
Delinquency and Mortality: A 50-Year Follow-Up Study of 1,000 Delinquent and Nondelinquent Boys
Abstract
OBJECTIVE: It is well established that until age 40 years, delinquent individuals have roughly twice the mortality of nondelinquent individuals and that the excess deaths are largely due to accidents, violence, and substance abuse. The present study examined if the increased mortality of delinquent subjects continues until age 65 years and, if so, why. METHOD: The authors followed 475 delinquent and 456 matched nondelinquent comparison boys from age 14 years until age 65 years. RESULTS: Thirteen percent (N=62) of the delinquent and only 6% (N=28) of the nondelinquent subjects died unnatural deaths. By age 65 years, 29% (N=139) of the delinquent and 21% (N=95) of the nondelinquent subjects had died from natural causes. In a univariate analysis, frequency of delinquency, abuse of alcohol, adult crime, dysfunctional home environment, and poor education were significantly related to death, especially to unnatural death. However, when delinquency and alcohol abuse were controlled by logistic regression, education, dysfunctional upbringing, and adult criminality made no further contributions to mortality. CONCLUSIONS: Although delinquency is strongly associated with premature mortality, the etiological links remain unclear. Alcohol abuse and poor self-care in adulthood (e.g., infections or accidents) account for most of the modest variance in mortality that could be accounted for.
Little is known about the overall mortality of those involved in persistent delinquency (i.e., multiple arrests for criminal behavior) except that before age 40 years, delinquent individuals are more likely to die from unnatural causes—accidents or homicide—than are nondelinquent individuals. Do men who experience multiple arrests in their youth continue to have higher rates of mortality as they age than do nondelinquent individuals? Are the causes of natural death different for delinquent and nondelinquent individuals? Do delinquent individuals continue to die excessively from accidents and homicide in midlife? The answers are lacking.
When we drew from a relatively limited body of literature, we found four competing hypotheses as to why delinquent individuals might have a higher death rate: 1) risk taking and impulsiveness, 2) increased substance abuse, 3) poor self-care associated with a dysfunctional upbringing, or 4) economic and educational deprivation.
First, many researchers have speculated that high-rate criminal offenders die earlier and experience more violent deaths as a direct consequence of their delinquency than do low-rate offenders (1). Such a perspective is consistent with the work of Gottfredson and Hirschi (2), who argue that the same individual trait—i.e., low self-control—accounts for the relationship of antisocial behavior to premature death and to death from accidents or homicide. For instance, in their longitudinal study of juvenile delinquency and adult crime up to age 32 years, the Gluecks (3) found that the death rate for delinquent individuals was twice that for matched nondelinquent comparison subjects. In a 30-year follow-up, Robins and O’Neal (4) found a twofold higher mortality rate for problem children with conduct disorder by age 40 years than for comparison subjects. In both studies, the twofold difference in mortality was due to a higher rate of unnatural deaths (i.e., homicide, suicide, accidents, and acute alcoholism). Since before age 40 deaths from natural causes are relatively rare, meaningful differences in such mortality could not be assessed.
Other studies that have followed delinquent boys into young adulthood have noted similar trends. Rydelius (5), in following 832 Swedish boys admitted to probationary schools, noted a death rate by age 40 of four times that expected. Two-fifths of the 110 deaths observed were from accidents, one-fifth from suicide, and only 3% from homicide. In contrast, Lattimore and co-workers (6) examined the risk of death among serious young male offenders who were paroled from the California Youth Authority and followed for 11 years. Among 1,998 subjects, they found that 109 (5.5%) had died—twice the expected rate. But in contrast to the Swedish data, 51 (47%) of these premature deaths were from homicide. The risk factors for death by homicide included minority status, residence in Los Angeles, a history of gang involvement, history of institutional violence, and history of drug arrests.
The second hypothesis has focused on the special role that alcohol, cigarettes, and drug abuse play in the elevated mortality among delinquent individuals. Drugs and alcohol abuse have appeared as leading candidates to explain the high mortality in long-term follow-up studies of heroin abusers (7). Romanov et al. (8) noted that delinquent individuals with heavy alcohol consumption (30 g or more per day) suffered a mortality rate twice that of men with less reported alcohol use. Heavy alcohol use was a more robust predictor of all causes of mortality (with the single exception of suicide) than was hostility (assessed by multiple scales). A large study (9) of young Swedish recruits noted a strong association between high alcohol consumption and premature death. In the case of delinquency, the proportion of violent deaths (suicides, homicides, and accidents) increased fivefold with the highest levels (more than 250 g per week) of alcohol consumption. Unfortunately, like other studies (4–6, 10), the previous study was a 15-year study of young adults; few subjects had yet died from cancer or heart disease. In addition, confounders like cigarette smoking and signs of delinquency (running away, school problems, and drug abuse) were also about five times more common in the group with the heaviest drinking. None of the preceding studies distinguished the risk of alcohol abuse from the severity of delinquency.
The third hypothesis, which has less experimental support, is that a lack of self-care due to a dysfunctional upbringing results in increased mortality. Psychodynamically oriented clinicians (11, 12) and other researchers (13) believe that social deprivation and parental neglect and abuse lead to poor self-care, which, in turn, result not only in antisocial behavior but also in poor health owing to covert depression and parasuicidality. Cairns and Cairns (14) have also provided suggestive evidence for a link between adolescent suicide and antisocial aggression.
Finally, the fourth hypothesis is based on the fact that low socioeconomic status, even without delinquency, leads to poor education and low job status, which, in turn, lead to chronic illness and premature mortality (15–17).
To address these four hypotheses, we took advantage of a 50-year prospective follow-up study of 1,000 socially disadvantaged Caucasian schoolboys (18). In their youth, 500 of these men had been persistent juvenile delinquents, and 500 were demographically matched nondelinquent subjects. This careful demographic matching, in effect, controlled for the well-substantiated fourth hypothesis linking low social status to premature mortality. As already noted, the delinquent subjects by age 32 were more likely to die prematurely than the nondelinquent comparison subjects (3).
To understand further the effects of delinquency on mortality after age 40, we examined the predictors of mortality, the timing of mortality, and the differential causes of death in these groups. Previously, this longitudinal study was extensively analyzed to follow the course of alcoholic (19) and criminal (20) careers, but to our knowledge this report is the first effort to contrast systematically the mortality of delinquent and nondelinquent subjects.
We continued to follow the two groups until age 65 years, and in this study we tested the first three hypotheses that any differential rates of mortality observed could be accounted for by an antisocial lifestyle, adult substance abuse, or a dysfunctional upbringing.
METHOD
Subjects
The subjects were delinquent and nondelinquent boys drawn from the Gluecks’s classic study of crime and delinquency, initiated in 1940 (18). Since 1968, the nondelinquent men have been closely followed (19). More recently, the delinquent men have also been restudied (20, unpublished reports by Laub and Sampson in 1995 and 1996).
The delinquent study group originally included 500 persistently delinquent boys aged 11–16 years who were committed to one of two Massachusetts correctional schools for boys—the Lyman School in Westboro and the Industrial School for Boys in Shirley. Approximately 30% of the delinquent group had had a juvenile court conviction by age 10 years, and by early adolescence, the average number of convictions (not just arrests) for the delinquent boys was 3.5 (18, p. 74).
The nondelinquent group, aged 11–16 years and drawn from the Boston public schools, were matched with the delinquent boys for age, ethnicity, IQ, and high-crime/low-income neighborhoods—variables thought to be critical in influencing both delinquent behavior and official reactions by the courts. One-fourth of the subjects in both groups were of English or English-Canadian descent, another one-fourth were Italian, one-fifth were Irish, and less than one-tenth were multigenerational American. The rest were Slavic, French-Canadian, Near-Eastern, Spanish, Scandinavian, German, or Jewish youth. Sixty percent of the parents were foreign born. The delinquent boys had an average IQ of 92, and the nondelinquent boys had an average IQ of 94, as measured by an individually administered Wechsler-Bellevue Test. Whether a boy met the nondelinquency criteria (met by about 80% of all inner-city students in 1940) was determined by criminal records checks and by a series of interviews with parents and teachers. After 10 years, for fiscal reasons, the youngest 7% (N=69) of the group were dropped. This left 475 delinquent and 456 nondelinquent subjects.
Measures
During an 18-year period of follow-up, from age 14 to age 32 years, the Gluecks collected multifaceted information on the delinquent and nondelinquent subjects in childhood (retrospectively), in adolescence (concurrently), and in adulthood by interviews at age 25 and 32 years (prospectively). They used a combination of official records, observations, and interviews with both the subjects and key informants (e.g., parents, teachers, spouses, military authorities, and employers). The Gluecks’s follow-up interview rate was 91% (delinquent subjects, N=432; nondelinquent subjects, N=415) for both groups at both age 25 and 32 years. Extensive data were available for analysis relating to family life, education, employment history, military experiences, recreational activities, and criminal history at each of the three interview waves.
Although the number of deaths between age 61 and 65 years may be underestimated, definite evidence of mortality or survival at age 60 years was available for 440 of 475 (93%) of the delinquent and 453 of 456 (99%) of the nondelinquent subjects. Positive evidence of survival past age 60 years was a completed questionnaire, a recent arrest, evidence of a driver’s license renewal, or a current address and telephone number. For subjects whom we could not locate in this way, we searched both the Massachusetts Registry of Vital Records before 1979, the National Death Index maintained by the National Center for Health Statistics 1979–1997, and FBI “rap sheets.” (The National Death Index is a centralized, computerized database of death records for all 50 states; it begins with deaths occurring in 1979.) We searched all sources through 1997, when all subjects would have been 65 years old.
When the subjects were age 65, death certificates were obtained for 305 of the 324 known study deaths. Information regarding the remaining deaths depended on evidence from police, relatives, or military authorities. Once a death certificate was secured, the age and cause of death were coded. The clinical record and newspaper obituaries were used to clarify ambiguities.
Dysfunctional upbringing was measured with the sum of five childhood factors: 1) uncohesive family, 2) no maternal affection, 3) no paternal affection, 4) unacceptable maternal supervision, and 5) unsatisfactory paternal discipline. These variables were the childhood variables that the Gluecks (18) found to be the best predictors of delinquency. Each of these five childhood factors was a composite constructed out of objective variables associated with multiproblem families (e.g., “known to nine or more social agencies” or “separated from both parents for more than 6 months”) (18). In childhood, each of the five factors that was present was scored 1, resulting in a possible range of 0–5.
Unofficial delinquency reports by the boy, his parents, and his teachers were summed for the presence or absence of several variables, including juvenile drinking, running away, gambling, truancy, sneaking rides, stealing autos, impulsive stealing, planned stealing, and arson. Scores from the three sources were added; they ranged from 1, indicating no misbehavior (N=196, all of whom were nondelinquent subjects), to more than 15 (N=144, all of whom were delinquent subjects).
Probable alcohol abuse was measured (0=no evidence of excessive drinking or alcohol-related arrests before age 32, 1=either excessive drinking or alcohol-related arrests, 2=both excessive drinking and alcohol-related arrests). This estimate of alcoholic abuse correlated (r=0.54, N=408, p<0.001) with a careful assessment of the lifetime prevalence of alcohol abuse (per DSM-III) for the more thoroughly studied, nondelinquent group (19).
From the official criminal history, we determined whether the subjects had arrests from age 25 to 32. Identical dichotomous variables were constructed for the delinquent and nondelinquent subjects.
Statistical Methods
We categorized deaths into those before age 40 and those from age 40 to 65. We also categorized deaths as 1) unnatural—those due to violence (suicide, homicide, or accident) and those due to poor self-care (infection or alcohol abuse) or 2) natural—deaths mostly from cancer and heart disease. We recognize that the distinction between “natural” and “unnatural” deaths can be misleading because natural deaths due to heart disease and cancer may be related to lifestyle.
Life tables and survival curves were used to contrast mortality in the two groups. Univariate risk ratios and logistic regression analyses were used to identify antecedent variables that made an independent contribution to mortality. Appropriate measures of association (e.g., gamma, Kendall’s tau) were used in these analyses; however, the results did not change when we used Pearson’s correlation. For consistency, we present only Pearson’s r throughout the text and tables. Where appropriate, all chi-square statistics were corrected for continuity.
RESULTS
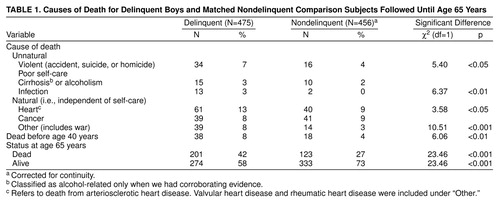
By age 65, 201 of the delinquent subjects had died, compared with only 123 of the nondelinquent comparison subjects (table 1). (U.S. Census data [21] revealed that between ages 10 and 65, 27% of the white males born in 1930 died.) Thirty-eight delinquent, but only 18 nondelinquent subjects, died before age 40 years. Perhaps more interesting is the fact that 163 delinquent subjects died between 40 and 65, compared to only 105 nondelinquent subjects (χ2=13.92, df=1, p<0.001) (table 1). Since the average age at death for the delinquent subjects was 49.2 years (SD=13.0), only slightly lower than that for nondelinquent subjects (51.6 years, SD=11.6), the trend of increased mortality among the delinquent subjects continued at least until age 65. Derived from life table methods, figure 1 displays survival curves for time until death (up until age 65 years) for the delinquent and nondelinquent groups.
Except for cancer (often cigarette-related) and cirrhosis and other alcohol-related deaths, all broad classes of illness—not just the often-cited triad of accidents, suicides, and homicides—were more likely among the delinquent boys (table 1). Overall, the leading cause of death for both groups was heart disease, but it was more frequent among the delinquent subjects.
table 2 shows that 53 of the delinquent subjects died unnatural deaths related to poor self-care—broadly defined as accidents, alcoholism, infections, and suicide—compared with only 28 of the nondelinquent subjects. Nine delinquent subjects died from homicide compared to none of the nondelinquent subjects. Among the nondelinquent subjects, death by infectious disease was as unusual as death by homicide, but 13 delinquent subjects died as a result of infections (e.g., tetanus, gangrene, lobar pneumonia, tuberculosis, and septicemia due to a urinary tract infection). In contradiction to our third hypothesis that increased mortality was due to depression and self-attack as a result of a dysfunctional upbringing, equal proportions of both groups died from suicide.
If just the deaths before age 40 years are examined, 29 delinquent and only 11 nondelinquent subjects died from violent causes or poor self-care. After age 39, this trend continued (table 2). The largest number of excess deaths, however, arose from the fact that 130 delinquent subjects, but only 88 in the comparison group, died of natural causes. In other words, if the delinquent group suffered 78 more deaths than the nondelinquent group, 54% (N=42) of these excess deaths were from natural causes between the ages of 40 and 65.
Since the two groups were roughly matched for economic deprivation but not for dysfunctional upbringing, factors other than underclass membership per se were needed to account for the differential rates of death among delinquent and nondelinquent subjects.
To quantify the individual differences in impulsivity and social deviancy that were independent of the Gluecks’s original delinquent versus nondelinquent comparison group design, we examined a composite measure of total unofficial delinquency derived from self, parent, and teacher reports for both delinquent and nondelinquent boys. The self, parent, and teacher reports correlated highly with one another (20). This scale included information on delinquent behavior (e.g., stealing and vandalism) and other misconduct (e.g., truancy and running away) not necessarily known to the police. There was a modest overlap between the groups in that 124 nondelinquent subjects exhibited unofficial delinquency scores of 4–12, as did 151 delinquent subjects (figure 2). However, only two delinquent subjects had unofficial delinquency scores under 4, and only 27% (N=124) of the nondelinquent subjects had scores over 3.
figure 2 shows the relationship between unofficial delinquent behavior before age 14 years and mortality after age 14 years. Overall, the 144 delinquent boys with high scores (range=17–26) on the unofficial delinquency scale were more than twice as likely to die (51%) as the 196 boys with no unofficial delinquency (23%). This difference remained if one studied only natural deaths: 18% of the 196 men with low delinquency scores and 36% of the 144 men with high unofficial delinquency scores died from natural causes. Equally important, however, the 124 nondelinquent subjects with modest unofficial delinquency (mean=6.0, range=4–12) were as likely to die young as the 151 delinquent subjects with modest unofficial delinquency scores (mean=9.4, range=4–12). This similarity suggests that it was delinquent behavior per se and not labeling by the courts or humiliation from reform schools that accounted for the observed variation in mortality.
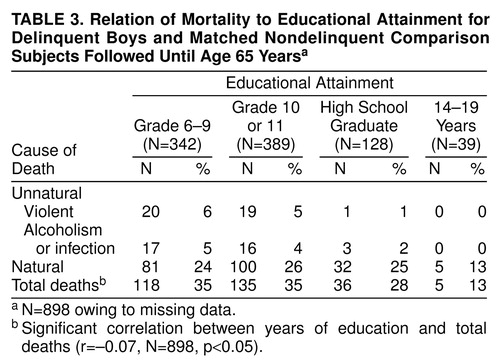
table 3 examines the effect of attained education on mortality. Substituting occupational status (15) or adult social class could account for roughly the same variance. However, since social adjustment of the delinquent subjects had been followed only until age 32 years, attained education appeared to be the most reliable objective indicator of adult social status. As expected, 12 or more years of education was protective against premature mortality, especially death from violence or poor self-care.
In trying to account for an almost twofold difference in overall mortality in both unnatural deaths and deaths from natural causes, we examined a wide range of childhood, adolescent, and adult factors. We found few significant associations. Overall, we were able to explain only a very low proportion of the variance in mortality from our independent, prospectively gathered psychosocial variables. Adult behaviors that were directly related to criminal and deviant behavior (e.g., number of arrests at ages 25 and 32 and/or alcohol abuse at ages 25 and 32) were far more likely to predict differences in mortality than were childhood and adolescent variables such as IQ (r=–0.01, N=931, p>0.86), family income (r=0.01, N=929, p>0.86), or early-onset delinquency (r=0.00, N=827, p>0.99).
table 4 demonstrates the univariate contribution of each of our most significant predictors of mortality. All five measures were significantly associated with both mortality and unnatural death. However, the matrix underscores that these variables show considerable overlap. A dysfunctional upbringing predicts delinquency, which, in turn, predicts limited education, alcohol abuse, and criminality in adult life. The association of education with mortality was less robust than the association of unofficial delinquency, alcoholism, and adult criminal behavior.
table 4 shows that, for the entire group, unofficial delinquency and alcohol abuse made independent contributions toward explaining both early mortality and unnatural death. Once these two variables were controlled, dysfunctional upbringing, education, and adult criminal behavior made no further contributions toward explaining mortality. We examined several interaction terms for our key variables and found no significant effects. Moreover, the results did not change after differences in type of crime (e.g., adult arrests for violence versus arrests for property crimes) were taken into account.
To avoid the often-hypothesized bias in group selection (22), we examined mortality within the delinquent and nondelinquent groups. A slightly different picture emerged in our logistic regression analysis. Specifically, for the delinquent subjects, only alcohol abuse was significantly related to mortality (odds ratio=1.51, 95% CI=1.21–1.81; χ2=7.31, df=1, p<0.01). For the comparison group, none of our variables was a significant predictor, although alcohol abuse was marginally significant (odds ratio=1.44, 95% CI=1.00–1.88; χ2=2.71, df=1, p<0.10). The opposite finding emerged when we examined unnatural death. For the nondelinquent subjects, only alcohol abuse was significantly related to unnatural death (odds ratio=3.22, 95% CI=2.41–4.03, χ2=7.91, df=1, p<0.01), whereas for the delinquent subjects, none of our variables was a significant predictor, even at the p<0.10 level. This is consistent with further analyses of the better-studied nondelinquent group. When alcohol abuse was controlled, dysfunctional upbringing, years of education, number of times in jail, and unofficial delinquency made no further contributions toward explaining mortality.
DISCUSSION
Although our group selection serendipitously controlled for the confounders of gender, race, illegal drugs (virtually absent in 1950–1960 Boston), and social class, the relationship between antisocial behavior and death is not a simple one. Whether poor self-care and premature health decline are caused more by childhood deprivation and poor self-worth or by impulsivity and/or by substance abuse was not answered with certainty. For example, alcohol abuse, impulsivity, and limited education are each correlated with the failure to stop smoking (unpublished report by Vaillant et al.). To which of these hypothetical causes should we attribute deaths from heart disease and lung cancer secondary to smoking? Nevertheless, we were able to conclude that many important childhood predictors of delinquency were not predictors of death. For example, IQ, family poverty, and early-onset delinquency were not related to death; moreover, key familial risk factors for delinquency (e.g., poor parental supervision, inconsistent discipline, and weak parent-child attachment) were only modestly related to death.
Admittedly, besides being narrowed to a 1930 birth cohort and consisting only of Caucasians, the study has several further limitations. First, owing to the incomplete data on the delinquent group, we could not control for smoking. In the nondelinquent comparison group, if smoking was included in the logistic regression model of table 5, none of the other variables predicted mortality except alcohol dependence (weakly). Second, we also did not control for genetic predisposition to delinquency or premature mortality. Third, we did not control for access to medical care and, perhaps more important, for compliance once it was attained. (It may be that antisocial individuals are less likely to seek or be able to afford optimal medical care and to comply with medical regimens.) Fourth, the importance of education may be underestimated because in this group the range of education was highly truncated, especially in the delinquent group. For example, only 2% (N=9) of the delinquent subjects graduated from high school (20, p. 132). A final limitation was that we probably missed a few deaths among the more difficult-to-follow delinquent subjects.
The study most comparable to ours is that by Stattin and Romelsjo (23). The authors examined all three hypotheses: social deprivation, adolescent antisocial behavior, and subsequent substance abuse. Data were drawn from 7,577 male Swedish conscripts who were followed until age 33 years. The authors found that early experience with police, truancy, and school misconduct were significant predictors of premature mortality. However, the data were consistent with the second hypothesis in that they noted that the relationship between criminal activity and death could be explained in large part by “the existence of a small group of alcohol and/or drug abusers who run a high risk of dying prematurely” (23, p. 280). Unfortunately, they failed to follow their subjects into later life, when mortality is more common. Their data also offered support for the third hypothesis—namely, in addition to delinquent subjects’ early conduct problems and drug abuse, dysfunctional families were also significant and independent predictors of mortality by age 33. They concluded that theories that offer a common set of factors to explain both criminality and mortality are too general and not useful for public policy. This is consistent with the relatively low univariate correlations that we found even among our most significant variables in table 4.
Others have come to the same conclusion. Farrington (24) investigated the relationship between criminal offending and physical health, including physical illnesses, injuries, accidents, and hospital treatment, with data from the Cambridge Study in Delinquent Development. He found no childhood factors that predicted both offending and physical health. In short, he found little support for the third hypothesis that there are common, early childhood causes of juvenile offending and adult illness. In a similar vein, Yeager and Lewis (25) found that none of the biopsychosocial variables that distinguished violent from nonviolent offenders helped explain subsequent mortality.
In summary, although juvenile antisocial behavior, alcohol abuse, adult criminal behavior, family upbringing, and education may each be associated with premature death, the magnitude of these relationships is quite modest. In multivariate analyses, the strongest predictors of death were juvenile antisocial behavior and alcohol abuse. In addition, delinquent subjects were particularly likely to die from homicide and poor self-care. In studies using more recent cohorts, the rate of death from illegal drugs among delinquent groups was much higher. (Surprisingly, death from lung cancer—often linked to cigarette abuse—was equally elevated in both of our groups.) Our study suggests that part of the explanation for the observed twofold difference in mortality for delinquents may be owing more to proximal unhealthy behaviors (e.g., alcohol abuse) rather than childhood and adolescent variables like education, dysfunctional upbringing, and even adolescent delinquency. We need further research on the predictors of sustained healthy and/or unhealthy lifestyles.
Received June 26, 1998; revisions received Nov. 23, 1998, and April 2 and June 16, 1999; accepted July 12, 1999. From the Department of Criminology and Criminal Justice, University of Maryland at College Park; the Henry A. Murray Research Center, Radcliffe College, Cambridge, Mass.; the Department of Psychiatry, Brigham and Women’s Hospital; and the Study of Adult Development, Harvard University Health Services, Cambridge, Mass. Address reprint requests to Dr. Vaillant, Department of Psychiatry, Brigham and Women’s Hospital, 75 Francis St., Boston, MA 02115. Supported by NIMH grant MH-42248 and the Harry Frank Guggenheim Foundation.
 |
 |
 |
 |
 |

FIGURE 1. Survival Rates for 475 Delinquent and 456 Matched Nondelinquent Comparison Subjects Followed Until Age 65 Years

FIGURE 2. Relation of Mortality to Unofficial Adolescent Delinquency for 475 Delinquent and 456 Matched Nondelinquent Comparison Subjects Followed Until Age 65 Years
aIncludes three nondelinquent subjects with scores greater than 12.
bIncludes two delinquent subjects with scores less than 4.
1. Reiss AJ Jr: Ending criminal careers, prepared for the Final Report of the “Desistance/Persistence Working Group” of the Program on Human Development and Criminal Behavior. Washington, DC, MacArthur Foundation and National Institute of Justice, 1989Google Scholar
2. Gottfredson M, Hirschi T: A General Theory of Crime. Stanford, Calif, Stanford University Press, 1990Google Scholar
3. Glueck S, Glueck E: Delinquents and Nondelinquents in Perspective. Cambridge, Mass, Harvard University Press, 1968Google Scholar
4. Robins LN, O’Neal P: Mortality, mobility, and crime: problem children thirty years later. Am Sociol Rev 1958; 23:162–171Crossref, Google Scholar
5. Rydelius PA: The development of antisocial behaviour and sudden violent death. Acta Psychiatr Scand 1988; 78:398–403Crossref, Google Scholar
6. Lattimore PK, Linster RL, MacDonald JM: Risk of death among serious young offenders. J Res Crime and Delinquency 1997; 34:187–209Crossref, Google Scholar
7. Vaillant GE: A 20-year follow-up of New York narcotic addicts. Arch Gen Psychiatry 1973; 29:237–241Crossref, Medline, Google Scholar
8. Romanov K, Hatakka M, Keskinen E, Laaksonen H, Kaprio J, Rose RJ, Koskenvuo M: Self-reported hostility and suicidal acts, accidents and accidental deaths: a prospective study of 21,443 adults aged 25–59. Psychosom Med 1994; 56:328–336Crossref, Medline, Google Scholar
9. Andreasson S, Allebeck P, Romelsjo A: Alcohol and mortality among young men: longitudinal study of Swedish conscripts. Br Med J 1988; 296:1021–1025Google Scholar
10. Abel EL, Zeidenberg P: Age, alcohol, and violent death: a postmortem study. J Stud Alcohol 1985; 46:228–231Crossref, Medline, Google Scholar
11. Bowlby J: Pathological mourning and childhood mourning. J Am Psychol Assoc 1963; 11:500–541Crossref, Medline, Google Scholar
12. Menninger K: Man Against Himself. New York, Harcourt Brace, 1938Google Scholar
13. Junger M: Accidents, in The Generality of Deviance. Edited by Hirschi T, Gottfredson MR. New Brunswick, NJ, Transaction Publications, 1994, pp 81–112Google Scholar
14. Cairns RB, Cairns BD: Lifelines and Risks: Pathways of Youth in Our Time. Cambridge, UK, Cambridge University Press, 1994Google Scholar
15. Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, White I, Brunner E, Feeney A: Health inequalities among British civil servants: the Whitehall II study. Lancet 1991; 337:1387–1393Google Scholar
16. Guralnik JM, Land KC, Blazer D, Fillenbaum GG, Branch LG: Educational status and active life expectancy among older blacks and whites. N Engl J Med 1993; 329:110–116Crossref, Medline, Google Scholar
17. Pappas G, Queen S, Hadden W, Fisher G: The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. N Engl J Med 1993; 329:103–109Crossref, Medline, Google Scholar
18. Glueck S, Glueck E: Unraveling Juvenile Delinquency. New York, Commonwealth Fund, 1950Google Scholar
19. Vaillant GE: The Natural History of Alcoholism, Revisited. Cambridge, Mass, Harvard University Press, 1995Google Scholar
20. Sampson RJ, Laub JH: Crime in the Making: Pathways and Turning Points Through Life. Cambridge, Mass, Harvard University Press, 1993Google Scholar
21. Vital Statistics of the United States—1988, vol II: Mortality, Part A. Washington, DC, US Department of Health and Human Services, Public Health Service, 1988Google Scholar
22. Reiss AJ Jr: Unraveling juvenile delinquency, II: an appraisal of research methods. Am J Sociol 1951; 57:115–120Crossref, Google Scholar
23. Stattin H, Romelsjo A: Adult mortality in the light of criminality, substance abuse, and behavioural and family-risk factors in adolescence. Criminal Behaviour and Ment Health 1995; 5:279–311Crossref, Google Scholar
24. Farrington DP: Crime and physical health: illnesses, injuries, accidents, and offending in the Cambridge study. Criminal Behaviour and Ment Health 1995; 5:261–278Crossref, Google Scholar
25. Yeager CA, Lewis DO: Mortality in a group of formerly incarcerated juvenile delinquents. Am J Psychiatry 1990; 147:612–614Link, Google Scholar

