
Natural History of Male Psychological Health, XV: Retirement Satisfaction
Abstract
Objective: Although previous studies of shorter duration have identified numerous risks and protective factors that powerfully influence outcomes in young adulthood and midlife, this long-term prospective study examines the effect of these prognostic factors on age at retirement and satisfaction with retirement. Method: In this prospective study, a cohort of socially disadvantaged men (N=151) were followed from adolescence until a mean age of 75 years (SD=2). Periodic interviews, biennial administration of questionnaires, and physical examinations every 5 years were conducted to determine biopsychosocial risk variables, age at retirement, and satisfaction with retirement. Results: Early age of retirement was found to be a function of preexisting mental and physical health and later age of retirement a function of occupational status. A surprising finding was that risk factors such as poor objective physical health, low income, and depression, which are commonly associated with poor outcomes in young adulthood and in midlife, were largely unrelated to satisfaction with retirement. Conclusions: A relatively high level of satisfaction with retirement was often attained by men who had reported many risk factors for poor child and midlife development (e.g., low IQ, dropping out of school, poor mental health, and being part of a multiproblem family) but who in later life had some positive resources (e.g., a good marriage, a low level neuroticism, enjoyment of vacations, and a capacity for play). In short, retirement may offer some men a fresh lease on life.
Economic and historical changes have led progressively to earlier retirement (1) , and advances have led to an increased active life expectancy. Thus, the length of retirement has increased from roughly 3 years in 1900 to 15 years in 2000 (2 – 4) . Although it has been repeatedly noted that retirement does not adversely affect physical health (4 , 5) , the jury is still out on the effect of retirement on mental health (6) . Indeed, most existing sociological theories of the psychological effects of retirement have proven inadequate (7) , and further research is needed to understand what has become an increasingly important segment of the life course.
In this article, we address two questions regarding retirement: 1) Besides retiring at a mandated age, which currently is a relatively unimportant reason for retiring, why do men retire? and 2) What are the determinants of satisfaction with retirement? To address these questions, we used data from the 60-year prospective Study of Adult Development at Harvard Medical School, which has contrasted two cohorts of men at opposite ends of the social spectrum: a college cohort, selected for social privilege, and an inner-city cohort, selected for social disadvantage.
Over the last 30 years, the Study of Adult Development has confirmed that childhood risk factors identified in other prospective studies (8 – 10) led to unhappiness and failure during the first 25 years of life (11) . By late middle life, however, the study noted many surprises. Maturation and/or successful marriage had often reversed multiproblem childhoods for the better (12 , 13) . Conversely, the penetrance of heredities burdened by alcoholism and depression in midlife often blighted lives that had seemed promising in young adulthood. Our hypothesis was that retirement satisfaction would depend on the same variables that predicted psychosocial satisfaction at midlife.
Method
Since 1970, the Study of Adult Development (14) has followed a socioeconomically disadvantaged sample of 456 inner-city men (13) , chosen in 1940–1944 as nondelinquent comparison subjects for the Gluecks’ studies of juvenile delinquency (15 , 16) , and a socioeconomically advantaged cohort of 268 Harvard college graduates (11 , 17) . The inner-city sample was homogeneous for potential confounders such as school system (all inner-city schools), race (all Caucasian), gender (all male), and parental education (uniformly disadvantaged). Their dates of birth were 1929 ( 2 years). Since the men in both cohorts entered the work force during a period of great economic growth and were further advantaged by white race and GI Bill benefits, they enjoyed superior occupational opportunities. Both cohorts were reinterviewed at approximately ages 25, 30, and 50 years. Since age 45 years, the men from both cohorts have been followed with biennial questionnaires and physical examinations every 5 years. Signed consent forms were obtained in all phases of the study, and the Brigham and Women’s Hospital Institutional Review Board has approved the study annually for the last 12 years.
For the inner-city cohort, the raw data for childhood assessments came from extensive interviews with both subjects and parents and an extensive search of probation, mental health, and social service records for the period before the youths were 16 years old (15) . To reduce halo effects, the 19 ratings for the inner-city cohort described in the following sections were from 13 different sources, and raters for each instrument were blind to the results of most other ratings. The college cohort, described in detail elsewhere (11 , 14) , are discussed only in passing in the current article.
Early-Life Ratings
Early-life ratings covered the period before subjects were age 21 years.
Parental social class
The rating of parental social class was based on Hollingshead and Redlich’s three-factor definition of parental social class (18) , which is based on the father’s education, residence, and occupation. Class I includes physicians and senior executives with college degrees who live in affluent suburbs, class IV includes blue collar workers, and class V includes unskilled laborers with less than a high school education who live in tenements. The parental social class of all but 45 of the 456 inner-city men was class IV or class V.
Intelligence
Intelligence was assessed with an individually administered Wechsler Bellevue Intelligence Test (19) , a normed and validated precursor to the WAIS, when the subjects were in junior high school.
Childhood temperament
Childhood temperament was measured on a 5-point scale on which 1 indicated a good-natured, outgoing temperament; 3 indicated an intermediate temperament, with no clear problems; and 5 indicated significant problems (e.g., very shy, asocial, had tics, phobias, or enuresis) (20) .
Childhood environmental strengths
Childhood environmental strengths were measured on a 3–15-point scale, described in detail elsewhere (12 , 21) , that reflected clinical judgment. Up to 5 points were assigned for the child’s relationship with the mother, the child’s relationship with the father, and the presence of an overall home atmosphere conducive to the “development of basic trust, autonomy and initiative.” Interrater reliability (three raters) ranged from 0.70 to 0.89.
Childhood weaknesses
Childhood weaknesses were measured with a 50-point scale that summed ratings of 25 concrete criteria reflecting the characteristics of multiproblem inner-city families; each criterion was assigned a score of 0–2 points (15 , 21) . Representative items included the presence of eight or more social agency contacts, being raised for more than 6 months apart from both parents, having a mother who was mentally retarded, and having a father who was cruel to the subject. Interrater reliability (three raters) ranged from 0.91 to 0.94.
Midlife Ratings
Independent raters who were blind to all data collected before the subjects reached age 35 years assessed the men primarily on the basis of a semistructured 2-hour interview conducted before the men reached age 50 years. Six variables were rated during the midlife period.
Global functioning
Global Assessment of Functioning (GAF) Scale (essentially axis V of DSM-III [pp. 28–30]) ratings were obtained when the subjects were 47 years old. Ratings were made on a scale from 1 to 100, with higher ratings indicating better functioning. Interrater reliability was 0.69.
Physical health
Physical health was assessed every 5 years by means of a complete physical examination scored by a research internist who was blind to the subject’s other data (22) . Physical health was scored on the following 4-point scale: 1=excellent health; 2=minor irreversible problems; 3=clear life-threatening, irreversible problems; 4=significant irreversible physical disability. Rater reliability measures were not obtained.
Alcohol abuse
Alcohol abuse was assessed when subjects were age 20–50 years. DSM-III criteria were used for assessment. Ratings were made on the following scale: 1=no abuse, 2=alcohol abuse (social complications of alcohol use and difficulty controlling or pathological pattern of alcohol use), 3=alcohol dependence. Assessment was by consensus of two raters.
Smoking
The amount of smoking was calculated in pack/years (number of packs per day times the number of years smoking).
Job status
Job status was assessed at age 50 years. The following modified Duncan seven-category occupational classification was used: 1=professional; 2=manager, minor professional; 3=semiprofessional; 4=technician/clerk; 5=skilled laborer; 6=semiskilled laborer; 7=unskilled laborer (23) .
Income
Income was determined at age 45–55 years. The maximum earned income in midlife was calculated in 1977 dollars and then doubled to approximate year 2000 dollars.
Late-Life Ratings
Adaptation to aging
At age 70 years, the surviving inner-city men were divided into the following three groups on the basis of subjective and objective mental and physical health: happy-well (good subjective and objective mental and physical health), intermediate, and sad-sick (both mentally and physically disabled) (24) .
Income
Income at age 70 years was determined in year 2000 dollars.
Neuroticism
Neuroticism was measured with the NEO Personality Inventory short form (25) , administered when the men were about age 60 years.
Psychosocial adjustment
Psychosocial adjustment was measured at age 50–65 years with the sum of ratings for 10 items reflecting objective estimates of job, marital, and vacation satisfaction and of psychiatric treatment in late midlife (26) . Scores ranged from 9 to 21. The questionnaire was administered eight times over the 15-year period. Rater reliability was 0.87.
Enjoyment of retirement
In 1998, 2000, and 2002, when the inner-city men were age 65–75 years, they were asked to rate numerically their enjoyment of retirement. These ratings were combined and distributed to produce three global ratings of retirement: 1=very satisfying, 2=satisfying, and 3=unsatisfying. On a similar Likert-type scale, the men rated their general mood and their subjective enjoyment of their marriage, children, hobbies, community service, and religion.
Instrumental activities of daily living
Instrumental activities of daily living were assessed when the subjects were age 70 years. Ratings were made on a 14-point self-report scale that included questions about whether the men could climb two flights of stairs, walk 2 miles without resting, drive at night, care for a yard, travel, shop without assistance, etc. (14) .
Age at retirement
Age at retirement was identified as the age at which the subject was last paid for more than 20 hours/week of work. (Two-thirds of the men who were still working after age 70 years worked 35 hours/week or more.)
Statistical Methods
If a man had not retired by age 75 years, his age of retirement (analytically treated as a continuous variable) was recorded as occurring at age 80 years. Simplified categorical percentages are presented in the tables to give the reader a sense of relative proportion. However, to avoid achieving significance due to fortuitous cutoff points, statistical significance is expressed by using Spearman’s correlation (r s ) for continuous predictor and outcome measures. Two-tailed tests were used throughout, except in the analysis of the association of age of retirement with categorical occupational groups, for which analysis of variance was used, and in the multivariate analysis of the association of age of retirement with midlife demographic and health variables, for which Cox proportional hazards analysis was used.
Attrition
Age at retirement was available for 281 of the 456 inner-city men. Of the 175 missing men, 125 had died while still working, and 50 had stopped participating in the study before retirement. Assessment of satisfaction with retirement was available for only 151 (33%) men; 181 (40%) had died before reaching age 70 years—a percentage not higher than expected for white 15-year-old males born in 1930 (26) . An additional 28 (6%) men could not give valid replies to questions about satisfaction with retirement because they were still working. Of the remaining 247 (54%) men eligible to reply, 61 (13% of 456)—an attrition rate of only 0.25% per year—had withdrawn from the study over the preceding half-century. An additional 35 (8%) men did not reply to any of the three questionnaires assessing retirement from age 69 to 74 years. This left a response rate of 151 of 456, or 33%.
Extensive information on the entire group of subjects allowed us to contrast the men who remained active study participants at age 70 years with the subjects who dropped out. Childhood social class, IQ, multiproblem family membership, childhood strengths, years of education, and age of retirement did not distinguish the two groups. Alcohol abuse (χ 2 =11.5, df=2, p<0.0001) and heavy smoking (χ 2 =31.6, df=6, p<0.0001) were more common among those who dropped out due to early death. Mental illness at age 50 years (χ 2 =11.1, df=3, p=0.01), inept social relationships before age 50 years (χ 2 =12.0, df=6, p=0.06), and alcohol abuse (χ 2 =9.0, df=2, p=0.01) were more common among men excluded because of poor participation or withdrawal.
Results
Table 1 illustrates the strong association between high occupational status and later age of retirement in the inner-city cohort. Only 34% of the men retired at the statutory ages of 62 or 65 years. In comparing the Study of Adult Development’s college and inner-city cohorts, we found that despite receiving far more generous pensions, the college cohort retired an average of 5 years later (mean=67.4 years, SD=7.2) than the inner-city men (mean=62.2 years, SD=8.9).
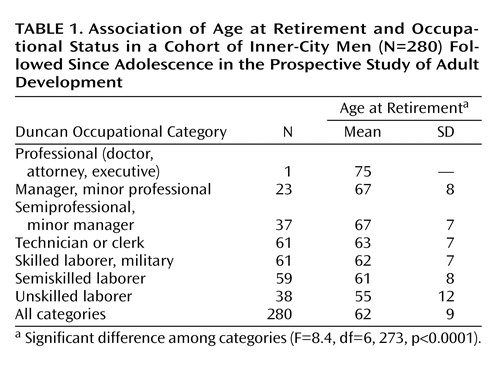
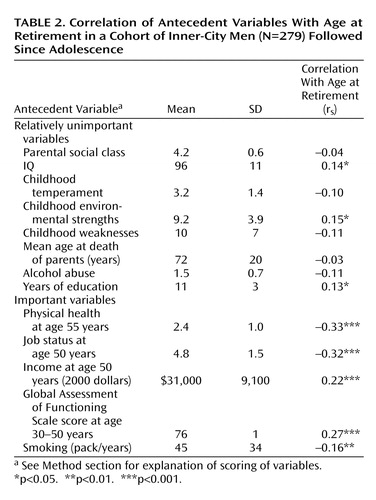
Table 2 reports results of univariate correlations of independent variables with early age of retirement in the inner-city cohort. Parental social class, intelligence, ancestral longevity, and childhood environment (whether assessed by strengths or weaknesses) exerted little effect on age of retirement. The variables most strongly associated with early age of retirement were those associated with low occupational status and premorbid mental and physical disability.
Early retirement, especially before age 60 years, was usually associated with poor physical and/or mental health. The men with the smallest preretirement incomes and smallest postretirement pensions retired earliest. For example, of the 41 inner-city men who retired before age 56 years, 18 had three or more (and an average of four) of the following six psychosocial handicaps: axis II personality disorder, GAF score less than 65 at age 45 years, receipt of psychoactive medication for a month or more, schizophrenia, inability to form intimate relationships, and unemployment for 4 or more years before age 50 years. Of the 23 inner-city early retirees who were not severely psychosocially handicapped, 11 were irreversibly physically disabled by age 55 years. Thus, only 12 of the 41 early retirees were neither mentally nor physically disabled. By age 70 years, only two of the 41 inner-city men who had retired before age 56 years were in the happy-well category of adaptation to aging. In contrast, of the 28 inner-city men still working after age 70 years, none had been psychosocially handicapped at age 50 years, and only one had been physically disabled by age 55 years. At age 70 years, 14 (50%) of the 28 still-employed men were in the happy-well category of adaptation to aging. Compared to the early retirees, only one-half as many of the late retirees abused alcohol.
A multivariate model for time of retirement was built by using Cox proportional hazards analysis ( Table 3 ). Subjects who died or were lost to follow-up before retirement were censored from the model. Two additional multivariate models were also considered to examine predictors of early versus late retirement. For early retirement, subjects who retired after age 62 years were censored; for late retirement, subjects who retired before age 62 years were censored. The results of the analysis suggested that for the study group as a whole, preretirement mental health and physical health were relatively more important than job status. We admit that the seven variables associated with age of retirement were all highly intercorrelated, and this collinearity limited the explanatory power of the regression analysis. Nevertheless, when all seven variables in Table 3 were entered in the regression analysis together, both mental health and physical health remained significant (p<0.02), and no other variables were significantly associated with age of retirement. However, in a comparison of those who retired early (before age 62 years) with those who retired after age 62 years (the minimum statutory age), the findings were different. For subjects who retired before age 62 years, both the GAF score (risk ratio=0.70, p=0.006) and physical health (risk ratio=1.87, p<0.001) predicted retirement, but for subjects who retired after age 62 years, no predictors were significant in the multivariate model.
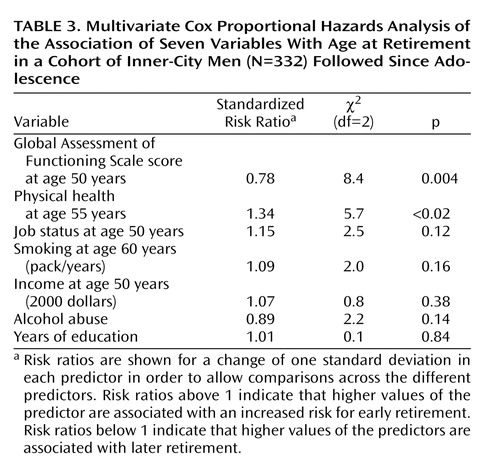
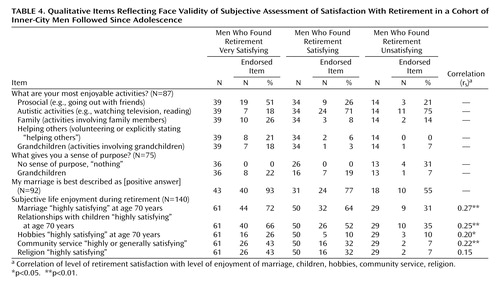
Table 4 presents qualitative data reflecting the face validity of the men’s subjective assessment of their satisfaction with retirement. The men who said they found retirement satisfying were two to three times as likely to report enjoying relationships, volunteering, and play (hobbies), compared with those who said they found retirement unsatisfying. Unfortunately, the numbers of the sentence completion responses were too small for statistical tests to be meaningful. The fact that our measure of retirement satisfaction had only a low correlation with reported mood (excellent to poor) (r s =0.12) ( Table 5 ) suggests that subjective ratings of satisfaction with retirement were relatively independent of positive mood per se.
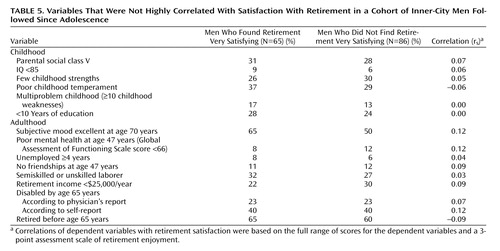
The most surprising finding (illustrated in Table 5 and Table 6 ) was that the inner-city men who most enjoyed retirement were not just those who at retirement were free from physical disability or possessed handsome pension funds. Even more noteworthy, the hallmarks of midlife psychosocial maladjustment—poor work histories, inability to make friends, and depression—were equally distributed between the most and the least happily retired men at age 70–75 years. Place of residence also did not make a difference. The men who remained in the congested areas of inner-city Boston where they had grown up were just as likely to enjoy retirement as those who moved to retirement communities in the Sunbelt. Even physical disability at age 65 years did not significantly predict dissatisfaction with retirement at age 70–75 years, although the lack of correlation of poor health with retirement dissatisfaction was in part an artifact of selective attrition—by age 70 years, a disproportionate number of depressed and chronically ill men had died.
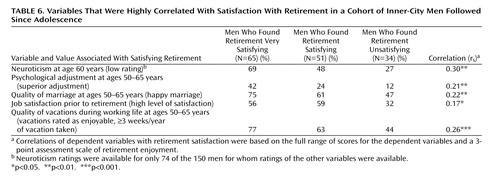
If during retirement one’s past psychosocial slate was wiped relatively clean, what prognostic factors did predict retirement satisfaction? A surprising finding, reflected in Table 4 , was that the levels of objective disability (physical health at age 65 years) and subjective disability (self-reported ability to perform instrumental activities of daily living) of the men who enjoyed retirement were not significantly different from those of the men who found retirement unsatisfying. Rather, the findings reported in Table 6 suggest that the most important preretirement factors leading to happy retirement were evidence of positive mental health rather than an absence of pathology. This evidence included marital enjoyment in late life, low levels of “neuroticism” (i.e., a sanguine temperament, at least as reflected by a pencil-and-paper test) at age 60 years, the capacity to play (enjoyment of vacations), prior job satisfaction, and global mental health. It is not surprising that after-retirement enjoyment of children, marriage, and hobbies was significantly correlated with satisfaction with retirement per se.
Discussion
As the findings reported in Table 4 suggested, the most outstanding differences between the happily and unhappily retired men were their answers to the qualitative questions, “What are your most enjoyable activities?” and “What gives your life a sense of purpose?” The happily retired men were more likely to base their purpose on prosocial and/or creative activities (e.g., “watching grandchildren,” “I know what it is like to be poor so I try to help others,” “writing my memoirs,” “playing piano”). The unhappily retired often answered “nothing” or identified autistic activities such as “watching TV,” “gambling,” or “caring for self.” Of the unhappily retired, only three men reported that helping others gave their lives a sense of purpose.
Two contrasting case histories further illustrate how retirement could create surprising outcomes.
Guido Costello (pseudonym) was psychosocially challenged during most of his life. His father, a gambler and a heavy drinker, spoke almost no English, worked as a fruit peddler, and beat his wife and children. One of Costello’s teachers nominated him as “the worst boy” she had ever taught. She described him as “sullen,” “mean,” “defiant,” “disobedient,” and a “show-off.” She believed he was “heading to trouble.” His tested IQ was 73.
Costello left school after the ninth grade. After having trouble on the job for a while, he quit. He felt he had to “cut himself free” from the responsibilities of a 40-hour-a-week job. When interviewed at age 44 years, he had spent the past 13 years either unemployed or working in a variety of dead-end part-time jobs. He did not seem to have much affinity to his family and was not attached to his children. He was assigned a GAF score of 61.
At age 55 years, despite having stated in the past that he would never take a steady job again, Costello began working full-time as a floor man in the card room of a gambling casino. Until retirement 7 years later, he worked 40 hours a week as a professional card dealer. He enjoyed his job. Having found a creative sublimation, his addiction to gambling ceased to be a problem.
Costello retired at age 62 years. After retirement, he spent his free time reading history books about the Civil War, playing softball, and watching movies. His children, now happily married adults, visited him and his wife “just about every other day.” He was extremely proud of the fact that he had nine grandchildren, for whom he often baby-sat. The interviewer noted that the 67-year-old Costello “expressed quite easily his love for his wife, his three children, and his nine grandchildren.” Five years later at age 72 years, when he was asked to rank his enjoyment of retirement, marriage, and children, Costello rated them all as “highly satisfying.”
In contrast to Guido Costello, Vincent Angelli (pseudonym) had been born to a very warm and stable working-class family.
As a boy, Angelli exhibited a stable temperament, a relatively high IQ, and good coping skills. On evenings and weekends, Angelli helped his father peddle fruit. Angelli’s teachers described him as “not a special problem…self-conscious and hardworking.” His primary hobby was collecting stamps, a hobby that continued for the next half-century.
In 1959, at age 31 years, Angelli founded his own wholesale produce company and served as its president for 11 years. In 1970, his company merged with one of his competitors, and he became the vice-president of the merged company. By 1975, his yearly salary was approximately $135,000 in 2003 dollars. He “worked 8 days a week,” often arriving at work before 6:30 a.m. to help the workers set up and staying until late in the evening. He rarely took vacation time and never missed work because of illness, emotional strain, or fatigue. At age 47 years, he had no retirement plans. He said he might slow down in the future, but he could not see himself not working. In midlife, Angelli sold his part of the business and went to work in a generative fashion as a consultant, buyer, salesman, and general manager for a produce company founded and owned by his sons.
At age 47 years, Angelli appeared as a “pleasant, friendly, and cooperative” individual who “did not seem to have any problems that interfered with his life.” Nevertheless, the interviewer felt that something about his life was “narrow and restrictive.” Since age 12 years, Angelli “had known nothing but work…and work had become his way of life…apart from his pride in his children, and his stamp collection, he did not really seem to have any other interest in life.”
In 1993, at age 65 years, Angelli was forced into retirement due to degenerative arthritis of the right hip, but he continued to view his most important task as “caring for adults younger than myself, coaching the next generation.” Nevertheless, his postretirement subjective enjoyment was quite low. At the beginning of his marriage, Angelli had “laid down the law,” telling his wife he would be in charge of running the business and earning money, while she would be in charge of raising their children and taking care of the house. After retirement, Angelli, who for 20 years had consistently rated his marriage as “good,” now, no longer working, rated his marriage as only “fair.” Four years later, he rated his marriage as “poor” and “not very satisfying.” After 8 years of retirement, he described his marriage as “poor” and “not at all satisfying.” When asked to rank his level of satisfaction over the past 20 years with various areas of his life, including retirement, the only activity he rated as “highly satisfying” was his income-producing work—now, alas, in the distant past.
In summary, the very risk factors associated with bleak young adulthood (28) and the very risk factors associated with bleak midlife adjustment appeared to exert relatively little effect on whether the men, followed since 1940, currently enjoyed retirement. Although poor health and poor psychosocial adjustment often precipitated early retirement, once retirement occurred, neither poor health nor premature retirement was associated with reported levels of retirement enjoyment. It appeared as if retirement created—for these men at least—a new age and a third chance at a contented life.
There is considerable support for the association of retirement with improved mental health and the reduction of depression (29 , 30) . Other studies have supported our finding that marital satisfaction and sanguine personality style, rather than income or health, appear to be the most significant sources of retirement satisfaction (31 , 32) . Our findings, however, must be accepted with caution. First, attrition was selective and excluded a disproportionate number of the depressed, alcoholic, and physically disabled men whose completed reports might have strengthened the correlation of these disorders with retirement dissatisfaction. Second, although evidence exists that subjective well-being can be validly assessed with simple as well as complex measures (33) , our assessment of retirement satisfaction was crude.
Perhaps the most important adjunct to happy retirement, besides a sense of purpose and a good marriage, was learning how to play again. “Play” is defined as behaviors that are highly gratifying to the individual and that do not injure the social order, do not contribute to the gross national product, and do not necessarily evoke societal praise or encouragement. Play not only appeared to provide a new lease on life for some men who as adults had earlier failed at working and loving, it also provided a means of actively exploring and enjoying the relationship of self to the outside world. Unlike in the world of work and love, in the world of play, the people in the outside world need not respond.
1. Han SK, Moen P: Clocking out: temporal patterning of retirement. Am J Sociol 1999; 105:191–236Google Scholar
2. Gruber J, Wise DA: Introduction and summary, in Social Security and Retirement Around the World. Edited by Gruber J, Wise DA. Chicago, University of Chicago Press, 1999, pp 1–36Google Scholar
3. Hedstrom P, Ringen S: Age and income in contemporary society: a research note. J Soc Policy 1987; 16:227–239Google Scholar
4. Mein G, Martikainen, Hemingway H, Stansfeld S, Marmot M: Is retirement good or bad for mental and physical health functioning? Whitehall II Longitudinal Study of Civil Servants. J Epidemiol Community Health 2003; 57:46–49Google Scholar
5. Ekert D, Baden L, Bosse R, Dibbs E: The effects of retirement on physical health. Am J Public Health 1982; 73:779–783Google Scholar
6. Kim JE, Moen P: Is retirement good or bad for subjective well-being? Current Directions in Psychological Science 2001; 10:83–86Google Scholar
7. Mein G. Higgs P, Ferric J, Stansfeld SA: Paradigms of retirement: the importance of health and ageing in the Whitehall II Study. Soc Sci Med 1998; 47:535–545Google Scholar
8. Garmezy N: Stressors of childhood, in Stress, Coping, and Development in Children. Edited by Garmezy N, Rutter M. New York, McGraw-Hill, 1983, pp 43–84Google Scholar
9. Rutter M, Yule B, Quinton D, Yule W, Berger M: Attainment and adjustment in two geographical areas, III: some factors accounting for area differences. Br J Psychiatry 1974; 125:520–533Google Scholar
10. Werner EE, Smith RS: Vulnerable But Invincible. New York, McGraw-Hill, 1995Google Scholar
11. Vaillant GE: Adaptation to Life. Boston, Little, Brown, 1977Google Scholar
12. Vaillant GE, Vaillant CO: Natural history of male psychological health, X: work as a predictor of positive mental health. Am J Psychiatry 1981; 38:1433–1440Google Scholar
13. Vaillant GE: The Wisdom of the Ego. Cambridge, Mass, Harvard University Press, 1993Google Scholar
14. Vaillant GE: Aging Well. Boston, Little, Brown, 2002Google Scholar
15. Glueck S, Glueck E: Unraveling Juvenile Delinquency. New York, Commonwealth Fund, 1950Google Scholar
16. Glueck S, Glueck E: Delinquents and Nondelinquents in Perspective. Cambridge, Mass, Harvard University Press, 1968Google Scholar
17. Heath C: What People Are. Cambridge, Mass, Harvard University Press, 1945Google Scholar
18. Hollingshead AB, Redlich FC: Social Class and Mental Illness. New York, John Wiley & Sons, 1958Google Scholar
19. Wechsler D: The Measurement of Adult Intelligence. Baltimore, Williams & Wilkins, 1939Google Scholar
20. Vaillant GE: Natural history of male psychological health, II: some antecedents of healthy adult adjustment. Arch Gen Psychiatry 1974; 31:15–22Google Scholar
21. Vaillant GE: Natural History of Alcoholism Revisited. Cambridge, Mass, Harvard University Press, 1995Google Scholar
22. Vaillant GE: Natural history of male psychological health: effects of mental health on physical health. N Engl J Med 1979; 301:1249–1254Google Scholar
23. Duncan OD: A socioeconomic index for all occupations, in Occupations and Social Status. Edited by Reiss A Jr. New York, Free Press, 1961, pp 109–138Google Scholar
24. Vaillant GE, Mukamal K: Successful aging. Am J Psychiatry 2001; 158:839–847Google Scholar
25. Costa PT, McCrae RR: The NEO Personality Inventory Manual. Odessa, Fla, Psychological Assessment Resources, 1985Google Scholar
26. Vaillant GE, Vaillant CO: Natural history of male psychological health, XII: a 45-year study of successful aging at age 65. Am J Psychiatry 1991; 147:31–37Google Scholar
27. US Department of Health and Human Services: Vital Statistics of the United States 1988, vol II: Mortality, Part A. Washington, DC, US Government Printing Office, 1989Google Scholar
28. Vaillant GE, Orav J, Meyer SE, McCullough L, Roston, D: Late life consequences of affective spectrum disorder. Int Psychogeriatr 1996; 8:1–20Google Scholar
29. Gall TL, Evans DR, Howard J: The retirement process: changes in the well-being of male retirees across time. J. Gerontol B Psychol Sci Soc Sci 1997; 57:110–117Google Scholar
30. Reitzes DC, Mutran EJ, Fernandez ME: Does retirement hurt well-being? Gerontologist 1996; 36:649–656Google Scholar
31. Machen MJ: Differences between adjustment to and enjoyment of retirement. Can J Aging 1982; 2:3–8Google Scholar
32. Fouquereau E, Mullet E: Reasons for retirement, satisfaction with retirement and sources of enjoyment among retirees: an English-French comparison, in Advances in Psychology Research, vol 2. Hauppauqe, NY, Nova Science Publishers, 2001, pp 31–42Google Scholar
33. Diener E: Subjective well-being. Annu Rev Sociol 1993; 19:353–373Google Scholar

