
Sex Differences in Response to Lithium Treatment
Abstract
OBJECTIVE: Although sex differences occur with some psychotropic drug treatments, they are not well defined for mood-stabilizing agents, including lithium. The authors’ goal was to investigate whether there are differences between the sexes in response to lithium. METHOD: Studies identified in a literature search were analyzed for reports of sex differences in clinical response to lithium in major affective syndromes. RESULTS: Data from 17 studies published in 1967–1998, involving 1,548 adults treated with lithium for a mean of 38.6 months (SD=30.5), yielded similar weighted response rates to lithium in 1,043 women (65.6% [N=684]) and 505 men (61.0% [N=308]). CONCLUSIONS: The results indicate little difference between the sexes in clinical response to lithium treatment of bipolar and related affective disorders.
Differences between men and women in clinical as well as pharmacokinetic responses to several psychotropic medicines, including antidepressants and antipsychotic agents, have been reported (1–3). In contrast, very little is known about possible sex-based differences in the effectiveness of mood-stabilizing agents in bipolar disorder (2–4), despite the obvious importance of optimizing the effectiveness and safety of mood-stabilizing therapy in women of childbearing age. Given the uncertainty about sex differences in treatment response in bipolar disorder and the very limited amount of relevant information on newer treatments, we undertook a systematic review of available published reports of clinical response in patients treated with lithium.
Method
We carried out computerized literature searches for reports of clinical trials of lithium in patients with major affective disorders, using the MEDLINE and Current Contents databases as well as references cited in the reports so identified. We included reports that 1) used lithium as the primary treatment or permitted separate analysis of lithium-treated subjects, 2) specified or permitted determination of response rates for men and women separately, 3) involved single-sex samples not otherwise selected, and 4) involved any duration of treatment and any number of subjects.
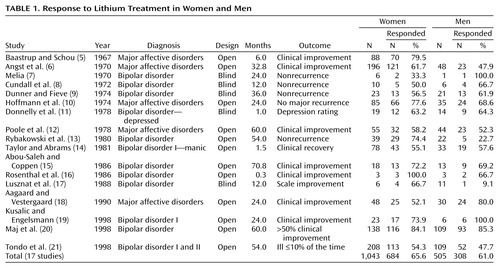
Response to treatment was defined in each study (Table 1). We tabulated the proportions of male and female responders to all male and female subjects and computed an overall proportion (weighted average) for the entire data set for comparison with a contingency table (chi-square at the stated degrees of freedom), setting two-tailed significance at 0.05.
Results
The search process yielded 16 published studies with the required information (5–20). We added data from a 1998 study of 317 adult patients with bipolar I and bipolar II disorder from our program who had not previously been divided by sex (21), for a total of 17 studies. All reports included data for both men and women, except for one study of 88 women with major affective disorders (5), whose response rate was within the range of rates for women in other studies. Data were obtained for 1,043 women and 505 men (N=1,548 subjects), with an average of 91 subjects/study (SD=93). Five studies involved mixed samples of patients with major affective disorders that included recurrent major depression as well as bipolar disorder (5, 6, 10, 12, 18), and one involved acutely manic patients (14). All but three short-term studies reporting on men and women (11, 14, 16) involved treatment that continued for at least 6 months.
Among the 16 studies with data for both sexes, eight suggested superior results in women, and eight suggested superior results in men, although results were closely similar in three of these overall, indicating no consistent sex preference (Table 1). Moreover, response rates for women compared with men in brief studies (less than 6 months; 58.0% versus 60.0%; χ2=0.06, df=1, n.s.) and long-term studies (65.0% versus 61.1%; χ2=3.52, df=1, n.s.) were similar, as they were in studies of bipolar disorder (64.1% versus 61.5%; χ2=0.88, df=1, n.s.) and major affective disorder (63.5% versus 59.9%; χ2=2.00, df=1, n.s.). As might be expected, double-blind studies yielded significantly lower overall response rates than open trials (54.7% versus 64.8%; χ2=4.84, df=1, p=0.03), although rates for men versus women in blind (52.8% versus 56.3%; χ2=0.03, df=1, n.s.) and open (61.9% versus 64.9%; χ2=2.26, df=1, n.s.) trials did not differ significantly.
Since response rates also did not differ significantly between studies of subjects with bipolar disorder (63.1%) and mixed affective disorder (64.9%) (χ2=2.82, df=1, n.s.) or between short-term (58.7%) and long-term (64.7%) studies (χ2=2.12, df=1, n.s.), all data were pooled. This pooled analysis yielded overall response rates of 65.6% (684 of 1,043) in women and 61.0% (308 of 505) in men. The response rate for all 1,548 patients was 64.1% (N=992); more women than men responded to lithium treatment (χ2=3.11, df=1, p=0.08) (Table 1).
Discussion
These results do not support the view that there are consistent and robust differences in clinical responsiveness in women and men in short-term or long-term studies involving lithium as a primary treatment for bipolar or major affective disorders. This lack of a clear sex difference, and even a nonsignificant tendency toward slight superiority in women, may be somewhat surprising because women are more likely than men to have rapid-cycling bipolar disorders (22). However, the sex difference in rapid cycling is substantially less than had been proposed and may have little effect on overall treatment responses because only about 15% of patients with bipolar disorder ever experience rapid cycling (22). Moreover, a recent study (23) did not find major differences in response to long-term treatment with lithium in patients with rapid-cycling disorder compared with patients who had other bipolar disorders.
The present results are limited by variability in the number of subjects, duration of treatment, and diagnostic and outcome measures in the 17 studies analyzed. Nevertheless, these studies do not indicate that women and men with bipolar or related major affective disorders differ appreciably in their clinical responses to lithium treatment. The sexes may show subtle differences in eliminating lithium, however: women may clear lithium less efficiently than men or vary more in lithium clearance, perhaps in association with the menstrual cycle (2) as well as during pregnancy (24). In addition, women may be at higher risk for hypothyroid effects of long-term lithium treatment (2). On the other hand, lithium appears to have more limited teratogenic risk than commonly used antimanic anticonvulsants (24–26). Therefore, lithium maintenance treatment remains an attractive option for the treatment of bipolar disorder in women of childbearing age.
 |
Received Dec. 7, 1999; revision received March 13, 2000; accepted April 14, 2000. From the International Consortium for Bipolar Disorder Research, Department of Psychiatry and Neuroscience Program, Harvard Medical School, Mailman Research Center, McLean Hospital, Belmont, Mass., and Massachusetts General Hospital; and the Department of Psychology, University of Cagliari, and the Lucio Bini-Stanley Foundation Mood Disorders Research Center, Cagliari, Sardinia, Italy. Address reprint requests to Dr. Viguera, Perinatal Psychopharmacology Unit, Department of Psychiatry, Massachusetts General Hospital, Fruit Street, Boston, MA 02114; [email protected] (e-mail). Supported in part by NIMH grants MH-01609 and MH-47370, a Theodore and Vada Stanley Foundation award, two National Alliance for Research on Schizophrenia and Depression investigator awards, a grant from the Bruce J. Anderson Foundation, and the McLean Private Donors Neuropharmacology Research Fund.
1. Yonkers KA, Kando JC, Cole JO, Blumenthal S: Gender differences in pharmacokinetics and pharmacodynamics of psychotropic medication. Am J Psychiatry 1992; 149:587–595Link, Google Scholar
2. Dawkins K: Gender differences in psychiatry: epidemiology and drug response. CNS Drugs 1995; 3:393–407Crossref, Google Scholar
3. Liebenluft E: Gender differences in major depressive disorder and bipolar disorder. CNS Spectrums 1999; 4:25–33Medline, Google Scholar
4. Goodwin FK, Jamison KR: Manic-Depressive Illness. New York, Oxford University Press, 1990Google Scholar
5. Baastrup PC, Schou M: Lithium as a prophylactic agent. Arch Gen Psychiatry 1967; 16:162–172Crossref, Medline, Google Scholar
6. Angst J, Weis P, Grof P, Baastrup PG, Schou M: Lithium prophylaxis in recurrent affective disorders. Br J Psychiatry 1970; 116:604–614Crossref, Medline, Google Scholar
7. Melia PI: Prophylactic lithium: a double-blind trial in recurrent affective disorders. Br J Psychiatry 1970; 116:621–624Crossref, Medline, Google Scholar
8. Cundall RL, Brooks PW, Murray LG: A controlled evaluation of lithium prophylaxis in affective disorders. Psychol Med 1972; 2:308–311Crossref, Medline, Google Scholar
9. Dunner DL, Fieve RR: Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry 1974; 30:229–233Crossref, Medline, Google Scholar
10. Hoffmann G, Gruneberger J. König P, Presslich O, Wolf R: Die mehrhjährige Lithiumtherapie affecktiver Störunder: Langzeiteffekte and Begleigterscheinungen. Psychiatr Clin (Basel) 1974; 7:129–141Medline, Google Scholar
11. Donnelly EF, Goodwin FK, Waldman IN, Murphy DL: Prediction of antidepressant responses to lithium. Am J Psychiatry 1978; 135:552–556Link, Google Scholar
12. Poole AJ, James HD, Hughes WC: Treatment experiences in the lithium clinic at St Thomas’ Hospital. J R Soc Med (Lond) 1978; 71:890–894Medline, Google Scholar
13. Rybakowski J, Chtopocka-Wozniak M, Kapelski Z, Strzyzewski W: The relative prophylactic efficacy of lithium against mania and depressive recurrences in bipolar patients. Int Pharmacopsychiatry 1980; 15:86–90Crossref, Medline, Google Scholar
14. Taylor MA, Abrams R: Prediction of treatment response in mania. Arch Gen Psychiatry 1981; 38:800–803Crossref, Medline, Google Scholar
15. Abou-Saleh MT, Coppen A: Who responds to prophylactic lithium? J Affect Disord 1986; 10:115–125Google Scholar
16. Rosenthal J, Strauss A, Minkoff L, Winston A: Identifying lithium-responsive bipolar depressed patients using nuclear magnetic resonance. Am J Psychiatry 1986; 143:779–780Link, Google Scholar
17. Lusznat RM, Murphy DP, Nunn CMH: Carbamazepine versus lithium in the treatment and prophylaxis of mania. Br J Psychiatry 1988; 153:198–204Crossref, Medline, Google Scholar
18. Aagaard J, Vestergaard P: Predictors of outcome in prophylactic lithium treatment: a two-year prospective study. J Affect Disord 1990; 18:259–266Crossref, Medline, Google Scholar
19. Kusalic M, Engelsmann F: Predictors of lithium treatment responsiveness in bipolar patients. Neuropsychobiology 1998; 37:146–149Crossref, Medline, Google Scholar
20. Maj M, Pirozzi R, Magliano L, Bartoli L: Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients in a lithium clinic. Am J Psychiatry 1998; 155:30–35Link, Google Scholar
21. Tondo L, Baldessarini RJ, Hennen J, Floris G: Lithium maintenance treatment of mania and depression in bipolar I and II disorders. Am J Psychiatry 1998; 155:638–645Link, Google Scholar
22. Tondo L, Baldessarini RJ: Rapid cycling in women and men with bipolar manic-depressive disorders. Am J Psychiatry 1998; 155:1434–1436Google Scholar
23. Baldessarini RJ, Tondo L, Hennen J: Effects of rapid cycling on response to lithium maintenance treatment in 360 bipolar I and II disorder patients. J Affect Disord (in press)Google Scholar
24. Yonkers KA, Little BB, March D: Lithium during pregnancy: drug effects and their therapeutic implications. CNS Drugs 1998; 9:261–269Crossref, Medline, Google Scholar
25. Cohen LS, Friedman JM, Jefferson JW, Johnson EM, Weiner ML: A reevaluation of risk of in utero exposure to lithium. JAMA 1994; 271:146–150Crossref, Medline, Google Scholar
26. Leppik IE, Wolff D, Purves S: Treatment of epilepsy in women of childbearing potential. CNS Drugs 1999; 11:191–206Crossref, Google Scholar

