
Attachment and Traumatic Stress in Female Holocaust Child Survivors and Their Daughters
Abstract
OBJECTIVE: During the Holocaust, extreme trauma was inflicted on children who experienced it. Two questions were central to the current investigation. First, do survivors of the Holocaust still show marks of their traumatic experiences, even after more than 50 years? Second, was the trauma passed on to the next generation? METHOD: Careful matching of Holocaust survivors and comparison subjects was employed to form a research study design with three generations, including 98 families with a grandmother, a mother, and an infant, who engaged in attachment- and trauma-related interviews, questionnaires, and observational procedures. RESULTS: Holocaust survivors (now grandmothers) showed more signs of traumatic stress and more often lack of resolution of trauma than comparison subjects, but they were not impaired in general adaptation. Also, the traumatic effects did not appear to transmit across generations. CONCLUSIONS: Holocaust survivors may have been able to protect their daughters from their war experiences, although they themselves still suffer from the effects of the Holocaust.
During the Holocaust, extreme trauma was inflicted on children who experienced it, raising two questions that are central to the current report. First, do Holocaust survivors still show marks of their traumatic experiences, even after more than 50 years? Second, was the trauma passed on to the daughters in the next generation (1)? The existence of long-term psychological effects of the Holocaust on survivors and their offspring still divide the scientific literature (1).
Generally, most large-scale and well-designed epidemiological studies do not show serious psychological problems in Holocaust survivors or their families (1). Such conclusions run contrary to other claims, stemming mostly from clinical observations, that the Holocaust had a profound effect on its victims, leaving many survivors with various psychological or marital problems (2–4). This is consistent with existing non-Holocaust-related trauma research, which provides evidence that people who undergo extreme stress are left more vulnerable to future adversity (5–7). Similarly, posttraumatic long-term effects were reported in a more recent nonclinical Holocaust-related study (8) showing that elderly survivors of the Holocaust suffered from the Persian Gulf War to a larger extent than other subjects. Also, clinically based reports on children of Holocaust survivors versus more controlled research paradigms are inconsistent in their findings. Whereas clinically based reports point to intergenerational transmission of traumatic experiences, more controlled studies have not found much psychopathology (1), except when second-generation subjects were confronted with life-threatening situations (9, 10).
We propose that the conceptual framework of attachment theory may shed new light on this controversy. From an evolutionary perspective, attachment is conceived as a universal bias in infants to remain in the proximity of a protective caregiver. The main focus of attachment theory is on the making and breaking of relationships, and it focuses on the determinants and effects of affective bonds between children and their caregivers and on the separation or loss of attachment figures (11). In attachment theory, unresolved mourning/trauma is indicated by disoriented thought processes about attachment experiences owing to lack of resolution of mourning in case of loss of a close attachment figure or lack of resolution of other traumatic experiences (12, 13). Many Holocaust survivors may well suffer from prolonged unresolved mourning/trauma (12). Lack of resolution of mourning might have led the child later as a parent to exhibit frightened, helpless, and unexpected behavior, hence enhancing the likelihood of a disorganized attachment relationship to develop in her own child (12).
In order to bridge the gap between clinical and nonclinical approaches, we compared two carefully matched groups (14): Israeli grandmothers with and without Holocaust experience during their own childhood, all of whom were residing in Israel during the past 50–60 years or so. We also included the daughters of the grandmothers in the two groups (now mothers themselves). Our first hypothesis was that anxiety and traumatic stress as well as insecure and unresolved mental representations of attachment were overrepresented in families with a Holocaust background. The second hypothesis was that possible traumatization in the grandmothers may have been transmitted to the next generation. The third hypothesis was that a higher frequency of disorganizing (e.g., frightened [12]) maternal behavior could be observed in the mothers whose own mothers (grandmothers) were Holocaust survivors than in the mothers without such a background. Finally, because both attachment and Holocaust researchers have documented human resiliency even under the most unfavorable life circumstances (15), our fourth hypothesis was that Holocaust survivors may be functioning well in several social domains, despite their traumatic experiences.
Method
Recruitment of the Sample
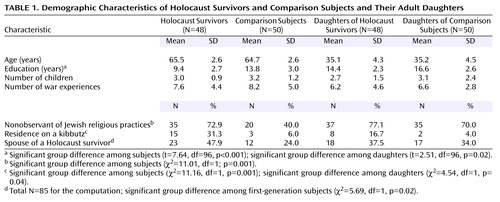
In order to avoid recruitment of participants through convenience groups (e.g., mental health clinics, Holocaust-related organizations, and advertisements), we used basic population-wide demographic information provided by the Israeli Ministry of the Interior. Israeli regulations concerning privacy allowed us to receive lists of names that included only the date of birth and year of immigration from Europe to Israel. We conducted approximately 30,000 standardized telephone calls to recruit two groups—Holocaust and matched comparison subjects—according to the following criteria (Table 1). Subjects in the Holocaust group (child survivors) were born in Europe between 1926 and 1937; thus, they were 4–14 years old during World War II. Having lost both their mothers and fathers and some even other family members, they immigrated as orphans to Israel during or soon after the war (1945). Later in life, they married Israeli spouses who were or were not Holocaust survivors. Their children (the second generation, now mothers) were all born in Israel between 1947 and 1970 and had at least one healthy child between the ages of 12 and 15 months (the third generation).
Subjects in the comparison group were in the same age range as that of the Holocaust group, were also born in Europe, did not experience the Holocaust, immigrated to Israel as children before the war, but did not lose any close family members because of the Holocaust. Their Israeli-born daughters (now mothers) also had at least one healthy infant between the ages of 12 and 15 months. The final sample consisted of 48 and 50 participants in the Holocaust and comparison groups, respectively. A power analysis showed that this sample size was sufficiently powerful to allow conclusions about the absence of differences between the two groups. With a moderate effect size (d=0.50), the power to predict conclusions was 0.80 (16).
Despite this unprecedented screening procedure, groups unavoidably differed on several Holocaust-related variables such as education (Holocaust survivors obviously received less education during the Holocaust years), residence (Holocaust survivors were more often welcomed into kibbutzim), religion (survivors were more often secular), and background of the partner (Holocaust survivors more often married partners with Holocaust experiences). In terms of age, number of children, and war-related experiences in Israel after World War II, the groups did not significantly differ. Despite the importance of the father’s role in child development, research on intergenerational transmission of attachment is more frequent with mothers. Thus, for both methodological and logistic reasons, the first generation as well as the second generation consisted of female participants only. Upon description of the study to the subjects, written informed consent was obtained.
Procedure
We interviewed and collected self-report data pertaining to the adults involved in two sessions for each generation (i.e., the Holocaust survivors, the comparison subjects, and the daughters of the two groups) about 2–3 months before we conducted direct laboratory observations of mother-infant interactions when the infants were 12–15 months old.
Measures
Unless otherwise stated, all interviews, questionnaires, and inventories were administered to both daughters (the second generation) and to their elder mothers (the first generation). The Marlowe-Crowne Social Desirability Scale (17) was used to ensure that both groups did not differ in their tendency for social desirability. Moreover, a checklist of war-related events in Israel since its founding in 1948 was administered to all participants. Because of space limitations, only major aspects of the measures are described here. Further details can be obtained upon request from the first author.
The Adult Attachment Interview (12, 13) assesses current mental representations of childhood attachment experiences, including loss and trauma experiences. The five attachment classifications were coded as follows: 1) secure: autonomous, coherent in exploring past experiences, whether positive or negative; 2) insecure: dismissive of past relationships with attachment figures and attachment experiences; 3) insecure: preoccupied with past experiences and angry toward attachment figures; 4) insecure: disoriented with regard to attachment because of lack of resolution of loss/trauma; 5) insecure: cannot classify (a mixture of diverging mental representations of attachment so that no single representation seems to dominate the participant’s thinking about the past) (12). In previous studies, the psychometric characteristics of the Adult Attachment Interview have proven to be excellent (13). The Adult Attachment Interviews were coded by two authors (T.J. and N.K.-K.), both of whom were certified to code the interview. Interjudgment reliability for the present study was 85%, with kappa=0.76 (p<0.001).
Anxiety and traumatic-related stress measures
The Endler Multidimensional Anxiety Scales (18) consist of two reliable and valid subscales: the cognitive worry scale and the autonomic anxiety scale. Cronbach’s alpha reliabilities for the cognitive worry scale were 0.85 and 0.84, and 0.84 and 0.83 for the autonomic anxiety scale (for first- and second-generation subjects, respectively).
The Impact of Event Scale (19, 20) is a posttraumatic stress measure that purports to assess the intensity of intrusion and avoidance responses that follow exposure to extreme stress. It has been found to be reliable and valid with different stressors and populations (19, 20). Horowitz et al. (20) suggested that the Impact of Event Scale can be tailored to any specific stressor, and in this study, it was adapted to Holocaust experiences. Cronbach’s alpha reliability coefficients for intrusion and avoidance were 0.84 and 0.78, respectively, for the first generation and 0.88 and 0.80 for the second generation.
The Berkeley-Leiden Adult Attachment Questionnaire for Unresolved Loss or Trauma (21) consists of 58 Likert-type items that constitute two major scales: unresolved states of mind (e.g., feelings of responsibility for a death) and unusual beliefs (e.g., mental telepathy). Two items (items 47 and 55) were deleted because they were not applicable to the current sample. In a previous study of Holocaust survivors, the Berkeley-Leiden Adult Attachment Questionnaire for Unresolved Loss or Trauma proved to be a valid measure (21). In the current study, alpha reliabilities were 0.90 and 0.86 for unresolved states of mind and unusual beliefs scales, respectively. Owing to the skewness of the distribution of the scores, all items were inverted (1/raw score) before the items were summed; therefore, higher scores represent higher levels of unusual beliefs and unresolved states of mind.
In order to create an overall score for signs of anxiety and posttraumatic stress for the subjects, we conducted a principal-components analysis of the six scales, which loaded on the first component (eigenvalues >0.45) and explained 43% of the variance. Alpha reliability of the total scale was 0.72. We replicated these analyses for the second generation—the daughters.
Personal, interpersonal, and social adaptation measures
An adapted version of the Mental Health Inventory (22) was completed to assess sense of well-being. The participants were asked to indicate on a 6-point Likert scale the extent to which different feelings of well-being (14 items) had been associated with their lives during the past month. Cronbach’s alpha reliability coefficients were 0.90 for the first generation and 0.91 for the second generation—the daughters.
The Social Adaptation Checklist was designed to obtain a global picture of the participants’ integration into the community, including affiliations with organizations and community activities, leisure activities, occupational and residential stability, and finally, history of illnesses and accidents.
The Marital Autonomy and Relatedness Inventory (23) assesses the perception of autonomy and relatedness in marriage. In the present study, we used 20 items pertaining to the love and warmth dimension, with Cronbach’s alpha reliability coefficients of 0.92 and 0.90 for the first- and second-generation subjects, respectively.
The daughters reported the satisfaction with their relationship with their mothers in the Caregiving Scale (available by request from the first author), which was especially designed for this study. The daughters were asked to indicate the extent to which they had to deal with the various challenges that may come from their own mothers now that they are aging. A summary score of successful caregiving was based on 19 items, with a Cronbach’s alpha reliability coefficient of 0.94.
Mother-infant interactions were observed with distressing toys and frightening robot situations, with a specific focus on identifying disorganizing maternal behaviors. The Maternal Inappropriate and Disorganizing Behavior Scale is based on earlier coding systems for insensitive and frightening maternal behaviors (24). In each observational situation, high reliability was established for 30 mothers (kappa=0.96).
Statistical Analyses
Data analyses consisted of four major segments: 1) a series of chi-square and hierarchical log linear analyses examining categorical attachment data, 2) a multivariate analysis of variance (MANOVA) and related post hoc analyses of variance (ANOVAs) examining the differences between Holocaust and comparison groups with regard to anxiety and traumatic stress measures, 3) a series of t tests contrasting Holocaust and comparison groups on personal, interpersonal, and social adaptation measures, and 4) ANOVAs examining differences in maternal disorganizing behaviors between the two groups.
Results
Attachment Data
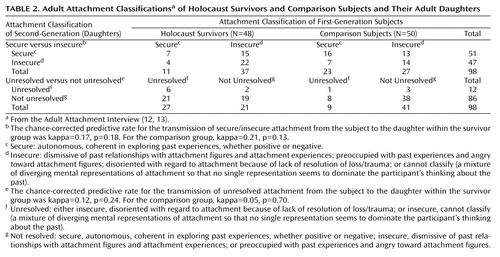
In Table 2, the Adult Attachment Interview classifications of first-generation subjects and their daughters in the Holocaust and comparison groups are presented in two ways: 1) secure versus insecure mental representations of past attachment experiences and 2) unresolved versus not unresolved representations indicating whether or not participants suffered from lack of resolution of past losses and trauma experiences. The attachment classifications were not associated with age, education, number of children, or any other background variables displayed in Table 1. Only residence on a kibbutz was related to the occurrence of unresolved loss or trauma in the first-generation subjects (χ2=9.45, df=1, p<0.02).
To test the effect of the Holocaust on the security of the attachment representation and its transmission from survivors to their children, a two-by-two-by-two hierarchical log linear analysis was performed to test the following model: security of attachment (secure versus insecure) by generation (first generation versus second generation) by group (Holocaust versus comparison). The analysis showed a best-fitting model consisting of the interaction of security by generation and the interaction of security of first generation by group (likelihood ratio: χ2=0.49, df=2, p=0.79). Holocaust survivors had significantly fewer secure attachment representations (N=11, 22.9%) than the comparison subjects (N=23, 46.0%), primarily owing to the large number of unresolved classifications in the Holocaust group. Furthermore, the interaction of security and generation meant that there was a significant transmission of attachment security from the first-generation subjects to their daughters, but this transmission was not specific to the Holocaust group. In fact, in 60.2% of the cases (N=59), the first-generation subjects and their daughters showed the same attachment representation (kappa=0.21, p=0.02), which is consistent with several nonclinical samples documenting intergenerational transmission of attachment (13).
To test the effect of the Holocaust on unresolved loss or trauma and its transmission from survivors to their daughters, we performed a two-by-two-by-two hierarchical log linear analysis of unresolved loss/trauma (unresolved versus not unresolved) by generation (first generation versus daughters) by group (Holocaust versus comparison). The best-fitting model consisted of the interaction between first-generation subjects with unresolved loss and trauma and group and a main effect for daughters with unresolved loss and trauma (likelihood ratio: χ2=3.31, df=3, p=0.35). In the Holocaust survivor group, there were significantly more subjects suffering from unresolved loss and trauma (N=27, 56.3%) than in the comparison group (N=9, 18.0%), whereas the daughters with unresolved loss and trauma were in the minority in the second generation (overall N=11, 11.2%). Differences between the daughters of Holocaust survivors and comparison subjects were absent, as was the transmission of unresolved loss or trauma from the survivors to their (adult) daughters (kappa=0.13, p=0.10). This outcome was replicated in a subset of nonkibbutz participants (likelihood ratio: χ2=3.40, df=3, p=0.33).
Anxiety and Traumatic Stress Measures
The anxiety and traumatic stress measures also confirmed the impact of the Holocaust on the generation of survivors, and at the same time, they corroborated the lack of any influence on the second generation. For the purpose of multivariate analyses, the measures were transformed into z scores. A MANOVA with the Endler Multidimensional Anxiety Scales, the Impact of Event Scale, and the Berkeley-Leiden Adult Attachment Questionnaire for Unresolved Loss or Trauma scales as dependent variables and group (Holocaust survivors versus comparison subjects) as a factor showed a significant multivariate effect (F=5.54, df=6, 91, p<0.001). Post hoc ANOVAs showed that significant associations were found for the autonomic-anxiety scale of the Endler Multidimensional Anxiety Scales (F=8.81, df=1, 96, p<0.004), the avoidance scale of the Impact of Event Scale (F=21.59, df=1, 96, p<0.001), and the unresolved loss scale of the Berkeley-Leiden Adult Attachment Questionnaire for Unresolved Loss or Trauma (F=6.09, df=1, 96, p<0.02). Holocaust survivors showed more anxiety and more traumatic stress reactions on the avoidance and unresolved measures (Figure 1 shows mean z scores). For the second generation, no significant differences on the anxiety and traumatic stress measures were found between the daughters of the Holocaust survivors and the daughters of the comparison subjects.
In order to protect against a chance finding, we used an overall measure for signs of posttraumatic stress in an ANOVA and found a significant group difference for the first-generation subjects (F=14.19, df=1, 96, p<0.001). Means and standard deviations for the Holocaust and first-generation comparison groups were mean=1.39 (SD=4.00) and mean=–1.33 (SD=3.12), respectively. Levene’s test for homogeneity of variances was not significant (F=2.04, df=1, 96, p=0.16). After computing the effect size for this comparison, we found a large Cohen’s d (0.77) (16). The same analysis for the daughters did not yield a significant difference (F=0.83, df=1, 96, p=0.36). Means and standard deviations for the Holocaust and comparison groups of daughters were mean=0.25 (SD=3.04) and mean=–0.38 (SD=3.82), respectively. Levene’s test for homogeneity of variances was not significant (F=2.48, df=1, 96, p=0.12).
We also compared the groups on the social desirability measure (17), for which no differences were found (F<1.00, df=1, 96, p=0.39, and F<1.00, df=1, 96, p=0.73) for the first-generation subjects and their daughters, respectively, suggesting that the differences between the subjects’ responses to the anxiety and traumatic stress measures could not be ascribed to differences in the tendency to provide socially desirable answers to the self-report measures.
Personal, Interpersonal, and Social Adaptation Measures
We also did not find differences on the various personal, interpersonal, and social adaptation measures that were not directly related to the traumatic experiences of the Holocaust. Protecting the t test against chance findings, we used the Bonferroni adjustment for the alpha level (alpha <0.008). Holocaust subjects and their daughters did not differ from their matched comparison subjects on the index for love and warmth in the marital relationship (Marital Autonomy and Relatedness Inventory), on the Caregiving Scale, as completed by the daughters about their relationship with their mothers, on the Mental Health Inventory for general well-being, on the amount of accumulated illnesses and accidents over time, on the various indices of integration into the community, and on occupational stability.
Maternal Disorganizing Behaviors
Finally, the daughters of the Holocaust survivors did not differ from their comparison subjects on both the distressing toys and frightening robot situations that were used to assess their inappropriate maternal and disorganizing behaviors (Maternal Inappropriate and Disorganizing Behavior Scale) with their infants (F<1.00, df=1, 80, p=0.48, and F<1.00, df=1, 79, p=0.79, respectively).
Discussion
The results support the hypothesis that the Holocaust affected the lives of child survivors, even after more than 50 years. The survivors showed more unresolved loss on the Adult Attachment Interview, and they displayed more anxiety and traumatic stress than the carefully matched comparison subjects, who did not experience the Holocaust. The difference amounted to a strong effect, according to conventional criteria (16). The daughters of Holocaust survivors, however, did not differ from the comparison group in their attachment representations, anxiety, traumatic stress reactions, and maternal behavior toward their infants. We suggest that the child survivors successfully protected their social lives and family relationships from being influenced by their Holocaust experiences. They reported a similar degree of general well-being and integration into the community as their comparison subjects, and they did not differ in the love and warmth they found in their marital relationships. They also related in similar ways to their daughters as the comparison subjects did.
However, some limitations should be mentioned. First, the entire sample consisted of 98 triads of participants that were equally divided among Holocaust and comparison groups. The unique and stringent matching procedure did not allow for a larger number of participants. It should be noted, however, that power analysis of the design suggested that this sample size was sufficiently powerful to accept the absence of differences between the groups as valid. Second, although state-of-the-art attachment and traumatic stress measures were used, physiological assessments, such as the use of cortisol for indexing stress levels, might have further enriched the findings (25). Traditional DSM-IV-based diagnostic assessment of posttraumatic stress disorder might have refined our results as well. At the same time, we decided to rely on self-reported and attachment-based indicators of posttraumatic stress because of the nonclinical nature of the Holocaust and the comparison group.
We speculate that Holocaust survivors are in a better position to avoid transmitting their traumatic experiences than child abuse victims for two reasons. First, the traumatic events were not created by their parents or other attachment figures but emerged from an almost anonymous destructive force (the Nazis). The Holocaust did not implicate a breakdown of trust in their attachment figures but consisted of an inhuman social-political force. Second, the child survivors in our study had experienced several years of normal family life before the Holocaust threw their lives into jeopardy. During these early years, basic trust in attachment figures may have developed, empowering the child survivors after the war to cope with the challenges of adapting to normal family and social life again and become attachment figures themselves.
Moreover, some of the subjects may have been experiencing continuing bonds with their deceased parents (26, 27). In a recent literature review on loss and bereavement (28), the continuing-bond concept was proposed to be a potentially important extension of Bowlby’s views on grief and mourning (11). Perhaps some of the subjects who were classified in the Adult Attachment Interview as not having resolved their loss or trauma experiences demonstrated a continuing bond with their deceased parents. One is reminded that the loss they experienced was under the least natural circumstances. In fact, it may be impossible for any person ever to resolve a trauma like that of the Holocaust, in particular when it involves the extermination of parents and other close relatives under such dark and atrocious circumstances.
Finally, Frankl’s idea of man’s search for meaning in avoiding fixating on the past by orienting toward future goals as a healing power in traumatized subjects (29) may be especially pertinent to Holocaust survivors in Israel who helped build a new nation after World War II. Furthermore, for Israeli Holocaust survivors, being part of a large community with a collective memory of the Holocaust may have served as a potentially protective factor (30, 31). Whatever interpretation will stand to empirical scrutiny, our investigation shows how resilient victims of major genocides might be in creating new hope for the coming generations.
 |
 |
Presented in part at the Eighth Congress of the World Association for Infant Mental Health, Amsterdam, July 16–20, 2002. Received Nov. 27, 2001; revisions received Aug. 9 and Nov. 22, 2002; accepted Nov. 26, 2002. From the Center for the Study of Child Development, University of Haifa, Israel; the Center for Child and Family Studies, Leiden University, Leiden, the Netherlands; and the Institute of Psychology, Regensburg University, Regensburg, Germany. Address reprint requests to Dr. Sagi-Schwartz, Center for the Study of Child Development, 6035 Rabin Building, University of Haifa, Haifa 31905, Israel; [email protected] (e-mail). The first three authors are the principal investigators of the study. The contributions of the first two authors to the present study were equal. Funded by the German-Israel Foundation for Research and Development (GIF 279) and the Koehler Stiftung. The authors thank Anouschka Büttner and Anika Keppler for coding the Maternal Inappropriate and Disorganizing Behavior Scale, the interviewers (Noa Egoz-Mizrachi, Ayelet Etzion-Carasso, Yael Goshen, Sarit Guttmann, and Ran Navon), and Motti Gini, Erik Hesse, Mary Main, Miriam Steele, and Howard Steele for their contributions, advice, and discussions.

Figure 1. Measures of Traumatic Stress for Holocaust Survivors and Comparison Subjectsa
aAll variables were standardized, and the mean score for every variable was 0. All scores for the Holocaust group were above the mean, and all scores for the comparison group were below the mean.
1. Bar-On D, Eland J, Kleber RJ, Krell R, Moore Y, Sagi A, Soriano E, Suedfeld P, Van der Velden PG, Van IJzendoorn MH: Multigenerational perspectives of coping with the Holocaust experience: on the developmental sequelae of trauma across generations. Int J Behav Dev 1998; 22:315-338Crossref, Google Scholar
2. Niederland WG: Clinical observations on the “survivor syndrome”: symposium on psychic traumatization through social catastrophe. Int J Psychoanal 1968; 49:313-315Medline, Google Scholar
3. Dor-Shav NK: On the long-range effects of concentration camp internment of Nazi victims. J Consult Clin Psychol 1978; 46:1-11Crossref, Medline, Google Scholar
4. Danieli Y: Families of survivors of the Nazi Holocaust: some short- and long-term effects, in Stress and Anxiety, vol 8. Edited by Spielberger CD, Sarason IG, Milgram N. New York, McGraw-Hill/Hemisphere, 1982, pp 405-421Google Scholar
5. Silver RL, Wortman CB: Coping with undesirable events, in Human Helplessness: Theory and Application. Edited by Garber J, Seligman ME. New York, Academic Press, 1980, pp 279-340Google Scholar
6. Frye JS, Stockton RA: Discrimination analysis of posttraumatic stress disorder among a group of Vietnam veterans. Am J Psychiatry 1982; 139:52-56Link, Google Scholar
7. Goldstein G, van Kammen W, Shelly C, Miller DJ, van Kammen D: Survivors of imprisonment in the Pacific Theater during World War II. Am J Psychiatry 1987; 144:1210-1213Link, Google Scholar
8. Solomon Z, Prager E: Elderly Israeli Holocaust survivors during the Persian Gulf War: a study of psychological distress. Am J Psychiatry 1992; 149:1707-1710Link, Google Scholar
9. Solomon Z, Kotler M, Mikulincer M: Combat-related posttraumatic stress disorder among second-generation Holocaust survivors: preliminary findings. Am J Psychiatry 1988; 145:865-868Link, Google Scholar
10. Baider L, Peretz T, Hadani PE, Perry S, Avramov R, Kaplan De-Nour A: Transmission of response to trauma? second-generation Holocaust survivors’ reaction to cancer. Am J Psychiatry 2000; 157:904-910Link, Google Scholar
11. Bowlby J: Attachment and Loss, Vol I: Attachment, 2nd ed. London, Pelican, 1984Google Scholar
12. Hesse E: The Adult Attachment Interview: historical and current perspectives, in Handbook of Attachment: Theory, Research, and Clinical Applications. Edited by Cassidy J, Shaver PR. New York, Guilford, 1999, pp 395-433Google Scholar
13. Van IJzendoorn MH: Associations between adult attachment representations and parent-child attachment, parental responsiveness, and clinical status: a meta-analysis on the predictive validity of the Adult Attachment Interview. Psychol Bull 1995; 117:387-403Crossref, Medline, Google Scholar
14. Cook TD, Campbell DT: Quasi-Experimentation: Design and Analysis Issues for Field Settings. Chicago, Rand McNally, 1979Google Scholar
15. Rutter M, Sroufe LA: Developmental psychopathology: concepts and challenges. Dev Psychopathol 2000; 12:265-296Crossref, Medline, Google Scholar
16. Cohen J: Statistical Power Analysis for the Behavioral Sciences, 2nd ed. New York, Academic Press, 1977Google Scholar
17. Crowne D, Marlowe P: The Approval Motive: Studies in Valuative Dependence. New York, John Wiley & Sons, 1964Google Scholar
18. Endler NS, Lobel TE, Parker JDA, Schmitz P: Multidimensionality of state and trait anxiety: a cross-cultural study comparing American, Canadian, Israeli and German young adults. Anxiety Res: An Int J 1991; 3:252-272Google Scholar
19. Schwarzwald J, Solomon Z, Weisenberg M, Mikulincer M: Validation of the Impact of Event Scale for psychological sequelae of combat. J Consult Clin Psychol 1978; 55:251-256Crossref, Google Scholar
20. Horowitz MJ, Wilner N, Alvarez W: Impact of Event Scale: a measure of subjective stress. Psychosom Med 1979; 41:209-218Crossref, Medline, Google Scholar
21. Sagi A, Van IJzendoorn MH, Joels T, Scharf M: Disorganized reasoning in Holocaust survivors: an attachment perspective. Am J Orthopsychiatry 2002; 72:194-203Crossref, Medline, Google Scholar
22. Florian V, Drori Y: [Mental Health Inventory (MHI): Psychometric characteristics and normative data regarding the Israeli population.] Psychology 1990; 1:26-35(Hebrew)Google Scholar
23. Schaefer ES, Edgerton M: Marital Autonomy and Relatedness Inventory (MARI). Princeton, NJ, Princeton University, 1979Google Scholar
24. Lyons-Ruth K, Bronfman E, Atwood G: A relational diathesis model of hostile-helpless states of mind: expressions in mother-infant interaction, in Attachment Disorganization. Edited by Solomon J, George C. New York, Guilford, 1999, pp 33-70Google Scholar
25. Yehuda R, Schmeidler J, Elkin A, Elson S, Siever L, Binder-Brynes K, Wainberg M, Aferiot D: Phenomenology and psychobiology of the intergenerational response to trauma, in International Handbook of Multigenerational Legacies of Trauma. Edited by Danieli Y. New York, Plenum, 1998, pp 639-655Google Scholar
26. Silverman PR, Nickman SL: Children’s construction of their dead parents, in Continuing Bonds: New Understandings of Grief. Edited by Klass D, Silverman PR, Nickman L. Washington, DC, Taylor & Francis, 1996, pp 73-86Google Scholar
27. Stroebe MS, Gergen MM, Gergen KJ, Stroebe W: Broken hearts or broken bonds: love and death in historical perspective. Am Psychol 1992; 47:1205-1212Crossref, Medline, Google Scholar
28. Fraley RC, Shaver PR: Loss and bereavement: attachment theory and recent controversies concerning “grief work” and the nature of detachment, in Handbook of Attachment. Edited by Cassidy J, Shaver P. New York, Guilford, 1999, pp 735-759Google Scholar
29. Frankl VE: Man’s Search for Ultimate Meaning. New York, Insight Books/Plenum, 1997Google Scholar
30. Paris J: Predispositions, personality traits, and posttraumatic stress disorder. Harv Rev Psychiatry 2000; 8:175-183Crossref, Medline, Google Scholar
31. Solomon Z: Transgenerational effects of the Holocaust: the Israeli research perspective, in International Handbook of Multigenerational Legacies of Trauma. Edited by Danieli Y. New York, Plenum, 1998, pp 69-84Google Scholar

