
Affective Disorder in Juvenile Offenders: A Preliminary Study
Abstract
OBJECTIVE: The authors’ goal was to determine the prevalence of major mental disorders and substance abuse in adolescents admitted to a juvenile detention center. METHOD: As part of a routine mental health screening, modules from the Diagnostic Interview Schedule for Children were administered to 50 youths (11–17 years old) at an urban juvenile detention center. RESULTS: A high rate of affective disorder (42%) was found among these adolescents: 10 (20%) met criteria for mania, another 10 met criteria for major depressive disorder, and one met criteria for bipolar disorder, mixed type. Thirty (60%) met criteria for conduct disorder, and very high rates of alcohol, marijuana, and other substance dependence were found. There was a strong association between affective disorder and conduct disorder; adolescents with mania had much higher rates of reported abuse of substances other than alcohol or marijuana. CONCLUSIONS: Juvenile offenders have high rates of affective disorder. Further studies are needed to examine the relationship of affective disorder to substance abuse as well as to antisocial behavior.
Affective disorders may have a relationship to antisocial behavior in both adults and children. Zoccolillo (1) noted a greater than expected co-occurrence of depressive/anxiety disorders and conduct disorder among children in four major epidemiologic studies. The role of bipolar disorder in conduct disorder and delinquency has been examined. One study (2) found that juvenile offenders in residential treatment who met criteria for attention deficit hyperactivity disorder (ADHD) were also more likely to meet criteria for mania. Other studies found high rates of conduct disorder (3) and delinquency (4) in adolescents who met criteria for bipolar disorder. We incorporated a structured diagnostic interview into the routine mental screening of adolescents admitted to an urban juvenile detention center and found higher than expected rates of both major depressive disorder and mania.
METHOD
Fifty adolescents (45 boys and five girls) who were consecutively admitted to the Bexar County, Tex., Juvenile Detention Center were interviewed. Their mean age was 15.4 years (SD=1.4), and all were interviewed within 4 days of their admission to the center. The Diagnostic Interview Schedule for Children, version 2.3 (5 and unpublished 1993 paper by P. Fisher et al.) was incorporated into the youths’ routine mental health screening; adolescents in need of treatment were then referred to a psychiatric clinic in the detention center. The Diagnostic Interview Schedule for Children was part of routine care, not a research protocol. The adolescents were given the opportunity to refuse the interview, but none did.
The interview was administered by an examiner using a laptop computer who read each question to the subject and entered the response by using the keyboard. If a symptom was endorsed, questions were then asked about duration of the symptoms as well as degree of impairment. If an altered mood state occurred only during an episode of substance abuse, a diagnosis of mania or depression was not made. All of the adolescents appeared to understand and tolerate the interview well.
RESULTS
Twelve (24%) of the adolescents did not meet criteria for any diagnosis according to their responses to the Diagnostic Interview Schedule for Children. Adolescents could meet criteria for more than one diagnosis. Conduct disorder was the most prevalent diagnosis (N=30 [60%]); 12 (24%) of the offenders met criteria for oppositional defiant disorder. Only nine (18%) met criteria for ADHD. Ten (20%) met criteria for major depressive disorder, and 10 met criteria for mania. One of the adolescents with mania also met criteria for major depressive disorder and, therefore, met criteria for bipolar disorder, mixed type. Thus, a total of 21 (42%) of the adolescents met criteria for an affective disorder. The mean age at onset of depression was 11.2 years (SD=2.3), compared with 13.6 years (SD=1.5) for mania, a difference that was statistically significant (t=2.8, df=18, p=0.01).
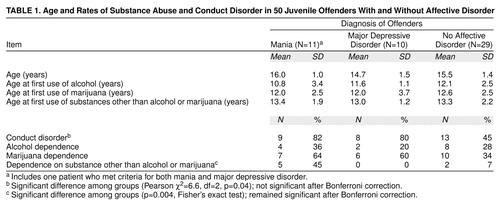
Five of the 11 adolescents with mania reported only irritability as their primary mood symptom (no euphoria), and three reported a mixture of irritability and euphoria. Three adolescents with mania reported euphoria without irritability. As shown in table 1, adolescents with mania or major depressive disorder were much more likely than those with no affective disorder to meet criteria for conduct disorder. For all of the adolescents with comorbid conduct disorder and affective disorder, the conduct disorder symptoms predated the onset of affective disorder.
Substance and alcohol use were highly prevalent: 14 (28%) of the adolescents were dependent on alcohol, although none showed signs of alcohol withdrawal while in detention. Marijuana dependence was endorsed by 23 (46%) of the adolescents, and seven (14%) reported that they were dependent on illegal substances other than alcohol or marijuana. Table 1 shows the relationship between affective disorder and substance abuse. Five of the seven adolescents with dependence on substances other than alcohol or marijuana met criteria for mania, but none of those with major depressive disorder reported such dependence. Only two of the 29 offenders without affective disorder were dependent on substances other than alcohol or marijuana. The mean age at which the three groups first used alcohol, marijuana, or other substances did not differ significantly.
DISCUSSION
Mania, ADHD, major depressive disorder, and alcohol/substance abuse and dependence were found to be quite common among adolescents detained in a urban juvenile detention center. The high rate of mania (22%) among these adolescents was striking and far above the rate of 1% of teenagers who met criteria for bipolar disorder in a community sample (6). Conduct disorder was more common among the offenders with affective disorder.
There are limitations to this preliminary study. We were not able to interview the parents of the adolescents with the Diagnostic Interview Schedule for Children, and it would be important to determine if they also would describe their adolescents as showing manic symptoms. The Diagnostic Interview Schedule for Children is a highly structured interview, and chronically oppositional and irritable adolescents might endorse symptoms of mania that a clinician would interpret as being part of the conduct disorder or oppositional defiant disorder diagnosis. On the other hand, by systematically asking about manic and depressive symptoms, the Diagnostic Interview Schedule for Children may be identifying problems that are viewed by clinicians as “typical conduct disorder behavior.”
Further studies should involve interviewing parents with the Diagnostic Interview Schedule for Children, using clinician ratings of mania, and using child care staff ratings of behavior to validate these preliminary findings. Confirmation of these elevated rates of mania in juvenile offender populations would have important treatment implications for mental health professionals working with individuals in the juvenile justice system.
Received Dec. 1, 1998; revision received April 5, 1999; accepted May 11, 1999. From the Division of Child and Adolescent Psychiatry, Department of Psychiatry, and the Department of Pediatrics, University of Texas Health Science Center at San Antonio; and Bexar County Juvenile Detention Center. Address reprints to Dr. Pliszka, University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Dr., San Antonio, TX 78284-7792; [email protected] (e-mail)
 |
1. Zoccolillo M: Co-occurrence of conduct disorder and its adult outcomes with depressive and anxiety disorders: a review. J Am Acad Child Adolesc Psychiatry 1992; 31:547–556Crossref, Medline, Google Scholar
2. Thompson LL, Riggs PD, Mikulich SK, Crowley TJ: Contribution of ADHD symptoms to substance problems and delinquency in conduct-disordered adolescents. J Abnorm Child Psychol 1996; 24:325–347Crossref, Medline, Google Scholar
3. Kovacs M, Pollock M: Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995; 34:715–723Crossref, Medline, Google Scholar
4. Geller B, Cooper TB, Sun K, Zimerman B, Frazier J, Williams M, Heath J: Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998; 37:171–178Crossref, Medline, Google Scholar
5. Shaffer D, Fisher P, Dulcan MK, Davies M, Piacentini J, Schwab-Stone ME, Lahey BB, Bourdon K, Jensen PS, Bird HR, Canino G, Regier DA: The NIMH Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3): description, acceptability, prevalence rates, and performance in the MECA Study (methods for the Epidemiology of Child and Adolescent Mental Disorders Study). J Am Acad Child Adolesc Psychiatry 1996; 35:865–877Crossref, Medline, Google Scholar
6. Lewinsohn PM, Klein DN, Seeley JR: Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995; 34:454–463Crossref, Medline, Google Scholar

