: Suicide by male physicians during a five-year period. Am J Psychiatry 1979; 136:1089–1090Link, Google Scholar
17. Revicki DA, May HJ: Physician suicide in North Carolina. South Med J 1985; 78:1205–1207Crossref, Medline, Google Scholar
18. Office of Population Censuses and Surveys: Occupational Mortality 1979–80, 1982–83, Decennial Supplement, Part I: Commentary: Series DS, Number 6. London, Her Majesty’s Stationery Office, 1986Google Scholar
19. Office of Population Censuses and Surveys: Occupational Mortality 1979–80, 1982–83, Decennial Supplement, Part II: Microfiche Tables: Series DS, Number 6. London, Her Majesty’s Stationery Office, 1986Google Scholar
20. Baemayr A, Feuerlein W: Suizidhaeufigkeit bei Aerzten und Zahnaerzten in Oberbayern. Soc Psychiatry 1986; 21:39–48Crossref, Medline, Google Scholar
21. Arnetz BB, Horte LG, Hedberg A, Theorell T, Allander E, Malker H: Suicide patterns among physicians related to other academics as well as to the general population. Acta Psychiatr Scand 1987; 75:139–143Crossref, Medline, Google Scholar
22. Rimpela AH, Nurminen MM, Pulkkinen PO, Rimpela MK, Valkonen T: Mortality of doctors: do doctors benefit from their medical knowledge? Lancet 1987; 1:84–86Crossref, Medline, Google Scholar
23. Nordentoft M: [Suicide among physicians.] Ugeskr Laeger 1988; 150:2440–2443 (Danish)Medline, Google Scholar
24. Andersen O: Dodelighed og erhverv 1970–1980. Copenhagen, Statistics Denmark, 1985Google Scholar
25. Schlicht SM, Gordon IR, Ball RB, Christie DGS: Suicide and related deaths in Victorian doctors. Med J Aust 1990; 153:518–521Crossref, Medline, Google Scholar
26. Ullmann D, Phillips RL, Beeson WL, Dewey HG, Brin BN, Kuzma JW, Mathews CP, Hirst AE: Cause-specific mortality among physicians with differing life-styles. JAMA 1991; 265:2352–2359Crossref, Medline, Google Scholar
27. Stefansson CG, Wicks S: Health care occupations and suicide in Sweden 1961–1985. Soc Psychiatry Psychiatr Epidemiol 1991; 26:259–264Crossref, Medline, Google Scholar
28. Herner B: High frequency of suicide among younger physicians: unsatisfactory working situations should be dealt with. Lakartidningen 1993; 90:3449–3452Medline, Google Scholar
29. Lindeman S, Laara E, Hirvonen J, Lonnqvist J: Suicide mortality among medical doctors in Finland: are females more prone to suicide than their male colleagues? Psychol Med 1997; 27:1219–1222Crossref, Medline, Google Scholar
30. Carpenter LM, Swerdlow AJ, Fear NT: Mortality of doctors in different specialities: findings from a cohort of 20,000 NHS hospital consultants. Occup Environ Med 1997; 54:388–395Crossref, Medline, Google Scholar
31. Rafnsson V, Gunnarsdottir HK: Causes of death and incidence of cancer in physicians and lawyers in Iceland. Nord Med 1998; 113:202–207Medline, Google Scholar
32. Innos K, Rahu K, Baburin A, Rahu M: Cancer incidence and cause-specific mortality in male and female physicians: a cohort study in Estonia. Scand J Public Health 2002; 30:133–140Crossref, Medline, Google Scholar
33. Hawton K, Clements A, Sakarovitch C, Simkin S, Deeks JJ: Suicide in doctors: a study of risk according to gender, seniority and specialty in medical practitioners in England and Wales, 1979–1995. J Epidemiol Community Health 2001; 55:296–300Crossref, Medline, Google Scholar
34. Juel K, Mosbech J, Stottrup-Hansen ES: Mortality and causes of death among Danish medical doctors 1973–1992. Int J Epidemiol 1999; 28:456–460Crossref, Medline, Google Scholar
35. STATA commands for meta-analyses, in STATA, vol 2001. College Station, Tex, Stata, 2001. www.stata.comGoogle Scholar
36. DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials 1986; 7:177–188Crossref, Medline, Google Scholar
37. Begg CB, Mazumdar M: Operating characteristics of a rank correlation test for publication bias. Biometrics 1994; 50:1088–1101Crossref, Medline, Google Scholar
38. Egger M, Smith GD, Schneider M, Minder C: Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315:629–634Crossref, Medline, Google Scholar
39. Tang J-L, Liu JLY: Misleading funnel plot for detection of bias in meta-analysis. J Clin Epidemiol 2000; 53:477–484Crossref, Medline, Google Scholar
40. Sterne JAC, Egger M: Funnel plots for detecting bias in meta-analysis: guidelines on choices of axis. J Clin Epidemiol 2001; 54:1046–1055Crossref, Medline, Google Scholar
41. Duval S, Tweedie R: Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000; 56:455–463Crossref, Medline, Google Scholar
42. Sainsbury P, Jenkins JS: The accuracy of officially reported suicide statistics for purposes of epidemiological research. J Epidemiol Community Health 1982; 36:43–48Crossref, Medline, Google Scholar
43. Roy A: Suicide in doctors. Psychiatr Clin North Am 1985; 8:377–387Crossref, Medline, Google Scholar
44. Simon W: Suicide among physicians: prevention and postvention. Crisis 1986; 7:1–13Medline, Google Scholar
45. Bonk K: Selbstmord und Alkohol unter besonderer Beruecksichtigung der alkoholischen Beeinflussung bei Tatzeit. Cologne, Germany, University of Cologne Medical School, 1973Google Scholar
46. Results and implications of the AMA-APA Physician Mortality Project. JAMA 1987; 257:2949–2953Crossref, Medline, Google Scholar
47. Vaillant GE, Sobowale NC, McArthur C: Some psychologic vulnerabilities of physicians. N Engl J Med 1972; 287:372–375Crossref, Medline, Google Scholar
48. Kligfeld M, Hoffman DL: Medical student attitude toward seeking professional psychological help. J Med Educ 1979; 54:617–621Medline, Google Scholar
49. Feuerlein W: Suicide and attempted suicide: trends, statistics, prevention, help. Med Klin 1973; 68:1717–1721Medline, Google Scholar
50. A’Brook MF, Hailstone JD, McLaughlan IE: Psychiatric illness in the medical profession. Br J Psychiatry 1967; 113:1013–1023Crossref, Medline, Google Scholar
51. Arana GW: The impaired physician: a medical and social dilemma. Gen Hosp Psychiatry 1982; 4:147–154Crossref, Medline, Google Scholar
52. Bressler B: Suicide and drug abuse in the medical community. Suicide Life Threat Behav 1976; 6:169–178Medline, Google Scholar
53. Chambers R, Maxwell R: Helping sick doctors: fix the job, not the doctors. Br Med J 1996; 312:722–723Crossref, Medline, Google Scholar
54. Johnson WD: Predisposition to emotional distress and psychiatric illness amongst doctors: the role of unconscious and experiential factors. Br J Med Psychol 1991; 64:317–329Crossref, Medline, Google Scholar
55. Welner A, Marten S, Wochnik E: Psychiatric disorders among professional women. Arch Gen Psychiatry 1979; 36:169–173Crossref, Medline, Google Scholar
56. Notman MT, Nadelson CC: Medicine: a career conflict for women. Am J Psychiatry 1973; 130:1123–1127Link, Google Scholar
57. Leonard M: US launches campaign to fight suicide. Boston Globe, May 3, 2001, p A5Google Scholar
58. Suicide prevention among active duty Air Force personnel—United States, 1990–1999. MMWR Morb Mortal Wkly Rep 1999; 48:1053–1057Medline, Google Scholar
59. Fish JS, Steinert Y: Helping physicians in distress: developing a physician assessment and referral service. Can Fam Physician 1995; 41:249–255Medline, Google Scholar
60. Johnston C: Suicide totals for MDs sad reminder of stresses facing medicine, conference told. Can Med Assoc J 1996; 155:109–111Google Scholar

