
Unexpected Cause of Anxiety and Parkinsonism
To the Editor: Parkinson’s disease is characterized by resting tremor, bradykinesia, rigidity, and postural instability. Neuroimaging is usually not necessary in patients with idiopathic Parkinson’s disease unless there are atypical features, neurological deficits, or poor response to treatment (1) . Anxiety symptoms are not uncommon in Parkinson’s disease patients, and in some instances may even precede the diagnosis (2) . Hence, anxiety may be due to neurobiological abnormalities in Parkinson’s disease. Anxiety symptoms alone in a Parkinson’s disease patient would not warrant an early imaging study. We report the case of a patient who presented with excessive anxiety and features suggestive of idiopathic Parkinson’s disease. However, an imaging study unexpectedly revealed a rare cause for his parkinsonism.
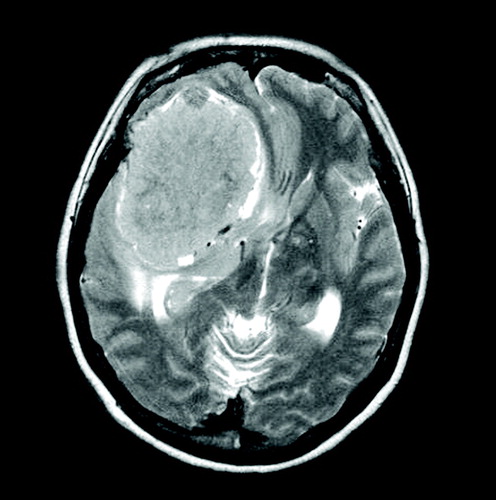
An elderly man presented with a gradual onset of left-sided resting tremor, bradykinesia, and rigidity, which progressed to involve the right-sided limbs over a few months, associated with symptoms of generalized anxiety disorder. He had palpitations, restlessness, sleep disturbance, worried excessively about daily events, and also complained of “poor concentration and memory.” However on examination, there was no evidence of impaired cognition, and his limb power, sensory modalities, and reflexes were normal. A formal neuropsychological assessment by a psychologist did not reveal any evidence of cognitive dysfunction. There were no atypical features such as gaze abnormalities or orthostatic hypotension to suggest secondary causes for his parkinsonism. The constellation of signs and symptoms of the motor system in our patient was compatible with clinical diagnostic criteria of “idiopathic” Parkinson’s disease. The patient was prescribed a course of Selegiline 5 mg per day for 2 months but subsequently discontinued receiving the medication despite subjective improvement. Because of his recent onset of anxiety symptoms, a brain magnetic resonance imaging (MRI) was carried out with the intention to reassure him. However, the scan unexpectedly revealed a large meningioma in the right frontal-temporal region with significant ventricular compression and midline shift of the brain ( Figure 1 ). The patient underwent a resection of the meningioma with resolution of his parkinsonism and anxiety symptoms.
Our case suggests that while anxiety symptoms are commonly observed in patients with Parkinson’s disease, they may also represent an early warning sign in tumour associated parkinsonism. Hence, we may have to actively exclude secondary causes of parkinsonism in patients who present with excessive anxiety or other nonmotor symptoms early in the course of the disease.
1. Polyzoidis KS, McQueen JD, Rajput AH, MacFadyen DJ: Parkinsonism as a manifestation of brain tumor. Surg Neurol 1985; 23:59–63Google Scholar
2. Richard IH: Anxiety disorders in Parkinson’s disease. Adv Neurol. 2005; 96:42–55Google Scholar

