
Posttraumatic Stress and Depressive Reactions Among Children and Adolescents After the 1999 Earthquake in Ano Liosia, Greece
Abstract
OBJECTIVE: This study evaluated the severity of posttraumatic stress and depressive reactions among children and adolescents 3 months after the 1999 earthquake in Ano Liosia, Greece, and additionally assessed the relationship of these reactions to objective and subjective features of earthquake exposure, sex, school level, postearthquake difficulties, death of a family member, and thoughts of revenge. METHOD: This school-based study of 1,937 students was conducted in two differentially exposed cities (Ano Liosia, at the epicenter, and Dafni, 10 kilometers from the epicenter) with an earthquake exposure questionnaire, the UCLA Posttraumatic Stress Disorder (PTSD) Reaction Index, and the Depression Self-Rating Scale. RESULTS: Endorsement of earthquake-related exposure items between the two cities was congruent with the extent of earthquake impact in each city. Median PTSD Reaction Index scores were significantly higher in Ano Liosia. The estimated rates of PTSD and clinical depression for both cities combined were 4.5% and 13.9%, respectively. Depression, subjective and objective earthquake-related experiences, and difficulties at home accounted for 41% of the variance in severity of PTSD reactions. PTSD score was the single most powerful variable predicting depression (36% of the variance), with only sex making a small but significant additional contribution. CONCLUSIONS: This study demonstrated the feasibility of conducting large-scale school-based postdisaster mental health screening for planning intervention strategies. The present findings regarding PTSD and depression indicate the need to provide targeted specialized postdisaster mental health services to subgroups with significant levels of posttraumatic stress and depressive reactions after an earthquake of moderate intensity.
A growing body of literature has addressed the psychological sequelae among children and adolescents after natural disasters. Hurricanes and earthquakes have typically been the more thoroughly studied disasters. Category 4 hurricanes (e.g., Hugo and Andrew) have been associated with moderate levels of posttraumatic stress reactions among school-age children (1–3). Category 5 Hurricane Mitch was found to be associated with severe posttraumatic stress and depressive reactions among highly exposed adolescents (4). Studies have indicated that children and adolescents exposed to the catastrophic 1988 Spitak earthquake in Armenia were suffering from chronic severe posttraumatic stress disorder (PTSD) symptoms years after the earthquake (5, 6). In addition to PTSD symptoms, children in Armenia were also experiencing comorbid depression and separation anxiety. A study among children and adolescents after the 1999 Chi-Chi earthquake in Taiwan (7) indicated that children near the epicenter were experiencing moderate levels of posttraumatic stress reactions 1 year after the earthquake.
Researchers have begun to more rigorously evaluate exposure and its relationship to posttraumatic stress reactions. Among adolescents exposed to Hurricane Mitch, there was a strong relationship between aspects of objective and subjective traumatic exposure experiences and severity of posttraumatic stress and depressive reactions (4). Most studies have found girls to score higher than boys on PTSD measures (3, 5, 8, 9), while one study found girls to report greater subjective appraisal of danger (4).
With regard to age, Green et al. (10) did not find any significant difference in the diagnosis of “probable PTSD” among three age groups (2–7, 8–11, and 12–15 years) after the Buffalo Creek disaster. However, there was a significant difference in the average number of PTSD symptoms, with the youngest age category showing fewer symptoms. After Hurricane Hugo, Shannon et al. (8) reported that children younger than 13 were more likely to test positive for posttraumatic stress syndrome than older children. After the earthquake in Armenia, there was no association found between the severity of PTSD and age among students 8–16 years old (11). In a study among students exposed to the Chi-Chi earthquake in Taiwan (7), elementary school students experienced more severe PTSD symptoms compared to junior high school students.
Evaluation of thoughts of revenge among adolescents after Hurricane Mitch revealed an association between vengeful thoughts and severity of PTSD symptoms (4). Vengeful thoughts were directed mostly against the government for not protecting the victims and their families against the calamity and not providing adequate relief in the aftermath.
With regard to postdisaster adversities, La Greca et al. (12) reported that “major life events” (e.g., death or hospitalization of a family member) had an additive effect on children’s postdisaster reactions. Lonigan et al. (13) noted that children whose parents were unemployed experienced more PTSD symptoms. In contrast, social support was found to diminish the impact of the disaster, with the support of teachers, as opposed to parents and friends, being associated with lower levels of PTSD symptoms (3, 12). Relocation did not have a negative impact on posttraumatic symptoms of students in Armenia after the Spitak earthquake (14) or the Chi-Chi earthquake in Taiwan (15). However, among relocated students in Taiwan, those who lived with their parents had fewer acute PTSD symptoms.
The Ano Liosia Earthquake
On September 7, 1999, an earthquake measuring 5.9 on the Richter scale struck the northern part of Greater Athens. One of the most severely affected regions was the municipality of Ano Liosia, a working-class community with a population of approximately 30,000. Eighty percent of the houses were severely damaged. Of these, 60% had to be demolished, and 40% required extensive repairs before the residents could return to their homes. Ten people were killed, all of whom had been buried under the ruins of their homes. At the time of the earthquake, the municipality was still recovering from the devastating effects of a 1996 flood that had caused loss of homes and property damage. Less affected by the earthquake was Dafni, a city on the outskirts of Athens, 10 km from the epicenter. In Dafni, there were no deaths attributable to the earthquake, and damage to buildings was significantly less compared with Ano Liosia.
Immediately after the earthquake, the Ministry of Health and Social Welfare sent mental health teams to provide psychological support to the people of the affected areas. A multidisciplinary child psychiatric team from Attiki Child Psychiatric Hospital was assigned to Ano Liosia to plan a postdisaster public mental health response for children and adolescents. Schoolwide screenings were performed in Ano Liosia. Students from Dafni, the less affected municipality, were evaluated to assess their earthquake-related experiences, posttraumatic stress, and depressive reactions. This article presents the findings from the evaluations in these two cities.
Method
Subjects
In December 1999, 3 months after the earthquake, a total of 1,685 students (738 boys and 947 girls), ages 9–18 years, from 13 schools in Ano Liosia, the city at the epicenter, were evaluated. These schools included seven primary schools, and two junior and four senior high schools. All but three schools in Ano Liosia participated in the survey. At the time of the survey, these three schools had already made arrangements for services to be provided through insurance companies. The authorities assigned to these three schools objected to the proposed schoolwide screenings because they were concerned that they might have a detrimental effect on the children. There was no apparent reason why the lack of participation of these three schools in the survey would bias the findings.
Four months after the earthquake, a comparison group of 252 students from Dafni, where there was no loss of life and substantially less property damage, was evaluated. A convenience group from three schools—one set of students each from a primary, a junior, and a senior high school (of a total of eight primary, two junior, and two senior high schools)—was selected. The three schools were ones in which the mental health team conducting needs assessment had a good working relationship with the school masters. This group consisted of 109 boys and 143 girls, ages 9–18 years. A greater number of girls than boys surveyed in each of the two municipalities was likely due to the boys being more often taken out of school to work. In each city, the questionnaires were administered to all classrooms at each school. The response rate was 99% of those present in school that day.
The study was conducted with the permission of the Ministry of Education. The interview procedures were explained to the students, and the parents gave written consent for their children to participate. All students gave their assent before participating. Only one parent refused to give permission for her child’s participation, and no student refused to be evaluated.
Instruments
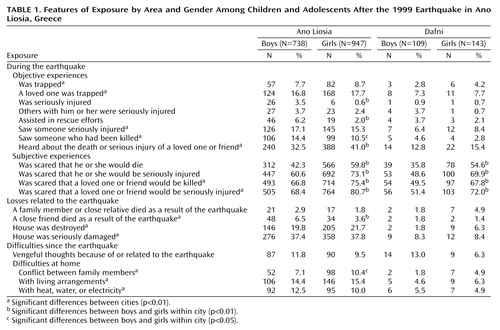
An earthquake exposure scale was adapted from a prior hurricane exposure scale based on DSM-IV A-1 and A-2 criteria for PTSD (4). The instrument included eight items evaluating objective and four items evaluating subjective features of exposure. It also included demographic items and questions about the loss of a loved one, damage or destruction to a home, postearthquake adversities, family problems, and thoughts of revenge. These items were rated as yes or no (Table 1). Total score for endorsement of objective and subjective experience was calculated by adding the yes responses within each category.
The Posttraumatic Stress Disorder Reaction Index is a 22-item self-report scale based on DSM-IV PTSD criteria. It includes items to evaluate all B, C, and D PTSD symptoms and two items to assess the associated features of trauma-related guilt and fear of recurrence. The frequency of symptom occurrence during the past month was rated on a 5-point Likert scale, ranging from 0=not at all to 4=most of the time. This measure is a revision of a widely used scale whose psychometric properties have been previously reported (11). The psychometric properties of the revised instrument used in this study have also been reported (16). In that study, the revised instrument demonstrated high internal consistency, with Cronbach’s alpha of 0.92 and a test-retest reliability coefficient of 0.84. With regard to validity, using a diagnosis of PTSD derived from the Schedule for Affective Disorders and Schizophrenia—Lifetime Version (17), a cutoff score of 38 had a sensitivity of 0.93 and specificity of 0.87 in detecting PTSD. In the present study, Cronbach’s alpha for internal consistency was 0.88.
The Depression Self-Rating Scale (18) contains 21 items that relate to affective, cognitive, and behavioral symptoms of depression. Ratings for the frequency of these symptoms over the previous 2 weeks are made on a 3-point scale: 0=never, 1=sometimes, 2=most of the time. Psychometric properties of this instrument have been previously reported (18). A score of 17 or above is highly associated with a diagnosis of major depression, dysthymic disorder, or adjustment disorder with depressed mood.
Translation and back-translation of these instruments followed previously published guidelines (19). All questionnaires were pretested with children and adolescents who had been exposed to the earthquake.
Statistical Analysis
Continuous data are described as means and standard deviations and as quartiles (median, first, second, and third) where appropriate. T tests were used to compare mean values. Differences in median values were examined by nonparametric Wilcoxon rank-sum tests. Chi-square tests or Fisher’s exact tests were used to examine associations between categorical variables. Spearman’s r was used to evaluate the relationship between PTSD Reaction Index and Depression Self-Rating Scale scores.
Stepwise multiple linear regression analyses were performed for the combined groups to identify independent predictors of PTSD Reaction Index and Depression Self-Rating Scale scores. A logarithmic transformation of the PTSD Reaction Index score was used to satisfy distributional assumptions for the regression analysis. A p value of less than 0.05 was considered significant. In order to ensure that appropriate statistical analyses were used for tests of central tendency, the skewness of PTSD Reaction Index and Depression Self-Rating Scale scores was examined. Distribution of PTSD Reaction Index score was positively skewed (sk=1.13), reflecting significantly higher mean values compared to median values. Consequently, median values of the PTSD Reaction Index are reported. Mean values are also included for comparison with other postdisaster studies. The distribution of the Depression Self-Rating Scale was not significantly skewed (sk=0.7).
For the overall group, the half-width for the confidence interval for differences between site-specific rates was approximately 7%. For the present analyses, this level of precision is adequate: if the true difference between Ano Liosia and Dafni is at least 9.5%, we can detect the difference at 80% power using a 5% two-tailed test.
Results
Features of Earthquake Exposure and Impact
Table 1 shows the frequency of endorsement of objective and subjective earthquake-related exposure items by city and gender. In Ano Liosia, compared with Dafni, all items relating to objective exposure experiences were more frequently endorsed, consistent with the levels of destruction and loss of life in the two regions. The mean number of endorsed objective exposure items was significantly higher in Ano Liosia (Ano Liosia: mean=1.00, SD=1.21; Dafni: mean=0.40, SD=0.87) (t=–7.3, df=1933, p<0.001). There was no significant difference between boys and girls with regard to the mean number of endorsed objective exposure items. The subjects from Ano Liosia more frequently endorsed items relating to subjective experiences during the earthquake (Ano Liosia: mean=2.67, SD=1.39; Dafni: mean=2.30, SD=1.62) (t=–3.8, df=1933, p<0.001). For both groups combined, girls more frequently endorsed subjective exposure items (girls: mean=2.86, SD=1.34; boys: mean=2.31, SD=1.47) (t=–8.6, df=1933, p<0.001).
Significantly more students in Ano Liosia (4.9%) reported loss of a close friend because of the earthquake compared with students in Dafni (1.6%) (χ2=5.6, df=1, p<0.02). In Ano Liosia, endorsement of serious damage to the home (38%) was significantly higher than in Dafni (8.3%) (χ2=84.9, df=1, p<0.001). The same was true for destruction of residence (21% in Ano Liosia, 4.4% in Dafni) (χ2=39.3, df=1, p<0.001). The rates in Ano Liosia reflect the degree of impact of the earthquake in that municipality. The rates of reported damage or destruction did not differ significantly between the boys and the girls in both locations.
There was no significant difference between the two cities with regard to vengeful thoughts since the earthquake (χ2=0.5, df=1, n.s.). However, for both groups combined, the boys endorsed this item more frequently than the girls: boys=12.0%; girls=9.1% (χ2=4.3, df=1, p=0.04). Difficulties at home were more frequently reported in Ano Liosia, including conflicts between family members (Ano Liosia: 8.9%; Dafni: 3.6%) (χ2=8.2, df=1, p=0.004), difficulties with living arrangements (Ano Liosia: 14.9%; Dafni: 5.6%) (χ2=16.2, df=1, p<0.001), and lack of heat, water, or electricity (Ano Liosia: 11.1%; Dafni: 5.2%) (χ2=8.3, df=1, p=0.004). There was no difference between boys and girls with regard to difficulties at home.
Posttraumatic Stress and Depressive Reactions
The median PTSD Reaction Index score was significantly higher in Ano Liosia (11; first to third quartiles=5–20) compared with Dafni (9; first to third quartiles=4–17.5) (Wilcoxon’s rank sum test: z=–2.3, p=0.02). The mean PTSD Reaction Index scores in the two cities did not differ significantly (Ano Liosia: mean=13.8, SD=11.2; Dafni: mean=12.6, SD=11.6) (t=–1.6, df=1930, n.s.).
Neither median nor mean Depression Self-Rating Scale scores were significantly different between the two cities. The median Depression Self-Rating Scale scores were the following: Ano Liosia=10 (first to third quartiles=6–15); Dafni=9 (first to third quartiles=6–14) (Wilcoxon’s rank sum test: z=0.3, n.s.). The mean Depression Self-Rating Scale score was 10.6 (SD=6.1) for Ano Liosia and 10.3 (SD=6.3) for Dafni (t=0.4, df=1894, n.s.).
For both cities combined, the girls had higher median PTSD Reaction Index scores (girls’ median=12, first to third quartiles=6–22; boys’ median=8, first to third quartiles=4–16) (Wilcoxon’s rank sum test: z=–7.7, p<0.001) and higher mean PTSD Reaction Index scores (girls’ mean=15.3, SD=11.7; boys’ mean=11.6, SD=10.4) (t=–7.2, df=1930, p<0.001). Also, for both cities combined, the girls had higher median Depression Self-Rating Scale scores (girls’ median=11, first to third quartiles=7–16; boys’ median=8, first to third quartiles=5–13) (Wilcoxon’s rank sum test: z=–7.6, p<0.001) and higher mean Depression Self-Rating Scale scores (girls’ mean=11.5, SD=6.2; boys’ mean=9.4, SD=5.9) (t=–7.3, df=1894, p<0.001).
For the total group, there was a significant positive correlation between PTSD Reaction Index and Depression Self-Rating Scale scores (rs=0.55, N=1,894, p<0.001). There was a similar positive correlation within each of the two cities (Ano Liosia: rs=0.56, N=1,644, p<0.01; Dafni: rs=0.51, N=250, p<0.001).
For the total group, there were significant differences in mean PTSD Reaction Index and mean Depression Self-Rating Scale scores between those with and without difficulties at home since the earthquake. The mean PTSD Reaction Index score for those with difficulties at home since the earthquake (N=434) was higher (mean=20.2; SD=12.7) than for those without difficulties (N=1,503) (mean=11.7, SD=10.1) (t=14.5, df=1935, p<0.001). The mean Depression Self-Rating Scale score for those with difficulties (N=425) was also higher (mean=12.5, SD=6.6) than for those without difficulties (N=1,476) (mean=9.5, SD=5.8) (t=9.2, df=1899, p<0.001).
Estimated Rates of PTSD and Depression
The estimated rates of PTSD (when using a cutoff of 38 for the PTSD Reaction Index) and clinical depression (when using a cutoff of 17 for the Depression Self-Rating Scale) for both cities combined were 4.5% and 13.9%, respectively, with no significant differences in the rates between the cities.
Independent Predictors of Severity of PTSD and Depression
Table 2 presents a stepwise multiple regression analysis of the contribution of depression, earthquake-related experience variables, sex, and school level in predicting the severity of posttraumatic stress reactions. It displays the adjusted R2, the change in R2, the standardized regression coefficient (beta), and partial correlations. At step 1, the strongest predictor of the severity of posttraumatic stress reaction was the level of depression, which accounted for 27% of the total variance. The next variable contributing significantly was severity of subjective earthquake-related experiences, accounting for another 11% of the variance, followed by the severity of objective earthquake-related experiences (2%) and difficulties at home (1%). Damage to home, school level (age), sex, and thoughts of revenge, taken together, contributed an additional 1% to the variance.
Table 3 presents a stepwise multiple regression analysis for both groups of the contribution of posttraumatic stress reaction, earthquake-related experience variables, sex, and school level to predicting the severity of depression. At step 1, the most significant variable that predicted the severity of depression score was PTSD Reaction Index score, which accounted for 36% of the total variance in depression severity. The only other variable contributing significantly was gender, which accounted for 1% of the variance.
Discussion
This study, evaluating posttraumatic stress and depressive reactions, represents one of the largest postearthquake screenings of children and adolescents after a natural disaster. It included most of the children and adolescents who were exposed at the epicenter of the 1999 earthquake in the city of Ano Liosia, Greece, and a comparison group of students from the nearby municipality of Dafni. The study demonstrated the feasibility of conducting large-scale, comprehensive systematic screening of primary, junior, and senior high school students after a disaster. The screening was conducted by using trauma-specific psychometric instruments that assessed exposure and distress reactions. The survey was administered to classrooms of students, taking one classroom period for administration.
Reports from the two groups of students regarding the extent of damage and destruction they experienced were consistent with the impact of the earthquake in the two cities. The higher frequency of endorsement of items related to objective features of exposure to trauma by the students in Ano Liosia was also consistent with the earthquake’s impact in that municipality. Endorsement of some items from the subjective features of exposure followed the same pattern, while others did not. Compared to the study after Hurricane Mitch, where items of subjective features of exposure did not discriminate between exposure groups (4), in the present study, these features demonstrated somewhat better discriminatory power. For future studies, the use of a continuous scaled response for these items is recommended as they will likely be more sensitive in detecting differences across differentially exposed populations. Similar to the findings in Nicaragua (4), the present study found that girls scored higher than boys on items regarding subjective features of exposure. However, it remains unclear whether girls actually experience more subjective fear or are simply more willing to endorse these items.
A significant minority of students in each city (approximately 10%) endorsed having vengeful thoughts after the earthquake. For both cities combined, higher percentages of boys than girls endorsed having such vengeful thoughts. For example, youngsters expressed anger and vengeful thoughts against the government for not having properly supervised the engineers responsible for the construction of buildings and against God for not protecting them from the earthquake. Prior reports have also documented vengeful thoughts involving attributions of blame after natural disasters (4, 20). Because thoughts of revenge can be detrimental to the recovery of children and adolescents, postdisaster interventions should include exploration and treatment of such thoughts.
Postearthquake difficulties at home, including conflicts between family members; difficulties with living arrangements; and difficulties with heat, water, or electricity, were more frequently reported in Ano Liosia and were congruent with the more destructive impact of the earthquake in that city. Disaster-related adversities have been reported to interfere with recovery from posttraumatic stress reactions and to be associated with comorbid depression (5, 21). The significant difference in mean PTSD and depression scores between those with and without postearthquake difficulties at home suggests that a comprehensive postdisaster mental health program for children and their families should include assistance in building problem-solving skills and enhancing coping strategies with regard to secondary adversities.
Median PTSD Reaction Index scores were higher in Ano Liosia, as would be predicted in a “dose of exposure” model. Prior studies in Armenia, Nicaragua, and Taiwan that compared differentially exposed groups found significantly higher mean PTSD Reaction Index scores in the high-exposure groups (4, 5, 7). The lack of significant differences in the present study in mean PTSD Reaction Index scores between the two municipalities may reflect the small difference in severity of exposure to the trauma. Adolescents in Dafni may have experienced more PTSD symptoms than expected because of vicarious traumatization. For weeks after the earthquake, the media provided repeated graphic coverage of the event. Such coverage may have constituted repeated traumatic reminders that rekindled symptoms or interfered with their resolution (22). A similar lack of difference in PTSD Reaction Index scores between high- and low-exposure groups was noted by Shaw et al. (23) among elementary school students after Hurricane Andrew.
PTSD Reaction Index scores in this study were relatively lower in comparison with PTSD Reaction Index scores reported after the Spitak earthquake (5, 6), the Chi-Chi earthquake (7), and Hurricane Mitch (4). The lower scores in Greece are directly related to the lower levels of destruction, morbidity, and mortality of the disaster. However, despite these lower scores, approximately 4.5% of the students evaluated were estimated to have PTSD. In addition to those meeting criteria for the diagnosis of PTSD, another group that would probably need intervention would be the students with subthreshold PTSD. The estimation of 4.5% with PTSD provides important information for planning needed resources and services for an appropriate postdisaster mental health intervention program. Such an intervention program is needed in light of prior findings that such posttraumatic stress reactions are likely to become chronic (6).
Depression scores did not differ between cities, with both cities scoring below the clinical cutoff. However, the estimated rate of 13.9% for clinical depression is significant. Prior disaster studies among highly exposed subjects have found the rates of depressive disorder to be similar to, or lower than, the rates of PTSD (4, 5). In contrast, among survivors with lower levels of traumatic exposure, rates of depression have exceeded those of PTSD, as in the city of Leon, where exposure to Hurricane Mitch was low (4). Depressive symptoms were probably due to multiple losses, both personal losses and loss of community, and ongoing adverse living conditions. The present finding also indicates that a significant number of children will need specialized interventions for depression after a moderate earthquake. It would have been useful to have had baseline data for the prevalence of PTSD and depression for these age groups in Greece for comparison. Community studies elsewhere, where no major disasters have occurred, have reported the prevalence of these disorders (24). With regard to gender effects, girls scored higher than boys on both the PTSD Reaction Index and the Depression Self-Rating Scale. These findings are consistent with the literature on gender differences in posttraumatic stress reactions (3, 4, 8) and depression (4). They may reflect actual differences in symptoms between boys and girls or reflect more willingness on the part of girls to endorse symptoms.
This study examined a conceptual model for the prediction of severity of posttraumatic stress and depressive reactions. Depression was found to be the best predictor of severity of posttraumatic stress reaction (explaining 27% of the variance). Alternatively, PTSD Reaction Index score was the best predictor of depression, explaining 36% of the variance. These findings are consistent with the high correlation between PTSD Reaction Index and Depression Self-Rating Scale scores. This correlation may be because the students who suffered more severe traumatic exposures (resulting in high levels of PTSD) also experienced more losses and adversities (resulting in higher levels of depression). Additionally, PTSD symptoms may have given rise to, or exacerbated, depressive symptoms, and depressive symptoms may have interfered with the resolution of PTSD symptoms. Further studies after natural disasters are needed to clarify the etiology of, and relationship between, these two disorders.
The severity of subjective earthquake-related experiences made a relatively large contribution to predicting PTSD (11%), with objective features making a relatively minor contribution. This is in contrast to findings after Hurricane Mitch (4), where injury, death, and destruction were more prevalent, and objective features contributed more than subjective features to predicting PTSD. The relative predictive power of objective versus subjective features of exposure in predicting the severity of PTSD may vary with the magnitude of a disaster. Future studies are needed to examine whether the less the objective impact, the more important the role of subjective experiences are in predicting the severity of PTSD.
In summary, this study demonstrated the feasibility of conducting a large-scale school-based postdisaster mental health screening. The findings regarding PTSD and depression provide important public mental health information for planning resources and strategies needed for postdisaster mental health recovery programs and indicate the need, even after an earthquake of moderate severity, for specialized trauma and depression services for targeted subgroups. Future studies are needed to evaluate the longitudinal course of PTSD and depression and the relationship of the course of recovery to the risk factors identified in this study.
 |
 |
 |
Received Jan. 29, 2003; revision received Oct. 15, 2003; accepted April 9, 2004. From Attiki Child Psychiatric Hospital, Athens, Greece; and UCLA/Duke University National Center for Child Traumatic Stress, Department of Psychiatry and Biobehavioral Sciences, University of California. Address correspondence and reprint requests to Dr. Goenjian, UCLA/Duke University National Center for Child Traumatic Stress, CNS Network, 12772 Valley View, Suite 3, Garden Grove, CA 92845; [email protected] (e-mail).
1. Belter RW, Dunn SE, Jeney P: The psychological impact of Hurricane Hugo on children: a needs assessment. Advances in Behaviour Research and Therapy 1991; 13:155–161Crossref, Google Scholar
2. Garrison CZ, Weinrich MW, Hardin SB, Weinrich S, Wang, L: Post-traumatic stress disorder in adolescents after a hurricane. Am J Epidemiol 1993; 138:522–530Crossref, Medline, Google Scholar
3. Vernberg EM, Silverman WK, La Greca AM, Prinstein MJ: Prediction of posttraumatic stress symptoms in children after Hurricane Andrew. J Abnorm Psychol 1996; 105:237–248Crossref, Medline, Google Scholar
4. Goenjian AK, Molina L, Steinberg AM, Fairbanks LA, Alvarez ML, Goenjian HA, Pynoos RS: Posttraumatic stress and depressive reactions among Nicaraguan adolescents after Hurricane Mitch. Am J Psychiatry 2001; 158:788–794Link, Google Scholar
5. Goenjian AK, Pynoos RS, Steinberg AM, Najarian LM, Asarnow JR, Karayan I, Ghurabi M, Fairbanks LA: Psychiatric comorbidity in children after the 1988 earthquake in Armenia. J Am Acad Child Adolesc Psychiatry 1995; 34:1174–1184Crossref, Medline, Google Scholar
6. Goenjian AK, Karayan I, Pynoos RS, Minassian D, Najarian LM, Steinberg AM, Fairbanks LA: Outcome of psychotherapy among early adolescents after trauma. Am J Psychiatry 1997; 154:536–542Link, Google Scholar
7. Chen S-H, Lin Y-H, Tseng H-M, Wu Y-C: Posttraumatic stress reactions in children and adolescents one year after the 1999 Taiwan Chi-Chi earthquake. J Chinese Institute of Engineers 2002; 25:597–608Crossref, Google Scholar
8. Shannon MP, Lonigan CJ, Finch AJ Jr, Taylor CM: Children exposed to disaster, I: epidemiology of post-traumatic symptoms and symptom profiles. J Am Acad Child Adolesc Psychiatry 1994; 33:80–93Crossref, Medline, Google Scholar
9. Shioyama A, Uemoto M, Shinfuku N, Ide H, Sek W, Mori S, Inoue S, Natsuno R, Asakawa K, Osabe H: [The mental health of schoolchildren after the Great Hanshin-Awaji earthquake, II: longitudinal analysis.] Seishin Shinkeigaku Zasshi 2000; 102:481–497 (Japanese)Medline, Google Scholar
10. Green BL, Korol M, Grace MC, Vary MG, Leonard AC, Gleser GC, Smitson-Cohen S: Children and disaster: age, gender, and parental effects on PTSD symptoms. J Am Acad Child Adolesc Psychiatry 1991; 30:945–951Crossref, Medline, Google Scholar
11. Pynoos R, Goenjian A, Tashjian M, Karakashian M, Manjikian R, Manoukian G, Steinberg AM, Fairbanks LA: Post-traumatic stress reactions in children after the 1988 Armenian earthquake. Br J Psychiatry 1993; 163:239–247Crossref, Medline, Google Scholar
12. La Greca AM, Silverman WK, Vernberg EM, Prinstein MJ: Symptoms of posttraumatic stress in children after Hurricane Andrew: a prospective study. J Consult Clin Psychol 1996; 64:712–723Crossref, Medline, Google Scholar
13. Lonigan CJ, Shannon MP, Taylor CM, Finch AJ Jr, Salle FR: Children exposed to disaster, II: risk factors for the development of post-traumatic symptomatology. J Am Acad Child Adolesc Psychiatry 1994; 33:94–105Crossref, Medline, Google Scholar
14. Najarian LM, Goenjian AK, Pelcovitz D, Mandel F, Najarian B: Relocation after a disaster: posttraumatic stress disorder in Armenia after the earthquake. J Am Acad Child Adolesc Psychiatry 1996; 35:374–383Crossref, Medline, Google Scholar
15. Soong T-W, Lee Y-C, Huang R-R, Liu S-Y, Chen Y-S: A comparative study of post-traumatic symptoms between students living at Yu-Chih and relocating to Kaohisung after the Chi-Chi earthquake, in Proceedings of the International Workshop on Annual Commemoration of Chi-Chi Earthquake. Taipei, Taiwan, National Center for Research on Earthquake Engineering, 2000, pp 308–317Google Scholar
16. Rodriguez N, Steinberg AM, Saltzman W, Pynoos RS: UCLA PTSD Reaction Index: psychometric analysis, in Proceedings of the International Society for Traumatic Stress Studies. Northbrook, Ill, ISTSS, 2001Google Scholar
17. Mannuzza S, Fyer AJ, Klein DF, Endicott J: Schedule for Affective Disorders and Schizophrenia—Lifetime Version modified for the study of anxiety disorders (SADS-LA): rationale and conceptual development. J Psychiatr Res 1986; 20:317–325Crossref, Medline, Google Scholar
18. Asarnow JR, Carlson GA: Depression Self-Rating Scale: utility with child psychiatric inpatients. J Consult Clin Psychol 1985; 53:491–499Crossref, Medline, Google Scholar
19. Brislin RW: Introduction, in Translations: Applications and Research. Edited by Brislin RW. New York, John Wiley & Sons, 1976, pp 1–43Google Scholar
20. Goenjian A: A mental health relief programme in Armenia after the 1988 earthquake: implementation and clinical observations. Br J Psychiatry 1993; 163:230–239Crossref, Medline, Google Scholar
21. Carr VJ, Lewin TJ, Kenardy JA, Webster RA, Hazell PL, Carter GL, Williamson M: Psychosocial sequelae of the 1989 Newcastle earthquake, III: role of vulnerability factors in post-disaster morbidity. Psychol Med 1997; 27:179–190Crossref, Medline, Google Scholar
22. Nader KO, Pynoos RS, Fairbanks LA, al-Ajeel M, al-Asfour A: A preliminary study of PTSD and grief among the children of Kuwait following the Gulf crisis. Br J Clin Psychol 1993; 32(part 4):407–416Google Scholar
23. Shaw JA, Applegate B, Tanner S, Perez D, Rothe E, Campo-Bowen AE, Lahey BL: Psychological effects of Hurricane Andrew on an elementary school population. J Am Acad Child Adolesc Psychiatry 1995; 34:1185–1192Crossref, Medline, Google Scholar
24. Kilpatrick DG, Ruggiero KJ, Acierno R, Saunders BE, Resnick HS, Best CL: Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: results from the National Survey of Adolescents. J Consult Clin Psychol 2003; 71:692–700Crossref, Medline, Google Scholar

