
Adolescent Suicidal Ideation as Predictive of Psychopathology, Suicidal Behavior, and Compromised Functioning at Age 30
Abstract
Objective: The purpose of this study was to examine whether suicidal ideation in a community population of adolescents represents normative adolescent angst or is predictive of psychopathology, suicidal and problem behaviors, and compromised functioning 15 years after onset. Method: Participants were 346 largely Caucasian individuals who were part of a single-age cohort from a working class community and whose development had been traced prospectively from ages 5 to 30. Those with suicidal ideation at age 15 were compared to those without suicidal ideation at age 15 on measures of psychopathology, suicidal ideation and behavior, problem behaviors, and adult functioning at age 30. Gender differences were assessed across all domains. Results: At age 30, there were marked differences between adolescents with suicidal ideation and adolescents without suicidal ideation of both genders in most domains examined. Subjects with suicidal ideation were twice as likely to have an axis I disorder, nearly 12 times more likely to have attempted suicide by age 30, and 15 times more likely to have expressed suicidal thoughts in the past 4 years. Subjects with suicidal ideation had more problem behaviors and poorer overall functioning as assessed by multiple informants. Their self-perceptions of coping ability, self-esteem, and interpersonal relations were also lower. Although subjects with suicidal ideation among both genders had higher levels of psychopathology, suicidal ideation and behavior, and problem behaviors at age 30, male subjects with suicidal ideation had lower salaries and socioeconomic status and were less likely to have achieved residential independence. Conclusions: Findings underscore the importance of considering suicidal ideation in adolescence as a marker of severe distress and a predictor of compromised functioning, indicating the need for early identification and continued intervention.
The importance of suicidal ideation, particularly in adolescence, and its relationship to psychiatric morbidity and completed suicide continue to be a subject of debate (1 – 7) . A number of recent studies, however, found that suicidal ideation was both associated with and predictive of psychopathology, especially mood, anxiety, and substance use disorders, among adolescents as well as older age groups (5 , 8–11) . Furthermore, adolescent suicidal ideation has been linked to deficits in behavioral and emotional functioning (e.g., low self-esteem, depressive symptoms) in adolescence, extending into young adulthood (1 , 3 , 4) .
We examined the association of suicidal ideation in a community population of 15-year-old adolescents with their subsequent psychopathology and suicidal ideation, problem behaviors, and compromised functioning at age 30, a critical period for career development and entrance into marriage and parenthood (12 – 14) . Our study focuses on suicidal ideation as a key marker of distress in adolescence and its link to compromised functioning and psychiatric illness during a pivotal period of adulthood. Covering a 15-year span, our study is one of the longest investigations of this area of major clinical concern and provides important implications for assessment and treatment.
Interest in all aspects of adolescent suicidal behavior is prompted because of the potential lethality of the behavior as well as rising rates of completed suicide in adolescent populations (15) . The seriousness of suicidal ideation as a symptom and indicator of psychiatric illness (1) and a marker of distress and poor functioning (11) has been confirmed by findings from several studies. Ahrens and colleagues (1) , Goldney and colleagues (3) , and Groleger and colleagues (4) found that deficits in emotional and behavioral functioning were associated with suicidal ideation in both adolescents and adults. Because of the role of suicidal ideation in the etiology of completed suicide, psychopathology, and poor functioning, it has been included as a focus of prevention and intervention initiatives at both clinical and community levels (16 , 17) . Still, there have been different views regarding the seriousness and consequences of adolescent ideation. Beliefs that ideation in adolescence and young adulthood is normative (6 , 18) are contrasted with findings from recent studies demonstrating associations between adolescent suicidal ideation and suicidal ideation and suicide attempts in young adulthood, in both community and clinical cohorts (5 , 10) .
Prior research has revealed marked gender differences in adolescent suicidal ideation and behavior. While female subjects outnumber male subjects in most community studies of suicidal ideation and attempts (4 , 11 , 19) , some studies have reported that adolescent boys are overrepresented in studies of completed suicide (20) . Moreover, findings from recent studies have indicated that there may be gender-specific patterns of early risk factors and/or developmental pathways associated with suicidal ideation and behavior in adolescence and young adulthood. For example, hopelessness, dependence, and poor social/emotional adjustment have been identified as early precursors for later ideation in boys, while family discord, early behavioral problems, and poor perception of family roles have been identified as risk factors for girls (11 , 21) . Therefore, gender is an important consideration in studies of suicidal ideation and behavior.
In spite of clinical concern and research interest, there have been few prospective studies of the relationship between suicidal ideation in adolescence and later developmental outcomes in adulthood. In our study, we evaluated the long-term effect of adolescent ideation by prospectively following a community sample of adolescents who expressed suicidal ideation at age 15, using multiple measures to assess their levels of psychopathology, suicidal ideation and behavior, problem behaviors, and adult functioning. Comparing outcomes at age 30 for those subjects who expressed suicidal ideation at age 15 and those who did not will help determine whether adolescent suicidal ideation is indeed a marker of severe distress and a predictor of adult psychopathology and poor functioning (22) or merely a manifestation of adolescent angst, in which associated difficulties fade over time (2) . The four objectives of our study are as follows: 1) to examine the link between ideation at age 15 and the presence of psychopathology and suicidal ideation and behavior at age 30, 2) to assess the relationship between suicidal ideation at age 15 and problem behaviors at age 30, 3) to determine the long-term association between ideation at age 15 and later adult functioning, and 4) to assess gender differences in these relationships.
Method
Participants were drawn from a prospective, longitudinal study that traced the adaptation and mental health of a single-age community cohort from childhood, age 5 (1977), to adulthood, age 30 (2002). The composition of the original study group (N=763) reflected the community from which they were drawn. Nearly all participants were Caucasian (99.0%), and two-thirds of the households were working or lower-middle class. Between 1977 and 2002, attrition occurred primarily following kindergarten, when a group of respondents (N=359) transferred from the public school system to private and parochial schools and were purposely excluded from follow-up, since data collection occurred in the public schools (23) . The group of participants who were retained at age 30 did not differ significantly from the group that was not on variables known to be associated with psychiatric illness, such as gender (χ 2 =1.53, df=1, p=0.22), parental socioeconomic status (χ 2 =1.96, df=1, p=0.22), nurse-rated child health (t=0.43, df=700, p=0.70), and maternal-rated anxious/depressed child behavior (t=1.15, df=725, p=0.25). These results strongly suggest that the retained subject group was not compromised by selective attrition.
In 1987, when adolescent suicidal ideation was assessed and most participants were 15 years old and in the ninth grade, complete data on suicidal ideation were collected for 378 respondents (185 boys and 193 girls). At age 15, subjects with suicidal ideation significantly differed from subjects without suicidal ideation. The subjects with suicidal ideation self-reported more problem behaviors (t=–8.26, df=340, p<0.0001). Greater problem behaviors in subjects with suicidal ideation relative to those without were also reported by teachers (t=–4.37, df=336, p<0.0001) and parents (t= –3.85, df=336, p<0.0001). In addition, subjects with suicidal ideation reported more depressive symptoms (t=–10.45, df=338, p<0.0001), higher levels of peer problems (t=7.36, df=338, p<0.0001), and lower family cohesion (t=2.80, df=228, p=0.005). There were no differences in parental socioeconomic status.
In 2002, when psychopathology, suicidal ideation and behavior, problem behaviors, and adult functioning were assessed, 377 respondents were interviewed at a mean age of 30. Participant retention from age 15 to 30 was high (93%). Analyses indicated that those who were retained in the age-30 study group did not differ from those who were not on measures of problem behaviors in self-, teacher, or parental reports; family socioeconomic status; or depressive symptoms.
Study Participants
The final subject group selected for our study was composed of participants for whom complete data were available on ideation at both age 15 and age 30 (N=346) (male subjects: 166, female subjects: 180). At age 30, the characteristics of the selected study group reflected qualities of the total cohort: 98% were Caucasian; 96% were either employed full-time or were stay-at-home parents; 39% had completed college; 43% were currently married; and 36% had made the transition to parenthood. Representative of the age-30 study group, a majority (74.9%) fell into categories 2 and 3 of the Hollingshead Socioeconomic Status Scale (24) , indicating middle-class status. After a complete description of the study at each time point, written informed consent was obtained from all participants.
Measures
Suicidal ideation at age 15
Subjects who gave a positive response to an item on the Youth Self-Report (25) (i.e., an answer of “somewhat” or “very true” to the statement, “I think about killing myself”) and/or a positive response to an item from the Children’s Depression Inventory (26) (i.e., an answer of “yes” to the statement, “I think about killing myself but would not do it” or “I want to kill myself”) were classified as having suicidal ideation at age 15 (N=76; 22%). Categorizing adolescents with suicidal ideation using multiple items is consistent with the methodology of previous community studies (27) and has been utilized in past analyses of this study group (11) .
Age 30 measures
Psychopathology, problem behaviors, and poor functioning were the measures chosen to assess salient domains of young adult functioning and have all been shown to negatively affect individuals during young adulthood, when relationships are established, families are started, and careers are solidified (13 , 28 , 29) .
Psychopathology and suicidal behavior
DSM-IV disorders (mood, anxiety, and substance), suicidal ideation, and lifetime suicide attempts were assessed using the National Institute of Mental Health Diagnostic Interview Schedule, Version IV (30) . Mood disorders examined were depression, dysthymia, and bipolar diagnoses; anxiety disorders included social and specific phobia, posttraumatic stress disorder, panic disorder, and generalized anxiety disorder; and substance disorders included alcohol and drug disorders.
Suicidal ideation at age 30 was assessed with the item “Have you thought about committing suicide at any time in the past 4 years?” from the Major Depressive Disorder section of the National Institute of Mental Health Diagnostic Interview Schedule, Version IV. Suicide attempts from ages 15–30 were assessed using a combination of data collected through age 26 (at ages 15, 18, 21, and 26) that indexed lifetime suicide attempts, as well as an item asked at age 30, “Did you try to end your own life in the past 4 years?”
Problem behaviors
Problem behaviors at age 30 were determined using total problem scores from the Young Adult Self-Report and the Young Adult Behavior Checklist (31) . Both measures are designed to assess behavioral and emotional problems of young adults ages 18–30. The Young Adult Self-Report is a self-report measure, and the Young Adult Behavior Checklist is administered to a parent or an individual close to the respondent. At age 30, the Young Adult Behavior Checklist was completed by the parents or relatives (N=299) of the respondents.
Young adult functioning
The Global Assessment of Functioning Scale and the Social and Occupational Functioning Assessment Scale from axis V of DSM-IV were used to assess young adults’ overall functioning. The Global Assessment of Functioning Scale is a comprehensive rating that takes into account all levels of functioning, excluding the influence of environmental and/or physical limitations. The Social and Occupational Functioning Assessment Scale provides an assessment of social and occupational functioning independent of the severity of psychological symptoms. Both yield scores that range from 1 (poorest functioning) to 100 (highest functioning) and were administered by trained interviewers blind to previous diagnoses and earlier suicidal ideation.
Self-esteem was measured by the Rosenberg Self-Esteem Scale (32) , a 10-item scale designed to measure the self-acceptance aspect of self-esteem. Coping was measured by a version of the General Perceived Self-Efficacy Scale (33) , a 10-item scale used to assess respondents’ abilities to cope effectively with life stressors. The respondents’ interpersonal problems (such as difficulties communicating with others) were assessed using the Simmons Interpersonal Problems Scale, a study-developed measure. Finally, the respondents’ need for social support was evaluated by the “need for social support” subscale of the Arizona Social Support Interview Schedule (34) .
The respondents’ current occupational prestige and educational attainment were the two indices used to determine socioeconomic status (24) . Current yearly salary was assessed on a 9-point scale from 1 (less than $10,000/year) to 9 ($80,000 or more/year). In addition, life marker events representing traditional transitions to adulthood, such as college completion, residential independence, home ownership, marriage, and parenthood, were examined.
Statistical Analyses
Because previous studies indicate that suicidal ideation may be differentially associated with outcomes as a function of gender (11 , 21) , preliminary analyses were used to test for interactions between group (subjects with versus without suicidal ideation) and gender (male versus female subjects). Specifically, analysis of variance was used to test for interaction effects across continuous measures. The Breslow-Day chi-square test for homogeneity of odds ratios tested for interaction effects across discrete measures. Analyses that revealed no gender differences in the means or odds ratios were subsequently repeated, removing gender as a factor. All significance tests were two-tailed.
Results
Psychopathology and Suicidal Behavior
Both male and female adolescents with suicidal ideation had greater overall levels of psychopathology and suicidal ideation and attempts by age 30 compared to their peers without suicidal ideation. At age 30, subjects with suicidal ideation were significantly more likely to have met criteria for an axis I psychiatric disorder in the past year than subjects without suicidal ideation (26.7% versus 16.4%) ( Table 1 ). When subjects with and without adolescent suicidal ideation were compared on specific disorders at age 30, significant differences emerged for anxiety disorders; those with suicidal ideation were more likely (odds ratio=2.56, p<0.05) than those without to have experienced an anxiety disorder in the past year. No gender differences were found in the proportion of male and female subjects with suicidal ideation versus subjects without suicidal ideation who met criteria for any specific psychiatric disorder examined.
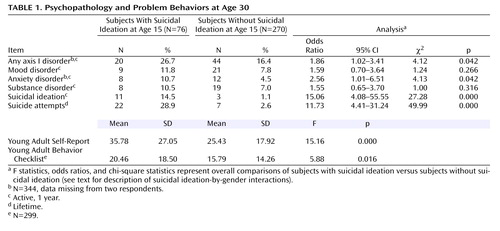
Large significant differences were found when subjects with and without adolescent suicidal ideation were compared on suicidal ideation and attempts at age 30. Adolescents with suicidal ideation were 15 times more likely (odds ratio=15.06, p<0.0001) to have expressed suicidal ideation in the past 4 years (from ages 26 to 30) and nearly 12 times more likely (odds ratio=11.73, p<0.0001) to have made at least one suicide attempt from ages 15 to 30 than adolescents without suicidal ideation. These associations did not vary by gender.
Problem Behaviors
Reports from multiple informants indicated that adolescents with suicidal ideation perceived themselves and were perceived by others as having more problems at age 30 than their peers without adolescent suicidal ideation. Subjects with suicidal ideation reported more problem behaviors at age 30 than subjects without adolescent suicidal ideation (F=5.16, df=1, 344, p<0.0001). The parents and relatives of subjects with suicidal ideation also reported significantly more problem behaviors than the parents and relatives of subjects without suicidal ideation (F=5.88, df=1, 344, p=0.02). Neither self-reports nor parent/relative reports yielded significant group-by-gender interactions, indicating that the associations between suicidal ideation and problem behaviors at age 30 were the same for both male and female subjects.
Young Adult Functioning
Across a wide variety of indicators, subjects with adolescent suicidal ideation reported significantly poorer functioning at age 30 than their peers without adolescent suicidal ideation ( Table 2 ). Interviewers rated subjects with suicidal ideation as having significantly lower levels of global functioning and social and occupational functioning than subjects without suicidal ideation. Self-reported coping and self-esteem were lower in subjects with suicidal ideation; interpersonal problems and reports of needing social support were higher for this group.

In our assessment of social class indicators and financial resources at age 30, we found that levels of socioeconomic status among subjects with adolescent suicidal ideation were lower than those of subjects without adolescent suicidal ideation. Tests for differences in the association between suicidal ideation and socioeconomic status by gender revealed differences for male and female subjects. A significant group-by-gender interaction (F=4.20, df=1, 318, p=0.04) indicated that male subjects with adolescent suicidal ideation had significantly lower socioeconomic status at age 30 than male subjects without adolescent suicidal ideation. There were no differences between the female subjects from both groups in socioeconomic status at age 30. Subjects with suicidal ideation also reported lower yearly salaries than subjects without suicidal ideation. A significant group-by-gender interaction (F=4.64, df=1, 303, p=0.03) revealed that male subjects with suicidal ideation reported significantly lower yearly salaries than male subjects without suicidal ideation, whereas there were no differences between the female subjects from both groups.
Contrary to expectation, the subjects with adolescent suicidal ideation were not significantly different from the subjects without adolescent suicidal ideation on several of the traditional markers of the transition to adulthood. By age 30, subjects with and without adolescent suicidal ideation were equally likely to have completed college and made transitions to marriage and parenthood. However, deficits in a number of areas of adult functioning were revealed, specifically for male subjects with suicidal ideation. While there were no overall differences in the proportions of subjects with suicidal ideation and subjects without suicidal ideation living with parents or reporting homeownership at age 30 ( Table 2 ), tests for interactions revealed discernible gender differences in these associations. Specifically, differences in the proportion of subjects with suicidal ideation and subjects without suicidal ideation who were living independently from their parents varied significantly by gender (χ 2 =7.47, df=1, p=0.006). Male subjects with suicidal ideation were significantly more likely (odds ratio=4.46, 95% confidence interval [CI]=1.55–12.88) to live with their parents at age 30 than male subjects without suicidal ideation (χ 2 =0.69, df=1, p=0.003), while there were no differences between the female subjects from both groups (χ 2 =0.59, df=1, p=0.44). There were significant differences in the proportion of male and female subjects with suicidal ideation who reported owning homes by age 30 (χ 2 =9.70, df=1, p=0.002). Although there were no significant differences between female subjects with suicidal ideation and female subjects without suicidal ideation in the proportion who reported being homeowners at age 30 (χ 2 =1.59, df=1, p=0.21), male subjects without suicidal ideation were nearly five times more likely (odds ratio=4.72, CI=1.54–14.53) than male subjects with suicidal ideation to be homeowners by age 30 (χ 2 =8.49, df=1, p=0.004).
Discussion
The findings of our study highlight the strong relationship between suicidal ideation at age 15 and higher rates of psychopathology, suicidal ideation and behavior, problem behaviors, and poor functioning 15 years later. These findings affirm previous studies (3 , 11) in which adolescent suicidal ideation was identified as a marker of strong emotional distress and associated with later impaired functioning.
Although less than 29% of subjects with suicidal ideation attempted suicide between ages 15 and 30, they were almost 12 times more likely to do so than subjects without suicidal ideation. In addition, these adolescents with suicidal ideation had a 15-fold greater likelihood of expressing suicidal ideation in the past 4 years than their peers. In addition, those who expressed suicidal ideation at age 15 were almost twice as likely as those without suicidal ideation to have an axis I disorder at age 30. When specific disorders were examined, subjects with suicidal ideation were two and one-half times more likely to have an anxiety disorder than their peers. Previous investigations have confirmed the relationship between suicidal ideation and anxiety in child, adolescent, and adult community populations (8 , 11 , 35 , 36) . Contrary to our expectation as well as to previous findings (5 , 9 , 37) , no statistically significant differences emerged between the subjects with suicidal ideation and subjects without suicidal ideation on 1-year rates of depression. This finding may be influenced by the small study group size or by the high lifetime and 1-year prevalence of depression in the overall study group at age 30 (lifetime=31%; 1 year=8%).
In numerous areas of normative adult functioning, subjects with suicidal ideation of both genders performed more poorly than subjects without suicidal ideation. They also reported higher levels of problem behaviors than subjects without suicidal ideation, and concomitantly were viewed as exhibiting more problem behaviors by other informants (mothers and relatives and interviewers). The subjects with suicidal ideation and their relatives reported higher problem behaviors on the Young Adult Self-Report and Young Adult Behavior Checklist than subjects without suicidal ideation. In addition, scores on measures of overall functioning (the Global Assessment of Functioning Scale) and social and occupational functioning (the Social and Occupational Functioning Assessment Scale) revealed striking differences between the adolescents with suicidal ideation and their peers at age 30.
In self-perceptions of well-being and coping ability, subjects with suicidal ideation of both genders showed lower self-esteem, lower ability to cope with difficult situations, and more need of social support. Subjects with suicidal ideation also reported more interpersonal problems, such as difficulty communicating with others.
The fact that the group with suicidal ideation tended to enter marriage and parenthood as frequently as their peers may be cause for concern. While the assumption of these roles can be a positive sign of reaching adult status (12) , prior investigation has shown that parenting and relational abilities are compromised by psychiatric disorder (38 – 41) . Thus, both the residual and current psychiatric disorders and functional deficits displayed by the subjects with suicidal ideation may impede successful performance of these salient adult roles.
In addition, in several areas of functioning, male subjects with suicidal ideation performed poorly when compared to their peers. Although it appeared that male subjects with suicidal ideation had a comparable history of college completion, marriage, and parenting, they fared worse in several important respects. When compared to female subjects with and without suicidal ideation and male subjects without suicidal ideation, male subjects with suicidal ideation were more likely to have lower socioeconomic status and salary level and less likely to have achieved residential independence or homeownership by age 30.
These findings are similar to those of earlier periods of this prospective study. Data collected when the participants were children indicate that boys classified as having suicidal ideation at age 15 also displayed marked difficulties in their earlier years (11) . These boys were described as being more dependent by their mothers at ages 5 and 9 and as having more health problems at age 9. At age 9, their teachers were also more likely to report difficulties with social/emotional adjustment and peer relations. Moreover, boys with suicidal ideation displayed an increased likelihood of experiencing family violence before age 15. Such childhood problems indicate a potential pattern of vulnerability for later poor functioning. McGee and colleagues (21) suggest that adverse experiences in childhood and maladaptive responses to these experiences may influence later suicidal ideation for boys.
Several limitations should be considered in interpreting the results of our study. First, because the cohort is from a predominately Caucasian working/middle class community, our findings may not be generalized to more racially and economically diverse populations. Second, the small number of subjects may have increased the risk for type II error. The strengths of the study, however, include the prospective nature of data gathered from early childhood to adulthood in a single-age cohort. Repeated administration of standardized instruments from multiple informants over the 15-year period from adolescence to adulthood offers a perspective that few studies can match.
There is growing awareness among clinicians of the importance of suicidal ideation in adolescence. The recent public controversy surrounding the potential relationship between antidepressants and the development of suicidal behavior has also led to an increased focus on suicidal ideation, particularly in clinical populations (42 , 43) . However, there has been less attention focused on the occurrence of suicidal ideation in community groups or its long-term implications. This study illustrates the enduring links between expression of suicidal ideation in mid-adolescence and adult psychopathology, suicidal ideation and behavior, and deficits in functioning 15 years after onset. These findings underscore the need for identification and treatment of adolescent suicidal ideation in order to alleviate immediate distress and forestall future negative consequences.
1. Ahrens B, Linden M, Zaske H, Berzewski H: Suicidal behavior—symptom or disorder? Compr Psychiatry 2000; 41:116–121Google Scholar
2. Dhossche D, Ferdinand R, van der Ende J, Hofstra MB, Verhulst F: Diagnostic outcome of adolescent self-reported suicidal ideation at 8-year follow up. J Affect Disord 2002; 72:273–279Google Scholar
3. Goldney RD, Smith S, Winefield AH, Tiggemann M, Winefield HR: Suicidal ideation: its enduring nature and associated morbidity. Acta Psychiatr Scand 1991; 83:115–120Google Scholar
4. Groleger U, Tomori M, Kocmur M: Suicidal ideation in adolescence—an indicator of actual risk? Isr J Psychiatry Relat Sci 2003; 40:202–208Google Scholar
5. Kessler RC, Borges G, Walters EE: Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry 1999; 56:617–626Google Scholar
6. Lieberman JE: Suicidal ideation and young adults. Am J Psychiatry 1993; 150:171Google Scholar
7. Meehan PJ, Lamb JA, Saltzman LE, O’Carroll PW: Attempted suicide among young adults: progress toward a meaningful estimate of prevalence. Am J Psychiatry 1992; 149:41–44Google Scholar
8. Cooper-Patrick L, Crum RM, Ford DE: Identifying suicidal ideation in general medical patients. JAMA 1994; 272:1757–1762Google Scholar
9. Goldney RD, Dal Grande E, Fisher LJ, Wilson D: Population attributable risk of major depression for suicidal ideation in a random and representative community sample. J Affect Disord 2003; 74:267–272Google Scholar
10. Pfeffer CR, Klerman GL, Hurt SW, Kakuma T, Peskin JR, Siefker CA: Suicidal children grow up: rates and psychosocial risk factors for suicide attempts during follow-up. J Am Acad Child Adolesc Psychiatry 1993; 32:106–113Google Scholar
11. Reinherz HZ, Giaconia RM, Silverman AB, Friedman A, Pakiz B, Frost AK, Cohen E: Early psychosocial risks for adolescent suicidal ideation and attempts. J Am Acad Child Adolesc Psychiatry 1995; 34:599–611Google Scholar
12. Arnett JJ: Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol 2000; 55:469–480Google Scholar
13. Arnett JJ: Conceptions of the transition to adulthood: perspectives from adolescence through midlife. J Adult Development 2001; 8:133–143Google Scholar
14. Levinson DJ: A theory of life structure development in adulthood, in Higher Stages of Human Development: Perspectives on Adult Growth. Edited by Alexander CN, Langer EJ. New York, Oxford University Press, 1990, pp 35–53Google Scholar
15. Centers for Disease Control 2002: Years of potential life lost (YPLL) before age 65. Retrieved November 4, 2004, from http://webappa.cdc.gov/cgi-bin/broker.exeGoogle Scholar
16. American Academy of Child and Adolescent Psychiatry: Practice parameter for the assessment and treatment of children and adolescents with suicidal behavior. J Am Acad Child Adolesc Psychiatry 2001; 40(suppl 7):24S–51SGoogle Scholar
17. Pelkonen M, Marttunen M: Child and adolescent suicide: epidemiology, risk factors, and approaches to prevention. Pediatric Drugs 2003; 5:243–265Google Scholar
18. Freud A: Adolescence as a developmental disturbance, in Adolescence. Edited by Caplan G, Lebovici S. New York, Basic Books, 1969, pp 5–10Google Scholar
19. Lewinsohn PM, Rohde P, Seeley JR: Psychosocial characteristics of adolescents with a history of suicide attempt. J Am Acad Child Adolesc Psychiatry 1993; 32:60–68Google Scholar
20. Brent DA, Baugher M, Bridge J, Chen T, Chiappetta L: Age- and sex-related risk factors for adolescent suicide. J Am Acad Child Adolesc Psychiatry 1999; 38:1497–1505Google Scholar
21. McGee R, Williams S, Nada-Raja S: Low self-esteem and hopelessness in childhood and suicidal ideation in early adulthood. J Abnorm Child Psychol 2001; 29:281–291Google Scholar
22. Pfeffer CR, Hurt SW, Tatsuyuki T, Peskin JR, Siefker CA, Nagabhairava S: Suicidal children grow up: suicidal episodes and effects of treatment during follow-up. J Am Acad Child Adolesc Psychiatry 1994; 33:225–230Google Scholar
23. Reinherz HZ, Paradis AD, Giaconia RM, Stashwick CK, Fitzmaurice G: Childhood and adolescent predictors of major depression in the transition to adulthood. Am J Psychiatry 2003; 160:2141–2147Google Scholar
24. Hollingshead AB, Redlich FC: Social Class and Mental Illness: A Community Study. New York, Wiley, 1958Google Scholar
25. Achenbach TM: Integrative Guide for the 1991 CBCL/4–18, YSR, and TRF Profiles. Burlington, University of Vermont, Department of Psychiatry, 1991Google Scholar
26. Kovacs M: The Children’s Depression Inventory. North Tonowanda, NY, Multi-Health Systems, 1992Google Scholar
27. Burless C, De Leo D: Methodological issues in community surveys of suicide ideators and attempters. Crisis 2001; 22:109–124Google Scholar
28. Hofstra MB, van der Ende J, Verhulst FC: Pathways to self-reported problem behaviors from adolescence into adulthood. Am J Psychiatry 2002; 159:401–407Google Scholar
29. Wittchen H-U, Nelson CB, Lachner G: Prevalence of mental disorders and psychosocial impairments in adolescence and young adults. Psychol Med 1998; 28:109–126Google Scholar
30. Robins LN, Cottler L, Bucholz K, Compton W: NIMH Diagnostic Interview Schedule, Version IV. St Louis, Washington University, Department of Psychiatry, 1997Google Scholar
31. Achenbach TM: Manual for the Young Adult Self-Report and Young Adult Behavior Checklist. Burlington, University of Vermont, Department of Psychiatry, 1997Google Scholar
32. Rosenberg M: Conceiving the Self. New York, Basic Books, 1979Google Scholar
33. Jerusalem M, Schwarzer R: Self-efficacy and stress appraisals, in Self Efficacy: Thought Control of Action. Edited by Schwarzer R, Washington, DC, Hemisphere, 1992, pp 95–213Google Scholar
34. Barrera M: A method for the assessment of social support networks in community survey research. Connections 1980; 3:8–13Google Scholar
35. Gould MS, Kramer RA: Youth suicide prevention. Suicide Life Threat Behav 2001; 31:6–31Google Scholar
36. Vilhjalmsson R, Kristjansdottir G, Sveinbrjarnardottir E: Factors associated with suicidal ideation in adults. Soc Psychiatry Psychiatr Epidemiol 1998; 33:97–103Google Scholar
37. Kuo WH, Gallo JJ, Tien AY. Incidence of suicide ideation and attempts in adults: the 13-year follow-up of a community sample. Psychol Med 2001; 31:1181–1191Google Scholar
38. Beardslee W, Keller MB, Lavori PW, Staley J, Sacks N: The impact of parental affective disorder on depression in offspring: a longitudinal follow-up in a nonreferred sample. J Am Acad Child Adolesc Psychiatry 1993; 32:723–730Google Scholar
39. Johnson JG, Cohen P, Kasen S, Smailes E, Brook JS: Association of maladaptive parental behavior with psychiatric disorder among parents and their offspring. Arch Gen Psychiatry 2001; 58:453–460Google Scholar
40. Kessler RC, Walters EE, Forthofer MS: The social consequences of psychiatric disorders, III: probability of marital stability. Am J Psychiatry 1998; 155:1092–1096Google Scholar
41. Langrock AM, Compas BE, Keller G, Merchant MJ, Copeland ME: Coping with the stress of parental depression: parents’ reports of children’s coping, emotional, and behavioral problems. J Clin Child Adolesc Psychol 2002; 31:312–324Google Scholar
42. Jick H, Kaye JA, Jick SS: Antidepressants and the risk of suicidal behaviors. JAMA 2004; 292:338–343Google Scholar
43. Wessely S, Kerwin R: Suicide risk and the SSRIs. JAMA 2004; 292:379–381Google Scholar

