
Changing Profiles of Service Sectors Used for Mental Health Care in the United States
Abstract
Objective: Redesigning the fragmented U.S. mental health care system requires knowing how service sectors share responsibility for individuals’ mental health needs. Method: Twelve-month DSM-IV mental disorders and their severity were assessed in respondents ages 15–54 from the National Comorbidity Survey (NCS) in 1990–1992 (N=5,388) and the NCS Replication in 2001–2003 (N=4,319). Six profiles involving potentially multiple service sectors were defined, including those in which pharmacotherapy plus psychotherapy (psychiatry profile, general medical with other mental health specialty profile), single modalities (general medical only profile, other mental health specialty only profile), or neither modality (human services only profile, complementary/alternative medicine only profile) could potentially have been received. The use of profiles was compared between surveys. Results: The general medical only profile experienced the largest proportional increase (153%) between surveys and is now the most common profile. The psychiatry profile also increased (29%), as did the general medical with other mental health specialty profile (72%). The other mental health specialty only (–73%), the complementary/alternative medicine only (–132%), and the human services only (–137%) profiles all decreased in use. The elderly, women, minorities, the less educated, and rural dwellers were less likely to use profiles capable of delivering pharmacotherapies and/or psychotherapies. Conclusions: How service sectors share responsibility for peoples’ mental health care is changing, with more care falling to general medical providers rather than specialists. Efforts are required to ensure that people who would benefit have access to the necessary treatment modalities.
The complexity of the U.S. mental health care system, which diffuses responsibilities for patients over multiple service sectors, poses critical challenges for patients, providers, and policy makers. Both a surgeon general’s report (1) and the president’s New Freedom Commission on Mental Health make rational reorganization of the U.S. mental health service system a high priority (2) . Redesigning the delivery system depends on understanding how care is shared across sectors and how these complex relationships are evolving over time.
The Epidemiologic Catchment Area study in the 1980s provided the first glimpse of overlapping responsibilities between service sectors (3) . The general medical sector provided mental health services to 43% of treated patients, including 32% solely. The mental health specialty sector served 40%, including 25% solely, 9% jointly with the general medical sector, and 7.5% with the human services sector. The human services sector provided services to 20%, including 11% solely; self-help sectors served 28%, including 15% exclusively. The National Comorbidity Survey (NCS) a decade later confirmed the fragmented nature of care, with 26% of respondents receiving services from multiple sectors, including 18% from two, 7% from three, and 1% from four sectors (4) .
In the past decade, overall rates of mental health service use in the United States increased from 12% of the population to 20% (5 , 6) . However, significant increases were limited to the general medical (159%), psychiatrist (117%), and other mental health specialty (59%) sectors. An important next step is moving beyond studying individual sector use only to more relevant profiles involving the potential combinations of sectors that people actually use. On one hand, managed care has placed greater emphasis on initial contact in primary care with triage of only more difficult cases to mental health specialists (7) . Newer medications have also made it easier for general physicians to treat people exclusively with pharmacotherapies, without referral to specialists for psychotherapies (8 , 9) . On the other hand, some (10 , 11) but not all (12 , 13) trials of pharmacotherapies and psychotherapies have shown increased efficacy with joint versus isolated use of these modalities. Data on the questionable safety and effectiveness of no health care have also raised concern over the isolated use of complementary/alternative medical or the human services sector for mental health care (14 – 17) .
For this article, we used the NCS and NCS Replication to address three aims. First, we sought to move beyond studying individual sector use to examining the profiles of care involving potential combinations of sectors that people use and how these have changed over the past decade. We focused on six profiles capable of delivering psychotherapy, pharmacotherapy, both, or neither modality. Because using profiles capable of delivering treatments does not necessarily mean those treatments were obtained (18) , we also estimated the extent to which people using services did not receive any active treatment or particular modalities (e.g., combined pharmacotherapy plus psychotherapy). Second, we examined whether the use of specific profiles differed by disorder severity. We did so in light of the greater needs for effective treatment among serious cases and evidence that combined modalities are especially beneficial for them (10 , 11) . Third, we identified predictors of using different profiles to inform efforts to redesign and reorganize the U.S. mental health care system.
Method
NCS and NCS Replication Samples
The original NCS, conducted between 1990 and 2002, was a nationally representative household survey of 8,098 respondents ages 15–54 (4) . A part I diagnostic interview was administered to all respondents, and a part II risk factor interview was administered to a probability subsample of 5,877 respondents who screened positive for mental disorders and a random subsample of the remaining part I respondents (response rate=82.4%).
The NCS Replication in 2001–2003 employed a nationally representative sampling scheme that differed from the NCS in three ways: 1) respondents ages 15–17 were not included, 2) the age range included those 55 and older, and 3) a second respondent was selected in 25% of the households to study within-household aggregation of disorders (19) . The respondents completed a part I diagnostic interview (N=9,282), and a probability subsample completed a part II risk factor interview (N=5,692) (rate of response=70.9%).
Data from both surveys were weighted for differential probabilities of selection, nonresponse, and discrepancies with U.S. Census population distributions on demographic and geographic variables (20 – 22) . After a complete description of the study to the subjects, written informed consent was obtained. Recruitment and consent procedures were approved by the Human Subjects Committees of the University of Michigan and Harvard Medical School (the latter only for the NCS Replication).
Presence and Severity of DSM Mental Disorders
The NCS and NCS Replication made DSM-III-R and DSM-IV, respectively, diagnostic assessments based on the World Health Organization Composite International Diagnostic Interview (CIDI) (23) . Both DSM versions assessed anxiety (panic disorder, generalized anxiety disorder, phobias, and posttraumatic stress disorder), mood (major depressive disorder, dysthymia, and bipolar disorder), and substance use disorders (alcohol and drug abuse and dependence). Good concordance has been observed between most CIDI–diagnosed disorders and blind clinician diagnoses made with the Structured Clinical Interviews for DSM-III-R or DSM-IV (22 , 24) .
NCS Replication respondents who reported 12-month DSM-IV disorders were asked to focus on the month in the past year when symptoms were most persistent and severe and to rate role disability during that month. Sheehan Disability Scale (25) responses were used to define a severity gradient. Seriously ill subjects met criteria for the following: bipolar I or nonaffective psychosis, a suicide attempt or psychiatric hospitalization in the past year, three or more areas of “severe” or “very severe” Sheehan Disability Scale role impairment (i.e., a domain score of 9 or 10), three or more areas of at least “medium” Sheehan Disability Scale role impairment (i.e., a domain score of at least 7 or 8), plus at least four mental disorder diagnoses or more than 5 days of hospitalization or a multivariate functional impairment score equivalent to a Global Assessment Scale score (26) of less than 55. Moderate cases were defined as those having at least “moderate” interference from a mental disorder in any Sheehan Disability Scale life dimension (i.e., a domain score of 4 or greater). All other disorders were classified as mild. In a previous examination of the validity of these ratings (6) , a significant gradient was found in average days out of role reported by patients with serious, moderate, and mild cases.
For NCS respondents, comparable aggregate estimates of disorder presence and severity were developed in nested logistic regression equations that used symptom measures available in both the NCS and NCS Replication to predict the following: 1) serious disorders versus all others, 2) serious-to-moderate disorders versus mild disorders or no disorder, and 3) any disorder (i.e., serious, moderate, or mild) versus no disorder. These were estimated only in the NCS Replication because the measures of seriousness were not available in the NCS. Areas under the receiver-operating characteristic curves indicated good predictive validity (6) .
Multisector Profiles of Care
The respondents to part II of the NCS and NCS Replication were asked whether they ever received mental health services and, if so, whether in the previous 12 months they used providers in each of the following five mutually exclusive service sectors: a psychiatrist; another mental health specialist, including a psychologist or other nonpsychiatrist mental health professional in any setting, a social worker or counselor in a mental health specialty setting, or mental health hot line workers; the general medical sector, including a primary care doctor, another general medical doctor, a nurse, or any other health professional not mentioned; human services, including a religious or spiritual adviser or a social worker or counselor in any setting other than a specialty mental health setting; and complementary/alternative medicine, including any other type of healer or participation in a self-help group.
Based upon their use of individual sectors, we then defined whether the respondents had used six mutually exclusive profiles of care involving potentially multiple sectors. Two profiles capable of delivering combined pharmacotherapies and psychotherapies were the following: the psychiatrist profile (defined as any use of the psychiatrist sector) and the general medical with other mental health specialty profile (defined as use of the general medical plus other mental health specialty sectors without use of the psychiatrist sector). Two profiles capable of delivering single modalities were the following: the general medical only profile (defined as use of the general medical sector without psychiatrist or other mental health specialty sectors) and the other mental health specialty only profile (defined as use of the other mental health specialty sector without the psychiatrist or general medical sectors). Finally, two profiles in which neither modality is likely to have been received were the following: the human services only profile (defined as use of the human services sector without a psychiatrist, another mental health specialty, or the general medical sectors) and the complementary/alternative medicine only profile (defined as use of the complementary/alternative medicine sector without any other sector).
The respondents who made only one visit to any sector, received no psychiatric medications, and were not in ongoing treatment at their interviews were considered to have obtained no active treatment. The respondents were considered to have obtained combined psychotherapy plus pharmacotherapy if they either 1) made eight or more visits to a provider and received a medication or 2) reported being in ongoing treatment at their interviews.
Sociodemographic Correlates
The NCS and NCS Replication asked identical questions to assess age (18–24, 25–34, 34–44, and 45–54 years), sex, race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, or other), marital status (married or cohabiting, previously married, or never married), education (0–11, 12, 13–15, and 16 years or more), household income, and urbanicity. Income was defined as a multiple of the federal poverty line accounting for the composition of the respondent’s family, with low income defined as an income-to-poverty ratio of less than 1.5:1; a low-average income ratio in the range of 1.5:1 to less than 3:1, a high-average ratio in the range of 3:1 to less than 6:1, and a high ratio of 6:1 or greater. Urbanicity was defined with the 1990 (NCS) and 2000 (NCS Replication) U.S. Censuses as large (at least 2 million residents) and small metropolitan statistical areas, central cities and suburbs within metropolitan statistical areas, adjacent areas (areas outside the suburban belt but within 50 miles of the central business district of a central city of a metropolitan statistical area), and rural areas (areas more than 50 miles from the central business district of a central city).
Analysis
The weighted part II data for respondents ages 18–54 were merged. Although some profiles are defined by use of a single sector (e.g., the psychiatrist profile), our analyses focused exclusively on those profiles involving potential combinations of sectors, not on individual sector use. We compared the NCS and NCS Replication for use of each of the six profiles of care defined. Differences were assessed in the overall sample and separately in serious, moderate, mild, and subthreshold 12-month cases. Statistical significance was evaluated by using z tests for the differences in prevalence estimates. Combined data from the two surveys were also used to estimate a series of logistic regression equations predicting use of specific profiles. Standard errors of all prevalence estimates and all logistic regression coefficients were obtained using the Taylor series linearization method (27) implemented in SUDAAN (28) .
Results
Use of Profiles Among All Respondents
Twelve-month prevalences of each profile are shown in the first two sets of rows in Table 1 . In the NCS, the most common profiles, in descending order, were other mental health specialty only, general medical only, psychiatrist, human services only, complementary/alternative medicine only, and general medical with other mental health specialty profiles. In the NCS Replication, the general medical only profile was most common, followed by the psychiatrist, other mental health specialty only, the human services only, general medical with other mental health specialty, and the complementary/alternative medicine only profiles. The greatest increase between surveys occurred in the general medical only profile, followed by the general medical profile with the other mental health specialty profile and the psychiatrist profile (tied), and the other mental health specialty only profile and the human services only profile (tied). The only profile to decrease between surveys was the complementary/alternative medicine only profile (see third set of rows in Table 1 ).

Profiles Used Among Those Receiving Services
To account for the increase (65%) in any service use in the NCS Replication versus the NCS (6) , we also examined 12-month prevalences of profile use just among respondents receiving services ( Table 2 ). The largest increase occurred in the general medical only profile. There were increases in use of the psychiatrist profile as well as the general medical with other mental health specialty profile. There were decreases in the use of the other mental health specialty only, the complementary/alternative medicine only, and the human services only profiles. Among those using any 12-month services, 9.1% (SE=1.3) of the NCS Replication and 15.4% (SE=1.6) of the NCS respondents met our definition for no active treatment. Among those using the psychiatrist profile, 75.8% (SE=2.9) of the NCS Replication and 71.1% (SE=5.0) of the NCS respondents met our definition for combined psychotherapy plus pharmacotherapy; for those using the general medical with other mental health specialty profile, 53.4% (SE=2.3) of the NCS Replication and 37.4% (SE=2.7) of the NCS respondents may have obtained dual-modality treatments.
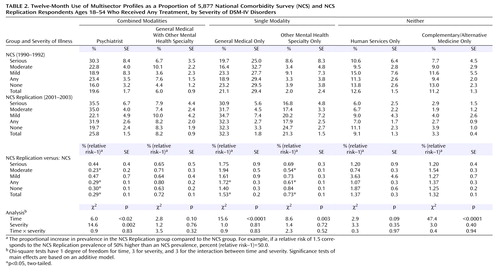
A significant positive relationship existed between severity of disorders and use of the psychiatrist profile, with proportional psychiatrist profile use being roughly 80% higher at the highest versus lowest severity levels in both surveys. Significant relationships with severity were not observed for the use of other profiles. The association between severity and the psychiatrist profile did not vary between surveys, implying that the proportional increase in use of the psychiatrist profile over time was roughly equal across disorder severity levels. The consistency in the relationship between severity and use of the psychiatrist profile between surveys also means that the distribution of severity among people with use of the psychiatrist profile was comparable over time. Only a minority of people diagnosed with use of the psychiatrist profile had serious disorders at either time, and many had mild or subthreshold disorders.
Sociodemographic Correlates of Profile Use
Table 3 presents demographic predictors of using particular profiles with control for disorder severity and time. Age was positively related to use of both the psychiatrist profile as well as the general medical only profile but negatively related to use of the other mental health specialty only profile. Women were less likely than men to use the psychiatrist profile as well as the complementary/alternative medicine only profile but more likely to use the general medical only profile. Hispanics were less likely to use the psychiatrist profile than non-Hispanic whites; Hispanics and non-Hispanic blacks were both more likely than whites to use the human services only profile. Unmarried people were more likely than those who were married to use the other mental health specialty only profile and less likely to use the general medical sector only profile. Education was positively related to use of the psychiatrist, other mental health specialty only, and human services only profiles, but it was negatively related to use of the general medical only profile. Urbanicity was positively associated with use of the complementary/alternative medicine only profile and negatively related to use of the human services only profile.
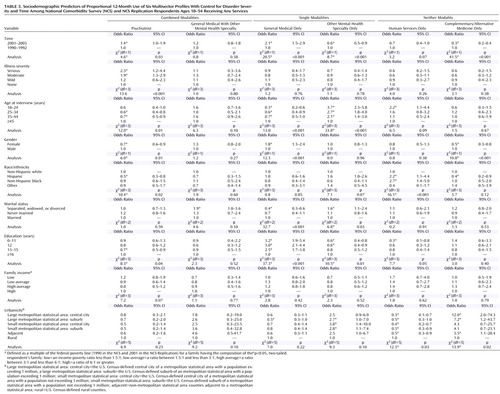
Examination of interactions between predictors and time revealed that significant associations between demographic variables and profile use were generally consistent between surveys. One exception was that a decrease in the human services only profile over time was significantly greater in urban than nonurban areas. No interactions between demographic variables and severity were significant (the data are not shown but are available upon request from the first author).
Discussion
Three sets of limitations should be kept in mind. First, although the methods, instruments, and sector classifications were kept largely the same between the NCS and the NCS Replication, the internal validity of responses could have been affected by even subtle differences in surveys, nonresponse, and nonreporting. For example, mental disorders were assessed differently, and imputation was employed to ensure comparable estimation of prevalences over time. The accuracy of these imputations is supported by strong associations between imputed and direct assessments in the NCS Replication.
Second, we cannot be certain whether those using profiles actually obtained any treatment, particular modalities, or adequate care. Our crude lower-boundary estimates suggested that at least 10%–15% of those using services fail to receive any active treatment. Among those using profiles capable of delivering combined psychotherapy plus pharmacotherapy, perhaps the minority actually obtains these modalities. Even those receiving pharmacotherapies and psychotherapies often fail to receive regimens that meet minimal thresholds for adequacy (18 , 29) . As a consequence, the actual number of patients who receive evidence-based pharmacotherapies and psychotherapies is likely to be much smaller than those with the potential to do so based on their profile use.
Finally, the external validity of these results may be limited because the sampling frame excluded people in institutions as well as the homeless and did not span all diagnostic categories. However, such restricted sampling frames have been shown to exclude only a small proportion of mentally ill people, and clinical reappraisal interviews have found that a vast majority of serious cases are detected by the NCS Replication interview (21) .
With these potential limitations in mind, this study sheds light on both the complexity of the U.S. mental health care delivery system as well as important shifts in the combinations of service sectors that individuals use. The general medical only profile experienced the largest growth over the past decade and is now the most common profile. This increased use of general medical providers without specialists may be because primary care physicians now act as “gatekeepers” for nearly one-half of patients (30) . The provision of mental health care in general medical settings has also been improved through greater understanding of how mental disorders present and the design of primary care screening tools (31 , 32) . The development and heavy promotion of new antidepressants and other psychotropic medications with improved safety profiles have further spurred care of mental disorders exclusively in general medical settings (8 , 9) . There has also been a growing tendency for some primary care physicians to deliver psychotherapies themselves (33) .
Two aspects of this expanded use of the general medical only profile warrant concern. One is that it has occurred equally for people with severe as well as less severe disorders. This is worrisome in light of growing evidence favoring combined psychotherapy and pharmacotherapy for patients with serious disorders (10 , 11) . In addition, general medical care without specialty use may result in lower treatment intensity and adequacy than in specialty care (29 , 34) .
The psychiatry profile is now the second most commonly used profile and also one experiencing growth during the last decade. On one hand, this may seem surprising, given both cutbacks in spending for specialty care as well as warnings by psychiatrists that managed care and gatekeeping would lead to diminished use of their services (32) . This increase may reflect factors similar to those responsible for greater use of nonpsychiatrist physicians, including diminished stigma, greater recognition of the need for mental health treatment, and greater availability and demand for pharmacotherapies (5 , 6 , 35) .
However, it is disconcerting that the temporal increase in use of the psychiatrist profile has not particularly benefited patients with serious conditions. The psychiatrist profile is one of two examined in which combined modality treatment could have been received. As mentioned, evidence has been growing that dual-modality treatments are especially beneficial to those with more serious disorders (10 , 11) . The general medical with mental health specialty profile was the other one from which combined modality treatment could have been received. Unfortunately, it was used only modestly and did not increase between surveys. The fact that it, like the psychiatry profile, was not more likely to be used by severely ill patients raises further questions regarding whether dual-modality treatments are being optimally allocated.
The other mental health specialty only profile, representing possible use of psychotherapy alone, had been the most popular profile in the NCS but declined significantly in the past decade. This finding is consistent with a significant decrease in psychotherapy visits during the 1990s (5 , 33) . It could reflect new restrictions on the number of psychotherapy sessions, increased patient cost sharing, and reduced provider reimbursements for psychotherapy visits imposed by many third-party payers (36) . It could also reflect changes in the popularity of therapeutic modalities, particularly patients’ growing preferences for psychotropic medications (5) .
Decreasing use of the human services only profile may be part of a longer-term decline in the use of the clergy for mental health care (37) . Recent cutbacks in funding and programs in social services agencies may also be contributing to the declining use of this profile (36) . Use of the complementary/alternative medicine only profile also decreased dramatically, perhaps in response to accumulating evidence that these treatments may lack efficacy or pose safety problems (14 , 15) .
Younger cohorts’ greater use of profiles capable of delivering psychotropic medications (the psychiatrist profile or the general medical only profile) could reflect the particular popularity and successful promotion of these agents to younger people (5 , 9) . By contrast, the older cohorts’ reduced use of profiles employing psychotherapy exclusively may reflect an unacceptability of this modality to the elderly (38) . Our observation that women receive fewer psychiatric services but more general medical services for mental health care than men is consistent with earlier findings that primary care physicians are more willing to treat women but tend to refer men to specialists (39) . Racial and ethnic minorities’ greater reliance on the human services only profile may reflect their ease of access to religious leaders or social services agencies, as well as prior experiences of prejudice and mistreatment within profiles involving health care sectors (16 , 17 , 40) .
Nonmarried peoples’ greater use of profiles capable of delivering exclusively psychotherapy and their reduced use of profiles capable of delivering pharmacotherapy exclusively may indicate that counseling is a preferred modality for relational difficulties (41) . Education’s positive relationship with profiles potentially employing psychotherapies and negative relationships with profiles potentially employing pharmacotherapies exclusively may reflect an importance placed on knowledge and cognitive processes in many psychotherapies (42) . Urbanicity’s positive association with the complementary/alternative medicine only profile and its negative association with the human services only profile may be due to structural realities that few complementary/alternative medicine sources are found outside urban areas, whereas religious and social services may be the only resources available to rural residents (43) . The fact that use of the human services without health care only profile did not decline in rural as in urban areas may further indicate the reliance on religious leaders for mental health needs among rural residents.
These results clearly confirm key observations made by the president’s New Freedom Commission on Mental Health: that the U.S. mental health care system remains fragmented and that this complexity may be contributing to many Americans failing to receive the treatments they need (2) . Although this analysis primarily focused on fragmentation of care across sectors, the commission also recognized the equally important fragmentation that can occur within sectors because of the variety of competing clinical (e.g., mental health versus general medical), social, and human service needs that many patients and their clinicians experience (44) .
Beyond documenting these realities, what can be done to address both types of fragmentation and help ensure that Americans with mental health needs receive effective care? In considering this difficult question, the commission recommended overcoming obstacles posed by fragmentation by meeting six goals. The commission’s first goal—increasing American’s awareness of their mental health needs—will almost certainly require renewed educational and awareness campaigns to promote the public’s recognition of disorders and profiles for which effective care can be received (7) . Another goal—early detection and treatment—would benefit from additional application of screening programs as well as timely referrals from profiles involving exclusively non-health-care-providers to those involving health care professionals (31 , 32 , 45) . The goal of increasing high-quality consumer-oriented care will likely require expansion of treatment resources as well as demanding greater accountability for the outcomes resulting from the use of different profiles (46) . Eliminating current disparities in service use suggests that such initiatives and resources should be focused on traditionally underserved groups, including racial and ethnic minorities and rural communities (47) . Final goals call for increased undertaking of best practices that optimally employ generalists, specialists, and health technology. Such interventions may be especially needed to address within -sector fragmentation from competing clinical, social, and human service demands on clinicians’ limited time and resources. Several disease-management models that employ allied health personnel and innovative decision-support systems to assist beleaguered clinicians have already proven to be effective and may deserve wider dissemination (48 – 52) . Recent legislation suggests that the public may already be willing to pay for such programs to ensure that Americans receive effective care (53) . Parallel efforts to define return on investments are needed to generate analogous support among employer purchasers for model programs that help transform the fragmented U.S. mental health care delivery system (37) .
Acknowledgments
Collaborating investigators include Ronald C. Kessler (principal investigator, Harvard Medical School), Kathleen Merikangas (co-principal investigator, NIMH), James Anthony (Michigan State University), William Eaton (Johns Hopkins University), Meyer Glantz (National Institute on Drug Abuse), Doreen Koretz (Harvard University), Jane McLeod (Indiana University), Mark Olfson (Columbia University College of Physicians and Surgeons), Harold Pincus (University of Pittsburgh), Greg Simon and Michael Von Korff (Group Health Cooperative), Philip Wang (Harvard Medical School), Kenneth Wells (UCLA), Elaine Wethington (Cornell University), and Hans-Ulrich Wittchen (Max Planck Institute of Psychiatry).
1. US Department of Health and Human Services: Mental Health: A Report of the Surgeon General. Rockville, Md, NIMH, 1999Google Scholar
2. New Freedom Commission on Mental Health: Achieving the Promise: Transforming Mental Health Care in America: Final Report. Rockville, Md, US Department of Health and Human Services, 2003Google Scholar
3. Regier DA, Narrow WE, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK: The de facto US mental and addictive disorders service system: Epidemiologic Catchment Area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94Google Scholar
4. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS: Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8–19Google Scholar
5. Olfson M, Marcus SC, Druss B, Elinson L, Tanielian T, Pincus HA: National trends in the outpatient treatment of depression. JAMA 2002; 287:203–209Google Scholar
6. Kessler RC, Demler O, Frank RG, Olfson M, Pincus HA, Walters EE, Wang P, Wells KB, Zaslavsky AM: Prevalence and treatment of mental disorders, 1990 to 2003. N Engl J Med 2005; 352:2515–2523Google Scholar
7. Hirschfeld RM, Keller MB, Panico S, Arons BS, Barlow D, Davidoff F, Endicott J, Froom J, Goldstein M, Gorman JM, Marek RG, Maurer TA, Meyer R, Phillips K, Ross J, Schwenk TL, Sharfstein SS, Thase ME, Wyatt RJ: The National Depressive and Manic-Depressive Association Consensus Statement on the Undertreatment of Depression. JAMA 1997; 277:333–340Google Scholar
8. Schatzberg A, Nemeroff CB (eds): Textbook of Psychopharmacology. Washington, DC, American Psychiatric Publishing, 2004Google Scholar
9. Kravitz RL, Epstein RM, Feldman MD, Franz CE, Azari R, Wilkes MS, Hinton L, Franks P: Influence of patients’ requests for direct-to-consumer advertised antidepressants: a randomized controlled trial. JAMA 2005; 293:1995–2002Google Scholar
10. Pampallona S, Bollini P, Tibaldi G, Kupelnick B, Munizza C: Combined pharmacotherapy and psychological treatment for depression: a systematic review. Arch Gen Psychiatry 2004; 61:714–719Google Scholar
11. Hollon SD, Jarrett RB, Nierenberg AA, Thase ME, Trivedi M, Rush AJ: Psychotherapy and medication in the treatment of adult and geriatric depression: which monotherapy or combined treatment? J Clin Psychiatry 2005; 66:455–468Google Scholar
12. Barlow DH, Gorman JM, Shear MK, Woods SW: Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: a randomized controlled trial. JAMA 2000; 283:2529–2536Google Scholar
13. Agency for Health Care Policy and Research: Depression Guideline Panel, Vol 2: Treatment of Major Depression, Clinical Practice Guideline, No 5. Rockville, Md, US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research, 1993Google Scholar
14. Hypericum Depression Trial Study Group: Effect of Hypericum perforatum (St John’s wort) in major depressive disorder: a randomized controlled trial. JAMA 2002; 287:1807–1814Google Scholar
15. Niggemann B, Gruber C: Side-effects of complementary and alternative medicine. Allergy 2003; 58:707–716Google Scholar
16. Wang PS, Berglund PA, Kessler RC: Patterns and correlates of contacting clergy for mental disorders in the United States. Health Serv Res 2003; 38:647–673Google Scholar
17. Weaver AJ: Has there been a failure to prepare and support parish-based clergy in their role as frontline community mental health workers? a review. J Pastoral Care 1995; 49:129–147Google Scholar
18. Wells K, Klap R, Koike A, Sherbourne C: Ethnic disparities in unmet need for alcoholism, drug abuse, and mental health care. Am J Psychiatry 2001; 158:2027–2032Google Scholar
19. Kessler RC, Walters EE: The National Comorbidity Survey, in Textbook of Psychiatric Epidemiology, 2nd ed. Edited by Tsuang MT, Tohen M, Zahner GEP. New York, John Wiley & Sons, 2002, pp 343–362Google Scholar
20. Kessler R, Merikangas K: The National Comorbidity Survey Replication (NCS-R): background and aims. Int J Methods Psychiatr Res 2004; 13:60–68Google Scholar
21. Kessler RC, Little RJ, Groves RM: Advances in strategies for minimizing and adjusting for survey nonresponse. Epidemiol Rev 1995; 17:192–204Google Scholar
22. Kessler RC, Berglund P, Chiu WT, Demler O, Heeringa S, Hiripi E, Jin R, Pennell BE, Walters EE, Zaslavsky A, Zheng H: The US National Comorbidity Survey Replication (NCS-R): design and field procedures. Int J Methods Psychiatr Res 2004; 13:69–92Google Scholar
23. Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Burke J, Farmer A, Jablenski A, Pickens R, Regier DA, et al: The Composite International Diagnostic Interview: an epidemiologic instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Arch Gen Psychiatry 1988; 45:1069–1077Google Scholar
24. Kessler RC, Wittchen H-U, Abelson JM, McGonagle KA, Schwarz N, Kendler KS, Knäuper B, Zhao S: Methodological studies of the Composite International Diagnostic Interview (CIDI) in the US National Comorbidity Survey. Int J Methods Psychiatr Res 1998; 7:33–55Google Scholar
25. Leon AC, Olfson M, Portera L, Farber L, Sheehan DV: Assessing psychiatric impairment in primary care with the Sheehan Disability Scale. Int J Psychiatry Med 1997; 27:93–105Google Scholar
26. Endicott J, Spitzer RL, Fleiss JL, Cohen J: The Global Assessment Scale: a procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry 1976; 33:766–771Google Scholar
27. Wolter KM: Introduction to Variance Estimation. New York, Springer-Verlag, 1985Google Scholar
28. Research Triangle Institute: SUDAAN Release 8.0.1, Jan 2002. Research Triangle Park, NC, RTI, 2002Google Scholar
29. Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC: Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005; 62:629–640Google Scholar
30. Forrest CB: Primary care in the United States: primary care gatekeeping and referrals: effective filter or failed experiment? BMJ 2003; 326:692–695Google Scholar
31. Simon GE, VonKorff M: Recognition, management, and outcomes of depression in primary care. Arch Fam Med 1995; 4:99–105Google Scholar
32. Spitzer RL, Kroenke K, Williams JB: Validation and utility of a self-report version of PRIME-MD: the PHQ Primary Care Study. JAMA 1999; 282:1737–1744Google Scholar
33. Olfson M, Marcus SC, Druss B, Pincus HA: National trends in the use of outpatient psychotherapy. Am J Psychiatry 2002; 159:1914–1920Google Scholar
34. Wells KB, Schoenbaum M, Unutzer J, Lagomasino IT, Rubenstein LV: Quality of care for primary care patients with depression in managed care. Arch Fam Med 1999; 8:529–536Google Scholar
35. Mechanic D, Bilder S: Treatment of people with mental illness: a decade-long perspective. Health Aff (Millwood) 2004; 23:84–95Google Scholar
36. Buck JA: Medicaid, health care financing trends, and the future of state-based public mental health services. Psychiatr Serv 2003; 54:969–975Google Scholar
37. Wang PS, Simon G, Kessler RC: The economic burden of depression and the cost-effectiveness of treatment. Int J Methods Psychiatr Res 2003; 12:22–33Google Scholar
38. Klap R, Unroe KT, Unutzer J: Caring for mental illness in the United States: a focus on older adults. Am J Geriatr Psychiatry 2003; 11:517–524Google Scholar
39. Kessler R: Sex differences in the use of health services, in Illness Behavior: A Multidisciplinary Model. Edited by McHugh S, Vallis M. New York, Plenum, 1986, pp 135–148Google Scholar
40. McLean C, Campbell C, Cornish F: African-Caribbean interactions with mental health services in the UK: experiences and expectations of exclusion as (re)productive of health inequalities. Soc Sci Med 2003; 56:657–669Google Scholar
41. Leaf PJ, Livingston MM, Tischler GL, Weissman MM, Holzer CE III, Myers JK: Contact with health professionals for the treatment of psychiatric and emotional problems. Med Care 1985; 23:1322–1337Google Scholar
42. Wells KB, Manning WG, Duan N, Newhouse JP, Ware JE Jr: Sociodemographic factors and the use of outpatient mental health services. Med Care 1986; 24:75–85Google Scholar
43. Rost K, Fortney J, Fischer E, Smith J: Use, quality, and outcomes of care for mental health: the rural perspective. Med Care Res Rev 2002; 59:231–265Google Scholar
44. Klinkman MS: Competing demands in psychosocial care: a model for the identification and treatment of depressive disorders in primary care. Gen Hosp Psychiatry 1997; 19:98–111Google Scholar
45. Jacobs DG: National Depression Screening Day: educating the public, reaching those in need of treatment, and broadening professional understanding. Harv Rev Psychiatry 1995; 3:156–159Google Scholar
46. Substance Abuse and Mental Health Services Administration (ed): Consumer-Oriented Mental Health Report Card. Rockville, Md, Center for Mental Health Services, SAMHSA, 1996Google Scholar
47. Mental Health: A Report of the Surgeon General: Culture, Race, and Ethnicity: A Supplement to Mental Health: Report of the Surgeon General. http://www.surgeongeneral.gov/library/mentalhealthGoogle Scholar
48. Gilbody S, Whitty P, Grimshaw J, Thomas R: Educational and organizational interventions to improve the management of depression in primary care: a systematic review. JAMA 2003; 289:3145–3151Google Scholar
49. John A Hartford Foundation: The Improving Mood-Promoting Access to Collaborative Treatment (IMPACT) Program. http://www.jhartfound.org/program/impact.htmGoogle Scholar
50. The John D and Catherine T. MacArthur Foundation: Campaign for Mental Health Reform. http://www.mhreform.orgGoogle Scholar
51. The Robert Wood Johnson Foundation: Depression in Primary Care: Linking Clinical & System Strategies. http://www.depressioninprimarycare.orgGoogle Scholar
52. US Department of Veterans Affairs: Mental Illness Research, Education and Clinical Center (MIRECC). http://www.mirecc.med.va.govGoogle Scholar
53. Scheffler RM, Adams N: Millionaires and mental health: Proposition 63 in California. Health Aff (Millwood) 2005; (suppl web exclusives): W5-212–W5-224Google Scholar

