
Association of the Dopamine D4 Receptor Gene 7-Repeat Allele With Neuropsychological Test Performance of Children With ADHD
Abstract
OBJECTIVE: Association between attention deficit hyperactivity disorder (ADHD) and the 7-repeat allele of a variant (a 48bp variable number of tandem repeats) in the dopamine D4 receptor gene (DRD4) has been widely documented. A meta-analysis of 21 studies revealed evidence of significant association. In this article the authors examine whether the DRD4 7-repeat allele is associated with performance on a variety of neuropsychological tasks in children with ADHD. METHOD: The presence or absence of the 7-repeat allele was determined in 133 drug-naive children 6 to 13 years of age who fulfilled diagnostic criteria for ADHD. These children were then assessed on several neuropsychological tests known to be associated with attention, impulse control, and response inhibition (the Continuous Performance Test, Matching Familiar Figures Test, Go/No Go Task, and Stop Task). Activity levels were assessed with an actigraph. Children with and without at least one 7-repeat allele were compared with each other and with children in a previous population-based study. RESULTS: Children who had the 7-repeat allele had significantly more incorrect responses on the Matching Familiar Figures Test (16.1 versus 14.3) than children who did not have the allele. Children with the allele also had shorter mean reaction times for incorrect responses on the Matching Familiar Figures Test (846.1 versus 1103.7 msec) and on the Stop Task (116.6 versus 134.1 msec) than children without the allele. Children with the allele also displayed higher activity levels. The children with and without the allele did not differ significantly in number of ADHD symptoms when the symptoms were split into the areas of inattention and hyperactivity/impulsivity. Both groups of children with ADHD were more neuropsychologically impaired than the nonpatient comparison group. CONCLUSIONS: In children with ADHD, possession of the DRD4 7-repeat allele appears to be associated with an inaccurate, impulsive response style on neuropsychological tasks that is not explained by ADHD symptom severity.
Attention deficit hyperactivity disorder (ADHD) has been shown to be familial and highly heritable (1). In view of such findings, there has been a wealth of molecular genetic studies attempting to identify susceptibility genes for ADHD (2). To date, there has been a large emphasis on association studies of variants within genes coding for enzymes and receptors involved in the dopaminergic system, although many others have also been examined.
Molecular genetic study findings showing association between ADHD and a variant—a 48bp variable number of tandem repeats (VNTR)—in the third exon of the dopamine D4 receptor gene (DRD4) have been widely replicated but are not entirely consistent (2). In 2001, in a meta-analysis of 21 studies (13 of which had initially found positive results), Faraone et al. (3) concluded that there was a small but significant association between the DRD4 7-repeat allele and ADHD in both family-based (odds ratio=1.4, 95% confidence interval [CI]=1.1–1.6) and case-control (odds ratio=1.9, 95% CI=1.4–2.2) studies. It cannot be ruled out that the 48bp VNTR is in linkage disequilibrium with another variant in the DRD4 and that the 7-repeat allele is not a true risk allele. However, there has been some evidence to suggest that the 7-repeat allele is functional (4).
To move on from this finding, it is now necessary to investigate what aspects of the ADHD phenotype are associated with the DRD4 7-repeat allele. This has received little attention, although preliminary findings suggest that the DRD4 7-repeat allele may increase the risk for behavioral rather than cognitive manifestations of ADHD. Holmes et al. (5) found evidence of association of the DRD4 7-repeat allele only in those children who had conduct problems in addition to ADHD. Swanson et al. (6) examined a subgroup of 32 children with ADHD and surprisingly found that those with the DRD4 7-repeat allele did not differ significantly from a control group on neuropsychological tests, whereas those without the 7-repeat allele did. Finally, findings from a recent study (7) suggest that the DRD4 7-repeat allele may have arisen as a relatively new and rare variant but increased in frequency due to positive selection. The authors of this study speculated that the DRD4 7-repeat allele may be associated with traits such as novelty seeking that could confer advantage in certain situations.
If the DRD4 7-repeat allele is associated with ADHD, and so far much of the available evidence is consistent with this, it will be crucial to examine how this risk is conferred and to investigate what specific susceptibility is increased. To address these questions, one strategy is to examine intermediate phenotypes (also referred to as endophenotypes) such as neuroimages of brains of ADHD patients or indices of neuropsychological functioning that might represent a link in the path from gene to psychiatric disorder (8). Neuropsychological measures have been suggested as suitable endophenotypes for ADHD (9, 10) and are now beginning to be examined in genetic studies (11).
We set out to compare whether drug-naive children with ADHD who did or did not have the 7-repeat allele differed from each other in performance on a variety of neuropsychological measures. Preexisting comparison data on children who did not have ADHD enabled us to investigate whether any differences found between the patient groups represented a departure of one patient group, but not the other, from the norm (as found by Swanson et al. [6]).
We hypothesized that there would be significant differences in performance on neuropsychological tests between children with ADHD who did or did not have a 7-repeat allele and that both groups would perform worse than nonpatient comparison subjects.
Method
Subjects and Diagnostic Assessment
The subjects consisted of 133 drug-naive Caucasian British children (122 boys and 11 girls) referred to child and adolescent psychiatry clinics in Greater Manchester, U.K., with a suspected diagnosis of ADHD. Children were between 6 and 13 years old (mean=9.2, SD=1.8). Subjects were excluded if they had a known neurological condition (including pervasive developmental disorder, epilepsy, or Tourette’s syndrome) or an IQ below 70 assessed by using the WISC-III. The study was approved by the North West Multicentre Ethics Committee. Informed written consent was obtained from each parent and written assent from each child.
The parent version of the Child and Adolescent Psychiatric Assessment (12) was administered by trained interviewers for each child. Additional teacher reports (13) were obtained and diagnoses assigned according to DSM-IV, DSM-III-R, and ICD-10 criteria. Subjects were excluded if they did not meet diagnostic criteria for ADHD or hyperkinetic disorder. Full details of the assessment and diagnostic process have been described previously (5).
Neuropsychological Measures
Children completed a battery of neuropsychological tests, consisting of the Matching Familiar Figures Test (14) and the Stop Task, Go/No Go Task, and Continuous Performance Test from the Maudsley Attention and Response Suppression Task Battery (15).
The Continuous Performance Test had a display time of 1 second and an interstimulus interval of 1.5 seconds. The test battery was performed with a UMAX (Milton Keynes, U.K.) multimedia portable computer (model 290) with a 10-inch screen displaying in black, white, and red. The researcher read standardized instructions to each participant before the test started, and a practice session was given before each trial to ensure that the child understood the procedure. To provide assistance if necessary, the researcher remained in the room during the trials. The Continuous Performance Test provided the number of targets missed (omission errors, considered to be a measure of inattention) and the number of times the button was incorrectly pressed (commission errors, considered a measure of both sustained attention and impulse control) (16).
The Matching Familiar Figures Test was developed as a measure of impulse control (17). The measures derived were the reaction time for correct responses, the reaction time for incorrect responses, and the number of correctly identified pictures. In the Go/No Go Task, response time to the Go stimuli and percentage of successful inhibitions to the No Go stimuli were taken as measures of response inhibition (15). For the Stop Task, overall response time and successful inhibitions were again taken as measures of response inhibition (15).
Finally, an actigraph (18) attached to the child’s nondominant wrist was used to measure activity levels objectively. The children wore actigraphs throughout the WISC-III-R and Maudsley Attention and Response Suppression Task Battery (between 1 and 2 hours). Their mean “activity score” was calculated, reflecting changes in the frequency and intensity of body movements.
Comparison data were available for a group of 40 children (all 9-year-old boys) from Greater Manchester, U.K., randomly selected from a population-based twin register (5, 19), who undertook the same versions of the Matching Familiar Figures Test and the Continuous Performance Test. Data from one randomly selected twin of each pair were used. For the Stop Task and Go/No Go Task, published comparison data for community children without ADHD were examined (15).
Laboratory Methods
DNA was extracted from blood samples and buccal cells. Genotyping of the 48bp VNTR in exon 3 of the DRD4 was performed according to previously described standard laboratory protocols (5).
Statistical Analysis
For the Continuous Performance Test and Matching Familiar Figures Test, those children with at least one DRD4 7-repeat allele, those without a DRD4 7-repeat allele, and nonpatient groups were compared by using one-way analysis of variance (ANOVA). Games-Howell post hoc analyses were used to investigate the nature of any significant differences. For the Go/No Go Task and Stop Task, actigraph data, and clinical data, analyses used independent t tests. When the distribution of data was skewed and could not be transformed to approximate normality, the Mann-Whitney U test was used. Chi-square analyses were used to analyze categorical data (sex and comorbidity). Finally, stepwise logistic regression analysis was undertaken to determine which neuropsychological tasks contributed significantly to the differences between the children with and without the 7-repeat allele. All neuropsychological task measures were included as independent variables, and the dependent variable was dichotomous (member of either the group with or the group without the 7-repeat allele). For all statistical tests, results were considered to be significant at p≤0.05. All analyses were performed with SPSS for Windows (version 10) (SPSS, Inc., Chicago).
Results
Patient Characteristics
All 133 of the children with ADHD met diagnostic criteria for DSM-III-R or DSM-IV ADHD or ICD-10 hyperkinetic disorder: 87 (65.4%) were diagnosed with ICD-10 hyperkinetic disorders, 95 (71.4%) with DSM-IV ADHD combined type, 15 (11.3%) with DSM-IV ADHD hyperactive/impulsive subtype, 10 (7.5%) with DSM-IV ADHD inattentive subtype, and 126 (94.7%) with DSM-III-R ADHD. In addition to ADHD, 78 (58.6%) of the children had oppositional defiant disorder, 16 (12.0%) had conduct disorder, 17 (12.8%) had tic disorders (although children with Tourette’s syndrome were excluded from the study), four (3.0%) had anxiety disorders, and two (1.5%) had depressive disorders. The children’s mean IQ according to the WISC-III-R was 91.2 (SD=13.0).
The patients were divided into two groups on the basis of their DRD4 48bp VNTR genotype: those with one or more 7-repeat alleles and those without any DRD4 7-repeat alleles. Of the 133 individuals taking part in this study, 51 (38.3%) were in the group with the 7-repeat allele and 82 (61.7%) were in the group without the allele. The two groups did not differ significantly in age (t=0.36, df=131, p=0.72), gender (χ2=1.33, df=1, p=0.25), or IQ (t=0.47, df=131, p=0.64).
Clinical Comparison of the Two Patient Groups
There were no differences between the groups with and without the 7-repeat allele on combined (χ2=0.51, df=1, p=0.82), inattentive (χ2=0.01, df=1, p=0.91), or hyperactive/impulsive (χ2=2.4, df=1, p=0.12) subtype of DSM-IV ADHD diagnosis. Children with the 7-repeat allele had a significantly higher total number of ADHD symptoms than the children without the 7-repeat allele (t=–2.18, df=131, p=0.03). However, the groups did not differ significantly in number of symptoms when the symptoms were split into the individual areas of inattention (p=0.13) and hyperactivity/impulsivity (p=0.80) (Mann-Whitney U tests).
The group with the 7-repeat allele showed significantly higher rates of oppositional defiant disorder and conduct disorder than the group without the 7-repeat allele (χ2=3.77, df=1, p=0.05). There were no differences between the groups in the frequency of comorbidity for depressive, tic, and anxiety disorders.
On the actigraph, the group with the 7-repeat allele had a significantly higher activity level (mean=40, SD=17.2) than the group without the 7-repeat allele (mean=33.5, SD=14.9) (t=2.11, df=131, p=0.04).
Neuropsychological Tests
Continuous Performance Test
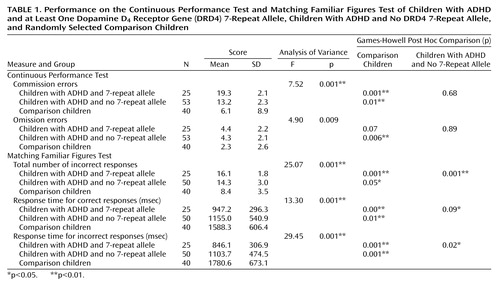
The three groups differed significantly on both the number of commission errors (p=0.001) and omission errors (p=0.009). Post hoc analyses showed that this was attributable to significant differences between both ADHD groups and the comparison group (Table 1) rather than differences between the groups with and without the 7-repeat allele.
Matching Familiar Figures Test
One-way ANOVAs showed that the three groups differed on all measures: number of incorrect responses, response time for correct responses, and response time for incorrect responses (all p<0.001) (Table 1). Games-Howell post hoc analyses showed significant differences between means not only between the comparison group and the ADHD groups with and without the 7-repeat allele on all three measures but also between the two patient subgroups. The ADHD patients with and without the 7-repeat allele differed significantly on the number of incorrect responses and response time for incorrect responses. There was a nonsignificant difference in the response time for correct responses (the children with the 7-repeat allele were faster) (Table 1).
Go/No Go Task
Table 2 presents the mean scores for the Go/No Go Task for the two patient subgroups and published comparison data (15). No significant differences were found between the two patient groups for mean response time or percentage of inhibitions. The ADHD group without the 7-repeat allele did not differ significantly from the comparison group on mean response time. However, a significant difference was found between the ADHD group with the 7-repeat allele and the comparison group (Table 2).
Stop Task
For the Stop Task, the comparison group again consisted of published data. On this task, the children with ADHD and the 7-repeat allele had a significantly shorter mean response time than the children with ADHD but no 7-repeat allele (Table 2). The children with ADHD and the 7-repeat allele were also significantly different from the comparison group at the p<0.05 level, but there was no such difference for the children with ADHD but no 7-repeat allele. The ADHD groups did not significantly differ with regard to their percentage of inhibitions (Table 2).
Logistic Regression Analysis
Logistic regression analysis was performed to select the set of tasks best distinguishing between the children with ADHD who did or did not have the 7-repeat allele. The result indicated that the measures of response time for the Stop Task (beta=–0.25, p<0.05) and number of incorrect responses for the Matching Familiar Figures Test (beta=0.25, p<0.05) were significant predictors of differences between the groups with and without the 7-repeat allele.
Discussion
In keeping with our hypotheses, we found that among children with ADHD, those with the DRD4 7-repeat allele differed significantly from the group without this allele in terms of performance on a variety of neuropsychological tasks. Overall, the group with the 7-repeat allele appeared to show greater impulsiveness in that their responses in the Matching Familiar Figures Test were faster and less accurate and their mean reaction time on the Stop Task was significantly faster. There were no differences between the two groups on the attentional measure (on the Continuous Performance Test) or response inhibition (percent of inhibitions on the Stop Task and Go/No Go Task) components of the neuropsychological battery. Comparison data for the Matching Familiar Figures Test and Continuous Performance Test were significantly different from those of both clinical groups.
In stepwise logistic regression analyses, those tasks which contributed significantly to differences between the groups with and without the 7-repeat allele were selected. This analysis takes into account (i.e., corrects) possible correlations between the tasks. The results indicated that the Stop Task response time and number of incorrect responses on the Matching Familiar Figures Test were the most significant contributors to the differences between the two patient groups, further confirming our findings.
Our findings suggest that ADHD patients with the 7-repeat allele show a more rapid, inaccurate, impulsive response style on neuropsychological tasks than ADHD patients without this allele. Our results also suggest that ADHD patients who have the DRD4 7-repeat allele are significantly more active according to actigraph measures and more severely clinically affected in terms of total ADHD symptom scores (although not specifically clinical symptoms of impulsiveness assessed by interview) and comorbid oppositional defiant or conduct disorders.
It is possible that the differences found in the neuropsychological tests are secondary to the finding that the children with the 7-repeat allele had a significantly greater number of ADHD symptoms. To test this hypothesis, we performed a multivariate analysis of variance (MANOVA) of the significant neuropsychological tests with total ADHD scores as a covariate (i.e., correcting the results for differences in total ADHD score). The results showed that the neuropsychological test scores of the groups were still significantly different. MANOVA was also performed on performance on neuropsychological tests with presence or absence of a conduct disorder as a grouping variable. This proved to be nonsignificant (Pillai’s trace=0.28).
Although we reach similar conclusions (that the DRD4 7-repeat allele is more strongly associated with behavioral than cognitive manifestations of ADHD), our findings differ significantly from those of Swanson et al. (6). They found no differences between subjects with the 7-repeat allele (N=13) and a control group (N=48). They also showed that subjects without the 7-repeat allele (N=19) had more attentional and response inhibition difficulties assessed with a color-word task, cued detection task, and go-change task. In contrast, we found that children with ADHD who did or did not have the 7-repeat allele differed from normal comparison subjects; children with the 7-repeat allele had greater differences from the comparison subjects than children without the 7-repeat allele. Our study also found differences in the number of ADHD symptoms according to possession of the 7-repeat allele. Swanson et al., however, noted that their finding of no difference in ADHD symptom scores could be attributed to the fact that they used only subjects who fulfilled DSM-IV criteria for the combined type of ADHD. Additional differences between our study and that of Swanson et al. are that our children were drug-naive, so that medication levels cannot have influenced our results, and we used different tasks.
To further investigate whether the DRD4 7-repeat allele is a risk allele for poor performance on particular neuropsychological task measures, genotypic as well as phenotypic data on a large comparison group would be needed. However, to avoid the potential problem of population stratification (false positive genetic results arising from unmeasured differences in patients and comparison subjects), which may also be an issue for this study, a family-based study of a general population sample (using, for example, the Quantitative Transmission Disequilibrium Test [20]), would be preferable (i.e., neuropsychological data would be needed from a large population sample with genotypic data from affected offspring as well as their parents). This would allow a statistically more robust, although less powerful, family-based method of analysis, in which it could be tested whether preferential transmission of the 7-repeat allele from parent to offspring affects neuropsychological task performance. Although Quantitative Transmission Disequilibrium Test analysis could be undertaken in a clinical sample (like our own), this type of analysis would not test whether the DRD4 7-repeat allele affects the overall level of task performance but only whether it affects variability of performance within subjects.
Limitations
There are several limitations of this study, which may place caveats on the interpretation of the results. First, because our main aim was to compare children with and without the 7-repeat allele, the comparison data were not collected as part of this study. The twin sample we used may not be the ideal comparison group. Nevertheless, given the findings of Swanson et al. (6), we presented these data from normal children for comparison. Moreover, the comparison data for the Continuous Performance Test and Matching Familiar Figures Test were obtained from a cohort sample of similar age and from the same area of Northwest England. A second limitation is that neuropsychological data were not available for all of the children with ADHD. However, those who performed all tests did not significantly differ from those who did not on any clinical or demographic measures.
We also have to consider that instead of reflecting a true association with ADHD, the DRD4 48bp variant is in linkage disequilibrium with another polymorphism. To further explore this issue, we repeated our analyses on a functional polymorphism in the DRD4 promoter region (a –521 C>T substitution at the 5′ promoter region) (21). We found no association with any task measure (results are available from the first author).
Because of the number of analyses performed, it is possible that our results are attributable to multiple testing. However, the results were all in the hypothesized direction, and positive findings were shown across a variety of tests. Furthermore, several results were significant at the p<0.01 level and remained positive in regression analysis. Therefore, it seems unlikely that the results are simply due to multiple testing. Finally, since our findings extended to different neuropsychological tasks, actigraph, and clinical interview measures, the likelihood is reduced that all these differences have arisen by chance alone.
Nevertheless, further replication of this study is needed, and clearly there are good grounds for examining other task measures (9, 10, 22) as well. However, conducting large-scale studies on drug-naive children (or drug-free children) may be difficult given that children are given stimulant medication fairly quickly once they are diagnosed with ADHD.
Conclusions
In conclusion, children with ADHD who possess the DRD4 7-repeat allele appear to differ from those who do not have the 7-repeat allele on neuropsychological task measures. Specifically, children with ADHD and a copy of the 7-repeat allele were faster and less accurate than those without the allele.
 |
 |
Received Feb. 12, 2003; revision received May 27, 2003; accepted June 6, 2003. From the Department of Psychological Medicine, University of Wales College of Medicine. Address reprint requests to Professor Thapar, Department of Psychological Medicine, University of Wales College of Medicine. Supported by the Wellcome Trust, Action Research, and Sport Aiding Medical Research for Kids. The authors thank Jane Holmes, Tracey Hever, Richard Harrington, Tony Payton, Jane Worthington, and Bill Ollier, who were involved in the first wave of the study, and Dr. Katia Rubia, Prof. Eric Taylor, and Dr. Edmund Sonuga Barke, who provided the neuropsychological test measures. They also thank all the families who participated in this work.
1. Thapar A, Holmes J, Poulton K, Harrington R: Genetic basis of attention deficit and hyperactivity. Br J Psychiatry 1999; 174:105–111Crossref, Medline, Google Scholar
2. Thapar A: Attention deficit hyperactivity disorder: new genetic findings, new directions, in Behavioral Genetics in the Postgenomic Era. Edited by Plomin R, Defries J, Craig I, McGuffin P. Washington, DC, American Psychological Association, 2002, pp 445–462Google Scholar
3. Faraone SV, Doyle AE, Mick E, Biederman J: Meta-analysis of the association between the 7-repeat allele of the dopamine D4 receptor gene and attention deficit hyperactivity disorder. Am J Psychiatry 2001; 158:1052–1057Link, Google Scholar
4. Ashghari V, Sanyal S, Buchwaldt S, Paterson A, Van Tol HH: Modulation of intracellular cyclic AMP levels by different human dopamine D4 receptor variants. J Neurochem 1995; 65:1157–1165Crossref, Medline, Google Scholar
5. Holmes J, Payton A, Barrett J, Harrington R, McGuffin P, Owen M, Ollier W, Worthington J, Gill M, Kirley A, Hawi Z, Fitzgerald M, Asherson P, Curran S, Mill J, Gould A, Taylor E, Kent L, Craddock N, Thapar A: Association of DRD4 in children with ADHD and comorbid conduct problems. Am J Med Genet Neuropsychiatr Genet 2000; 114:150–153Crossref, Google Scholar
6. Swanson J, Oosterlaan J, Murias M, Schuck S, Flodman P, Spence MA, Wasdell M, Ding Y, Chi H-C, Smith M, Mann M, Carlson C, Kennedy JL, Sergeant JA, Leung P, Zhang Y-P, Sadeh A, Chen C, Whalen CK, Babb KA, Moyzis RK, Posner MI: Attention deficit/hyperactivity disorder children with a 7-repeat allele of the dopamine receptor D4 gene have extreme behavior but normal performance on critical neuropsychological tests of attention. Proc Natl Acad Sci USA 2000; 97:4754–4759Crossref, Medline, Google Scholar
7. Ding Y-C, Chi H-C, Grady DL, Morishima A, Kidd JR, Kidd KK, Flodman P, Spence MA, Schuck S, Swanson JM, Zhang Y-P, Moyzis RK: Evidence of positive receptor selection acting at the human dopamine receptor D4 gene locus. Proc Natl Acad Sci USA 2002; 99:309–314Crossref, Medline, Google Scholar
8. Van de Bree M, Owen M: The future of psychiatric genetics. Ann Med 2003; 35:122–134Crossref, Medline, Google Scholar
9. Castellanos FX, Tannock R: Neuroscience of attention-deficit/hyperactivity disorder: the search for endophenotypes. Neuroscience 2002; 3:617–628Medline, Google Scholar
10. Crosbie J, Schachar R: Deficient inhibition as a marker for familial ADHD. Am J Psychiatry 2001; 158:1884–1890Link, Google Scholar
11. Malhotra AK, Kestler LJ, Mazzanti C, Bates JA, Goldberg T, Goldman D: A functional polymorphism in the COMT gene and performance on a test of prefrontal cognition. Am J Psychiatry 2002; 159:652–654Link, Google Scholar
12. Angold A, Prendergast M, Cox A, Harrington R, Simonoff E, Rutter M: The Child and Adolescent Psychiatric Assessment. Psychol Med 1995; 25:739–753Crossref, Medline, Google Scholar
13. Holmes J, Lawson D, Langley K, Fitzpatrick H, Trumer A, Pay H, Harrington R Thapar A: The Child Attention Deficit Hyperactivity Disorder Teacher Telephone Interview (CHATTI): reliability and validity findings. Br J Psychiatry (in press)Google Scholar
14. Sonuga-Barke EJS, Houlberg K, Hall M: When is impulsiveness not impulsive? the case of hyperactive children’s cognitive style. J Child Psychol Psychiatry 1994; 35:1247–1253Crossref, Medline, Google Scholar
15. Rubia K, Taylor E, Smith AB, Oksanen H, Overmeyer S, Newman S: Neuropsychological analyses of impulsiveness in childhood hyperactivity. Br J Psychiatry 2001; 179:138–143; correction, 179:272Crossref, Medline, Google Scholar
16. Corkum PV, Siegel LS: Is the Continuous Performance Task a valuable research tool for use with children with attention-deficit-hyperactivity disorder? J Child Psychol Psychiatry 1993; 34:1217–1239Crossref, Medline, Google Scholar
17. Kagan R: Reflection-impulsivity and reading ability in primary grade children. Child Dev 1965; 36:609–628Crossref, Google Scholar
18. Redmond D, Hegge F: Observations on the design and specification of a wrist-worn human activity monitoring system. Behav Res Methods Instrum Comput 1985; 17:659–669Crossref, Google Scholar
19. Thapar A, Harrington R, Ross K, McGuffin P: Does the definition of ADHD affect heritability? J Am Acad Child Adolesc Psychiatry 2000; 39:1528–1536Crossref, Medline, Google Scholar
20. Xu X, Horvath S, Laird N: The FBAT (Family Based Association Test) Program: Testing for Linkage and Association With Family Data, Version 1.2: Program for Population Genetics. Boston, Harvard School of Public Health, 2000Google Scholar
21. Okuyama Y, Ishiguro H, Toru M, Arinami T: A genetic polymorphism in the promoter region of DRD4 associated with expression and schizophrenia. Biochem Biophys Res Commun 1999; 258:292–295Crossref, Medline, Google Scholar
22. Kuntsi J, Stevenson J: Psychological mechanisms in hyperactivity, II: the role of genetic factors. J Child Psychol Psychiatry 2001; 42:211–219Crossref, Medline, Google Scholar

