
Can Psychiatry Cross the Quality Chasm? Improving the Quality of Health Care For Mental and Substance Use Conditions
Abstract
In 2001, a seminal Institute of Medicine report, Crossing the Quality Chasm: A New Health System for the 21st Century , put forth a comprehensive strategy for improving the quality of U.S. health care. This strategy attained considerable traction within the overall U.S. health care system and subsequent attention in the mental health community as well. A new Institute of Medicine report, Improving the Quality of Health Care for Mental and Substance Use Conditions , examines the quality chasm strategy in light of the distinctive features of mental and substance use health care, including concerns about patient decision-making abilities and coercion into care, a less developed quality measurement and improvement infrastructure, lagging use of information technology and participation in the development of the National Health Information Infrastructure, greater separations in care delivery accompanied by more restrictions on sharing clinical information, a larger number of provider types licensed to diagnose and treat, more solo practice, and a differently structured marketplace. This article summarizes the Institute of Medicine’s analysis of these issues and recommendations for improving mental and substance use health care and discusses the implications for psychiatric practice and related advocacy efforts of psychiatrists, psychiatric organizations, and other leaders in mental and substance use health care.
Over the past decade, numerous studies have documented significant quality problems in general health care, as well as in mental and substance use care. In 2001, a seminal Institute of Medicine report, Crossing the Quality Chasm: A New Health System for the 21st Century(1) , put forth a comprehensive strategy for addressing these problems that has attracted the attention of leaders in numerous health care fields. Intended for use by the overall health care system, this report did not explicitly address mental and substance use conditions, and it was unclear to what extent its approach might apply to these. To address this question, a coalition of public and private funders asked the Institute of Medicine to explore the implications of the quality chasm report for mental health and addictive disorders, identify barriers to achieving significant improvements, and develop an action agenda for improving health care for mental and substance use conditions. In response, the Institute of Medicine convened the Committee on Crossing the Quality Chasm: Adaptation to Mental Health and Addictive Disorders (the committee). The committee’s analysis and recommended action agenda are contained in the report titled Improving the Quality of Health Care for Mental and Substance Use Conditions(2) .
This article 1) briefly summarizes the findings, conclusions, recommendations, and controversies of the 500-page report; 2) discusses the implications for psychiatrists in their daily practice; and 3) identifies changes in public policy recommended by the report that psychiatrists, psychiatric organizations, and other leaders in mental and substance use health care should champion.
The Quality Chasm and the Institute of Medicine Framework for Improvement
Despite the availability of outstanding health care in the United States, several independent reports, including the Institute of Medicine’s quality chasm report, found that the gap between the care that patients could receive and do receive is greater than a fissure; it is a chasm. Problems include the underuse, overuse, and misuse of interventions and other errors in care. These problems are found in all types of services (i.e., preventive, acute, and chronic), patient age groups, treatment settings, managed and unmanaged care, and somatic and behavioral health services.
In mental and substance use care, clinicians’ departures from evidence-based practice guidelines have been well documented for conditions as varied as attention deficit hyperactivity disorder (ADHD) (3) , anxiety disorders (4) , and conduct disorders in children (5) ; comorbid mental and substance use illnesses (6) and depression in adults (7) and children (8) ; and opioid dependence (9) , use of illicit drugs (10) , schizophrenia (11) , and alcohol dependence (12) . Furthermore, many individuals who need treatment receive none (13 – 15) . Although reports show improved access to care for people with the most severe mental illnesses, they also show declining access for those with less severe mental illnesses (14) and ethnic minorities (13) . In addition, racial and ethnic minorities have also been demonstrated to receive lower quality of care (16) . These documented disparities are especially of concern given that evidence-based practices, when adjusted to the needs of minority populations, have been shown to result in as good or better quality improvements and outcomes (17 , 18) . Also worrisome, less is known about errors in or injuries due to mental and substance use treatment than is known about general health care (19 , 20) .
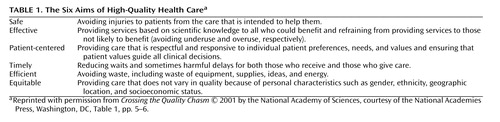
The original quality chasm report concluded that a fundamental redesign of the health care system is required and proposed a framework for fixing the system based on six aims for high-quality health care ( Table 1 ) and 10 rules to guide redesign ( Table 2 ). Six critical pathways were identified for achieving the prescribed aims and rules: 1) adopting new ways of delivering care; 2) effectively using information technology; 3) managing the clinical knowledge, skills, and deployment of the workforce; 4) building effective teams and coordination of care across patient conditions, services, and settings; 5) improving how quality is measured; and 6) using payment methods conducive to good quality.

In analyzing the applicability of this framework to mental and substance use health care, the Committee found the quality chasm recommendations for redesign to be as applicable to mental and substance use health care as they are to general health care but requiring some adaptation to reflect the characteristics that distinguish mental and substance use from general health care. These characteristics include greater obstacles to patient-centered care, a weaker quality measurement and improvement infrastructure, more separate care-delivery arrangements, less use of information technology, a more diverse workforce with greater use of solo practice, and a differently structured marketplace. Improving the Quality of Health Care for Mental and Substance Use Conditions offers a multifaceted and comprehensive strategy that specifies actions that clinicians, health care organizations, purchasers, health plans, educational institutions, federal and state legislators, executive agencies, and others should take to improve quality.
What Should Psychiatrists and Psychiatric Organizations Do to Improve the Quality of Mental and Substance Use Care in Daily Practice?
Pursue Patient-Centered Care
The original quality chasm report calls for “patient-centered” care (i.e., care in which patient preferences, needs, and values guide all clinical decision making; patient needs are anticipated; knowledge and information are shared freely; and care is transparent to the patient). Within a shared decision-making model, patients, as the “source of control,” should be able to exercise the degree of control they choose over health care decisions that affect them.
However, mental and substance use health care consumers face obstacles to serving as the source of control that generally are not encountered by consumers of general health care. The capacity of individuals with mental and substance use conditions to make decisions on their own behalf is often underestimated by clinicians and not supported by the health care system, especially when patients are coerced into treatment (as are the majority of individuals receiving treatment for substance use). Although a minority of mental and substance use patients, like patients with general health conditions, have some degree of impaired decision making, the adverse effect of stigma on mental and substance use patients’ ability to exercise their capacity for decision making can seriously impede their ability to manage their illnesses and achieve recovery.
Clinicians and organizations providing mental and substance use health care can promote patient-centered care by 1) endorsing and supporting decision making by mental and substance use health care consumers as the default policy in their practices, 2) providing decision-making support to all such patients, including those coerced into care, and 3) supporting illness self-management practices for all consumers and formal self-management programs for individuals with chronic illnesses. Organizations delivering care additionally should involve mental and substance use health care consumers in the design, administration, and delivery of organization services.
Endorsing and supporting patient decision making means assuming each patient’s right to make treatment decisions unless there is evidence of danger to the patient or others or the patient has been determined to be incompetent to make decisions. However, patient-centered decision making is also part of shared clinician-patient decision making; it does not mean that professionals must agree with all of the patient’s decisions.
The original quality chasm report notes that among all consumers, there can sometimes be a tension between providing patient-centered care and providing effective (evidence-based) care. This tension was addressed in the committee’s analysis as well. The committee noted that patients may express a preference for treatment that lacks an evidence base (e.g., psychodynamic psychotherapy for obsessive-compulsive disorder) when other, evidence-based treatments exist (e.g., medications and cognitive behavior therapy). For clinicians to adhere in such cases to an approach grounded in empirical research may leave them at odds with patients who desire an intervention that they believe will better meet their needs. In such instances, resolution may be obtained only over time, as the patient and clinician work together to reconcile competing and conflicting aims through shared decision making.
When patients, such as individuals with severe mental illnesses, propose a course of action that the clinician believes to be misguided, the clinician needs to support the patient through disagreements about treatment decisions, asking about the patient’s goals for recovery, and factoring these into treatment decisions and recovery plans. Patient education can play a critical role in this process, as clinicians provide information about the benefits and risks of different treatment options. Supporting consumer decision making also means offering consumers a choice of treatments and providers; assistance in making choices; and, for individuals with significantly impaired cognition or diminished self-efficacy beliefs, compensatory mechanisms such as peer support programs and advance directives. Duke University’s Program on Advance Psychiatric Directives provides toolkits and user-friendly instructions for consumers, clinicians, and family members to use in completing psychiatric advance directives (21) .
Illness self-management encompasses the day-to-day tasks an individual carries out to live successfully with chronic illness(es) and requires such skills as monitoring symptoms, using medications appropriately, practicing behaviors conducive to good health (e.g., in nutrition, sleep, and exercise), employing stress-reduction practices and managing negative emotions, using community resources appropriately, communicating effectively with health care providers, and practicing health-related problem solving and decision making (2) . Illness self-management programs for a variety of chronic illnesses, including heart disease, lung disease, stroke, and arthritis, have reduced disability, decreased needed visits to physicians and emergency rooms, and increased self-reported energy and health. Components of illness self-management for individuals with chronic mental illnesses include psychoeducation, behavioral practices to support taking medications appropriately, relapse prevention, and teaching coping skills and actions to alleviate symptoms. Stanford University has validated a standardized approach for illness self-management (described at http://patienteducation.stanford.edu/programs/cdsmp.html) (22) .
Help Strengthen the Quality Measurement and Improvement Infrastructure
The infrastructure needed to measure, analyze, publicly report, and improve the quality of mental and substance use health care is less well developed than that for general health care. Strengthening this infrastructure requires 1) a more coordinated strategy for filling gaps in the evidence base, 2) better dissemination of evidence to clinicians, 3) improved diagnostic and assessment strategies, 4) a stronger infrastructure for measuring and reporting quality, and 5) support for quality improvement practices at the locus of care.
Although the majority of the report’s recommendations for building this infrastructure call for action by the U.S. Department of Health and Human Services, funders of research, and other organizations, the report identifies two key roles that individual clinicians and provider organizations need to play: 1) increasing their use of valid and reliable questionnaires or other patient-assessment instruments to assess outcomes of treatment and help build the evidence base on effective treatments and 2) using measures of processes and outcomes of care to continuously improve the quality of the care.
In general health care, patients are increasingly recognized as valid judges of the quality of care they receive. Patient questionnaires about the extent to which symptoms are reduced as a result of treatment are already being used to measure outcomes for treatment of conditions such as benign prostatic hypertrophy and cataracts. These questionnaires yield accurate and reliable information on changes in symptoms and detailed and sensitive measures of treatment effectiveness (23) . The committee recommended that outcomes of mental and substance use health care be similarly measured. In addition to reporting on experiences with care delivery, such as the extent to which they were able to participate in treatment and other care decisions and gain skill in self-management of their illness, consumers can provide information on the effectiveness of treatment in reducing symptoms and improving functioning.
Several clinically feasible, valid, and reliable questionnaires, such as the Behavior and Symptom Identification Scale (24) , the Patient Health Questionnaire (25) , and the Addiction Severity Index (26 , 27) , can measure patient reports of symptoms and functioning. Alternatively, clinicians can assess response to treatment by obtaining information from the patient, combined with other data, and following up over time by using such instruments as the Global Assessment of Functioning (GAF) scale. The Veterans Health Administration requires all mental health inpatients to be rated at discharge using the GAF scale and all outpatients to be similarly rated at least once every 90 days during active treatment (28) .
Successful quality improvement also requires that such measurement be linked with day-to-day activities at the locus of care. Five practices are essential to successfully undertaking and sustaining improvements in quality: 1) ongoing communication about the desired change with those who are to affect it, 2) training in the new practice, 3) worker involvement in designing the change process, 4) sustained attention to progress in making the change, and 5) use of mechanisms for measurement, feedback, and redesign. These practices are found in leading health care quality improvement initiatives, such as those of the Institute for Health Care Improvement (http://www.ihi.org/ihi/programs). They also have been employed by some of the smallest and least resource-rich health care providers—providers of substance use treatment services—through the Network for the Improvement of Addiction Treatment (http://www.niatx.org). Individual clinicians not already experienced in quality improvement techniques must take steps to become educated in these and incorporate them into their daily practice.
Use Effective Linkage Mechanisms
Despite high rates (15%–60%) of co-occurrence of mental and substance use conditions (29 – 31) with multiple general health care conditions (32) , mental and substance use health services remain typically separated from each other and from general health care. These disconnected care delivery arrangements require multiple provider “handoffs” of patients for different services and the transmission of information to and joint planning by all of these providers, organizations, and agencies. The situation is exacerbated by the special legal and organizational prohibitions related to sharing mental and substance use information across providers. The Institute of Medicine calls on clinicians to routinely use four practices to bridge the separations between providers: screening, anticipating comorbidity and preplanning the clinical responses to it, establishing clinically effective linkages with other providers treating the patient, and routinely sharing information.
Effective screening can be performed by using a number of available and reliable instruments, such as the Patient Health Questionnaire, a self-administered instrument for screening for depression, anxiety disorders, alcohol abuse, and somatoform and eating disorders (33) . The National Institute on Alcohol Abuse and Alcoholism also has developed a single-question screener (one for men, one for women) for detecting alcohol problems in primary care and other settings (34) .
Because co-occurring disorders are expected in substance use and mental health treatment systems, the report recommends that whenever a patient is seen with a mental or substance use condition, the clinician should automatically screen for the other. Clinicians also should preplan their responses, i.e., treatment or referral, and whenever referral is planned, formal prearrangements with referral providers should be established. These arrangements should consist of clinically effective linkages with other treating providers; referral by itself is not an effective coordination mechanism. The committee noted special concerns regarding linkages between mental and substance use providers and general medical providers going in both directions, i.e., individuals with mental health and substance use problems who are seen in general medical settings and individuals with severe mental illnesses and substance abuse seen in specialty behavioral health settings who also have significant general medical conditions (35 – 37) . A continuum of four evidence-based coordination mechanisms are promoted, ranging from 1) formal (i.e., written) agreements among mental, substance use, and primary health care providers (less effective) to 2) case management of mental, substance use, and primary health care to 3) co-location of mental, substance-use, and primary health services and then to 4) delivery of mental, substance use, and primary health care through clinically integrated practices of primary and mental and substance use care providers (most effective). Shared electronic health records are also identified as an effective tool for care coordination.
Clinically effective linkages also require routine sharing (with patient knowledge and consent) of information on patients’ problems and treatments among providers treating the patient. Committee members identified this as another issue that brings conflicting ethical and clinical imperatives into play. Identifiable information about mental health and substance abuse treatment may be particularly sensitive, in part because of the lingering stigma of these disorders. Health care systems that fail to offer patients an adequate level of privacy protection may discourage them from seeking care or being open about the problems that have brought them to treatment. However, failure to share patient-specific information across providers (e.g., allowing a patient’s primary care physician to remain unaware that the patient is depressed and is receiving antidepressant medication) promotes uncoordinated and sometimes unsafe care.
The committee recognized that there is no ideal solution to this dilemma. In a patient-centered system, patients should be offered the maximum possible level of control over their health information. However, patients who are aware of the advantages of sharing at least some of their data are likely to opt for such an approach, particularly if effective technological protections for privacy are developed. Educating patients about these issues thus becomes a key strategy in promoting an optimal balance between privacy and efficient sharing of information.
Although the Health Insurance Portability and Accountability Act’s (HIPAA)’s regulations generally permit health care organizations to release—without requiring patient consent—individually identifiable information (except psychotherapy notes) about the patient to another provider or organization for treatment purposes, the same regulations do not supersede any contrary provisions of state laws, many of which are more stringent than the HIPAA requirements. HIPAA regulations also permit health care organizations to implement their own more stringent privacy protections. Moreover, separate federal laws govern release of information pertaining to treatment received in specialty drug or alcohol use treatment programs that receive federal funding—which are also superseded by any more stringent state laws. The Institute of Medicine report calls attention to this issue as one that requires review and possible change in public policy, one that leaders in the mental and substance use should champion. Organizations that impose constraints on information sharing beyond those imposed by federal or state laws also should examine them for any unintended adverse consequences on care coordination and make appropriate changes.
What Specific Policy Changes Should Psychiatrists, Psychiatric Organizations, and Other Leaders in Mental and Substance Use Care Advocate for to Help Psychiatry Cross the Quality Chasm?
Become Involved in Building the National Health Information Infrastructure
Major public and private sector collaborations are underway to develop the critical components of a National Health Information Infrastructure: 1) electronic health record systems with decision support for clinicians, 2) a secure platform for exchanging patient information across health care settings, and 3) data standards so that shared information will be understandable to all users. However, mental and substance use health care is not well addressed by National Health Information Infrastructure initiatives. Of the nearly 600 applications for awards by the Agency for Health Care Research and Quality in 2004 to promote the use of health information technology, only a handful had any substantive behavioral health component. Of 103 grants awarded, only one specifically targeted mental and substance use health care (2) . Mental and substance use health care also lags behind in its use of electronic health record systems and other forms of health information technology.
The report calls on the federal government (i.e., the Department of Health and Human Services and the Veterans Health Administration) to charge the national coordinator of health information technology and the Substance Abuse and Mental Health Services Administration with ensuring that the National Health Information Infrastructure addresses mental and substance use health care as fully as general health care and that public and private-sector mental and substance use health care stakeholders are integrated into these efforts. Individual clinicians and organizational leaders in mental and substance use health care should urge these federal agencies to do so and also should become involved in the major national committees and initiatives developing the National Health Information Infrastructure.
Advocate Sustained Workforce Development and Organize Unconnected Small Practices to Promote Innovation
Sustained national attention—in contrast to the many short-lived initiatives created and abandoned over the past decades—is needed to strengthen the quality and capacity of the mental and substance use workforce. The report recommends that an ongoing, federally funded, public-private council on the mental and substance use health care workforce, analogous to the Council on Graduate Medical Education and the National Advisory Council on Nurse Education and Practice, be created to develop and implement a comprehensive plan for workforce development. The committee envisions that educational organizations and training institutions would collaborate with this council, as would licensing/accrediting bodies, purchasers, and other private-sector initiatives. This public-private partnership would 1) identify specific competencies that all mental and substance use professionals must possess to be licensed or certified and 2) develop national standards for the credentialing and licensure of mental and substance use providers to eliminate differences in the standards now used by the states. The federal government would also support faculty development in mental and substance use health care in health profession schools, such as nursing and medicine, and schools and programs that educate mental and substance use specialist professionals, such as psychologists. Clinicians and organizational providers and their national organizations should advocate the creation of this council.
The report also calls attention to the high prevalence of unconnected solo practices among mental and substance use providers, which can impede uptake of information technology, evidence-based practices, and other advances in care. Practice size is a key determinant of information technology adoption for five clinical functions: obtaining treatment guidelines, exchanging clinical data with other physicians, accessing patient notes, generating treatment reminders, and writing prescriptions. Knowledge uptake similarly requires additional resources for the timely identification of scientific advances and innovations. In a study of the adoption of clinical practice guidelines for the treatment of ADHD, solo practice was associated with a reduced likelihood of adopting the guidelines (3) .
Some have seen these workforce recommendations (coming from a committee largely populated by individuals affiliated with large health systems) as calling for an end to the “cottage industry” of solo practice. Whether one agrees with the recommendations or not, society is clearly placing greater expectations for performance and accountability on all providers. Organizations assimilate innovations more readily if they are large, mature, divided into semiautonomous units, have flexible resources to channel into new projects, and have decentralized decision-making structures (38) . Larger groups also are theorized to have readier access to capital and administrative support staff and the ability to spread acquisition and implementation costs among more providers (39) . Solo or smaller practices may need to trade off some autonomy and band together to marshal resources and achieve some of the functionalities of larger organizations in order to meet these expanding expectations (40) .
Advocate With Purchasers and Policy Makers
The mental and substance use health care marketplace is distinguished by the dominance of government purchasers, use of “carve-out” insurance arrangements, the tendency of private insurance to avoid covering persons with mental and substance use illnesses, and government purchasers’ greater use of direct provision and purchase of care rather than insurance arrangements (41) .
The report makes a number of recommendations targeted to these purchasers and their purchasing practices. It also speaks to the ongoing need to achieve better coverage of mental and substance use health care in public- and private-sector insurance plans. The dominance of public purchasers makes purchasing processes more transparent and open to public discussion. Leaders in psychiatry should continue to advocate equal coverage of mental and substance use treatments and for purchasers to take steps to reorient procurement processes to give greater weight to the quality of care in selecting vendors.
Finding a Balance
In drafting its recommendations, the committee recognized and sought to find a balance in multiple areas of controversy. We have noted and discussed a number of these issues earlier in our article: What happens when patients wish to obtain treatments for which efficacy is not established or refuse recommended care? How do you balance privacy and consumer control over their health information with the need for coordinating the efforts of multiple providers? Does the greater capacity of larger organizations to implement quality improvement strategies signal an end to solo practice?
Perhaps the deepest controversy of all is the degree to which mental health and substance use can or should be integrated into the rest of medicine. This is evident not only in terms of recommendations regarding collaboration between mental health and other providers but in the very rationale for the report itself. Should not the original quality chasm report have applied to mental health and substance use conditions as it does to all other illnesses such as diabetes and heart disease? The committee concluded that quality improvement strategies adopted for general health care are indeed applicable to mental health and substance use conditions. However, several features of the mental and substance use system, such as stigma, separation from the rest of health care, and complexity of the mental health workforce, made it important to adapt those recommendations and justified the need for a separate report. More profound and more controversial is the question of whether the mental and substance use field is truly ready and willing to engage the overall health care field in an integrated way. Psychiatrists, along with other mental health advocates, have long espoused the biopsychosocial model and decried being carved out in insurance plans. At the same time, there often is a parallel fear of engulfment and loss of autonomy, usually accompanied by an insularity of the field. From a clinical perspective, the committee felt that one cannot espouse “treating the whole person” without treating the whole person . As such, it came to a fundamental conclusion that coordination and collaboration with the rest of medicine are essential (and vice versa), but it is also critical to ensure access to the depth and expertise provided by psychiatrists and other mental health and substance use specialists.
In sum, improving mental and substance use health care will be most readily achieved through the efforts of participants at all levels of the health care system. However, the Institute of Medicine report identifies actions that each party involved in delivering mental and substance use health care—clinicians, health care organizations, purchasers, health plans, educational institutions, federal and state governments—can take now to achieve significant improvements in care.
1. Institute of Medicine Committee on Quality of Health in America: Crossing the Quality Chasm: A New Health System for the 21st Century: 1–337. Washington, DC, National Academies Press Report, 2001Google Scholar
2. Institute of Medicine Committee on Quality of Health in America: Improving the Quality of Health Care for Mental and Substance Use Conditions: 77–139. Washington, DC, National Academies Press Report, 2006Google Scholar
3. Rushton JL, Fant K, Clark SJ: Use of practice guidelines in the primary care of children with attention-deficit hyperactivity disorder. Pediatrics 2004; 114:e23–e28Google Scholar
4. Stein MB, Sherbourne CD, Craske MG, Means-Christensen A, Bystritsky A, Katon W, Sullivan G, Roy-Byrne P: Quality of care for primary care patients with anxiety disorders. Am J Psychiatry 2004; 161:2230–2237Google Scholar
5. Zima BT, Hurlbert MS, Knapp P, Ladd H, Tang L, Duan N, Wallace P, Rosenblatt A, Landsverk J, Wells KB: Quality of publicly-funded outpatient specialty mental health care for common childhood psychiatric disorders in California. J Am Acad Child Adolesc Psychiatry 2005; 44:130–144Google Scholar
6. Watkins K, Burnam A, Kung F, Paddock SM: A national survey of care for persons with co-occurring mental and substance use disorders. Psychiatr Serv 2001; 52:1062–1068Google Scholar
7. Simon GE, Von Korff M, Rutter C, Peterson DA: Treatment process and outcomes for managed care patients receiving new antidepressant prescriptions from psychiatrists and primary care physicians. Arch Gen Psychiatry 2001; 58:395–401Google Scholar
8. Richardson L, Di Guiseppe D, Christakis DA, McCauley E, Katon W: Quality of care for Medicaid-covered youth treated with antidepressant therapy. Arch Gen Psychiatry 2004; 61:475–480Google Scholar
9. D’Aunno T, Pollack HA: Changes in methadone treatment practices: results from a national panel study. JAMA 2002; 288:850–856Google Scholar
10. Friedman PD, McCullough D, Saitz R: Screening and intervention for illicit drug abuse: a national survey of primary care physicians and psychiatrists. Arch Int Med 2001; 161:248–251Google Scholar
11. Buchanan RW, Kreyenbuhl J, Zito JM, Lehman AF: The schizophrenia PORT pharmacological treatment recommendations: conformance and implications for symptoms and functional outcome. Schizophr Bull 2002; 28:63–73Google Scholar
12. McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, Kerr EA: The quality of health care delivered to adults in the United States. N Engl J Med 2003; 348:2635–2645Google Scholar
13. Kessler RC, Demler O, Frank RG, Olfson M, Pincus HA, Walters EE, Wang P, Wells KB, Zaslavsky AM: Prevalence and treatment of mental disorders: 1990 to 2003. N Engl J Med 2005; 352:2515–2523Google Scholar
14. Mechanic D, Bilder S: Treatment of people with mental illness: a decade-long perspective. Health Aff 2004; 23:84–95Google Scholar
15. Substance Abuse and Mental Health Services Administration: Results from the 2003 National Survey on Drug Use and Health: national findings, NSDUH Series H-25. Rockville, Md, Substance Abuse and Mental Health Services Administration, 2004Google Scholar
16. US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration and Center for Mental Health Services: Mental Health: Culture, Race, and Ethnicity: A Supplement to Mental Health: A Report of the Surgeon General, 1–217. Rockville, Md, US Department of Health and Human Services Report, 2001Google Scholar
17. Wells KB, Miranda J, Bauer M, Bruce ML, Durham ML, Escobar J, Ford DE, Gonzales JJ, Hoagwood K, Horowitz S, Lawson W, Lewis L, McGuire TG, Pincus HA, Scheffler RM: Overcoming barriers to reducing the burden of affective disorders. Biol Psychiatry 2002; 52:655–675Google Scholar
18. Miranda J, Duan N, Sherbourne CD, Schoenbaum M, Lagomasino I, Jackson-Triche M, Wells KB: Improving care for minorities: can quality improvement interventions improve care and outcomes for depressed minorities? results of a randomized, controlled trial. Health Serv Res 2003; 38:613–630Google Scholar
19. Bates DW, Shore MF, Gibson R, Bosk C: Examining the evidence. Psychiatr Serv 2003; 54:1–5Google Scholar
20. Moos RH: Iatrogenic effects of psychosocial interventions for substance use disorders: prevalence, predictors, prevention. Addiction 2005; 100:595–604Google Scholar
21. Duke University Program on Advance Psychiatric Directives. Durham, NC, Duke University, 2006 electronic citationGoogle Scholar
22. Lorig KR, Hurwitz EL, Sobel D, Hobbs M, Ritter P: A national dissemination of an evidence-based self-management program: a process evaluation study. Patient Educ Couns 2005; 59:69–79Google Scholar
23. Stanton M: Expanding Patient-Centered Care to Empower Patients and Assist Providers: 02–0024. Rockville, Md, AHRQ Report, 2002Google Scholar
24. Eisen SV, Normand SL, Belanger AJ, Spiro A III, Esch D: The Revised Behavior and Symptom Identification Scale (BASIS-R): reliability and validity. Med Care 2004; 42:1230–1241Google Scholar
25. Lowe B, Unutzer J, Callahan CM, Perkins A, Kroenke K: Monitoring depression treatment outcomes with the Patient Health Questionnaire–9. Med Care 2004; 42:1194–1201Google Scholar
26. Butler SF, Budman SH, Goldman RJ, Newman FL, Beckley KE, Trottier D, Cacciola JS: Initial validation of a computer-administered addiction severity index: the ASI-MV. Psychol Addict Behav 2001; 15:4–12Google Scholar
27. McLellan AT, Luborsky L, Woody GE, O’Brien CP: An improved diagnostic evaluation instrument for substance abuse patients: the Addiction Severity Index. J Nerv Ment Dis 1980; 168:26–33Google Scholar
28. Greensberg G, Rosenheck R: Department of Veterans Affairs National Mental Health Program Performance Monitoring System: Fiscal Year 2004 Report 182. West Haven, Conn, Northeast Program Evaluation Center Report, 2005Google Scholar
29. Kessler RC, Nelson CB, McGonagle KA, Edlund MJ, Frank RG, Leaf PJ: The epidemiology of co-occurring addictive and mental disorders: implications for prevention and service utilization. Am J Orthopsychiatry 1996; 66:17–31Google Scholar
30. Grant BF, Stinson FS, Dawson DA, Chou SP, Dufour MC, Compton W, Pickering RP, Kaplan K: Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 2004; 61:807–816Google Scholar
31. Grant BF, Stinson FS, Dawson DA, Chou SP, Ruan WJ, Pickering RP: Co-occurrence of 12-month alcohol and drug use disorders and personality disorders in the United States: results from the National Epidemiology Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 2004; 61:361–368Google Scholar
32. Horvitz-Lennon M, Kilbourne A, Pincus HA: From silos to bridges: meeting the general health care needs of adults with severe mental illnesses. Health Aff 2006; 25:659–670Google Scholar
33. Spitzer RL, Kroenke K, Williams JB: Validation and utility of a self-report version of PRIME-MD. JAMA 1999; 282:1737–1744Google Scholar
34. National Institute on Alcohol Abuse and Alcoholism, US Department of Health and Human Services, National Institutes of Health: Helping Patients Who Drink Too Much: A Clinician’s Guide, 2005. http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicGoogle Scholar
35. Horvitz-Lennon M, Kilbourne A, Pincus HA: From silos to bridges: meeting the general health care needs of adults with severe mental illnesses. Health Aff 2006; 25:659–670Google Scholar
36. Pincus HA: The future of behavioral health and primary care: drowning in the mainstream or left on the bank? Psychosomatics 2003; 44:1–11Google Scholar
37. Druss BG, von Esenwein SA: Improving general medical care for persons with mental and addictive disorders: a systematic review. Gen Hosp Psychiatry 2006; 28:145–153Google Scholar
38. Greenhalgh T, Robert G, MacFarlane F, Bate P, Kyriakidou O: Diffusion of innovations in service organizations: systemic review and recommendations. Milbank Q 2004; 82:581–629Google Scholar
39. Reed MC, Grossman JM: Limited Information Technology for Patient Care in Physician Offices. Washington, DC, Center for Studying Health System Change, 2004Google Scholar
40. Berwick DM: Disseminating innovations in health care. JAMA 2003; 289:1969–1975Google Scholar
41. Pincus H, Hough L, Knox Houtsinger J, Rollman B, Frank RG: Emerging models of depression care: multi-level (“6 P”) strategies. Int J Methods Psychiatr Res 2003; 12:54–63Google Scholar

