
Maternal Smoking During Pregnancy and Risk of Criminal Behavior Among Adult Male Offspring in the Northern Finland 1966 Birth Cohort
Abstract
OBJECTIVE: The goal of this study was to test the hypothesis that maternal smoking during pregnancy is associated with greater risk for criminal behavior of the offspring in adulthood. METHOD: An unselected, general population cohort composed of 11,017 subjects (5,636 men, 5,381 women) was followed up prospectively from the sixth month of pregnancy to age 28 years. Interviews with the mother during the pregnancy, health records, and an assessment of the offspring at age 1 year provided information on risk factors. The Ministry of Justice provided information on criminal offenses for all subjects. RESULTS: Because of the low rate of criminal offenses among women, the present analyses are restricted to men (N=5,636). Compared to the sons of mothers who did not smoke, the sons of mothers who smoked during pregnancy had more than a twofold risk of having committed a violent crime or having repeatedly committed crimes, even when other biopsychosocial risk factors were controlled. While maternal smoking during pregnancy alone explained 4% of the variance associated with violent offenses among male offspring, it was not significantly associated with nonviolent offenses among male offspring. When maternal smoking during pregnancy was combined with a maternal age of less than 20 years, a single-parent family, an unwanted pregnancy, and a developmental lag in walking or talking, the odds ratios for violent offenses increased up to ninefold and for persistent offenses up to 14-fold. CONCLUSIONS: Maternal smoking during pregnancy is associated with violent offenses and persistent offenses, but not with nonviolent offenses, among male offspring in adulthood.
Maternal smoking during pregnancy has been found to be associated with conduct disorder (1), attention deficit hyperactivity disorder (2), and juvenile delinquency (3) among male offspring. In turn, conduct disorder, attention deficit disorder, and delinquency during adolescence have all been found to be highly predictive of criminal offenses during adulthood (4, 5). In addition, obstetrical complications, in combination with a negative maternal attitude toward the pregnancy and an adverse early-childhood environment, have been found to be associated with later criminal behavior (6–11). Data from the Danish perinatal project, with over 9,000 subjects, suggest that the prevalence of aggressive behavior is highest among those individuals who experienced both perinatal complications and broken families (12). Using the same cohort, Raine et al. (8) found a highly significant relationship between violent offenses at age 18 and a combination of birth complications and early maternal rejection among male subjects. Neither maternal rejection nor birth complications alone were related to violent offenses. These factors, alone or in combination, were unrelated to nonviolent offenses. To further examine this issue, Raine et al. (13) randomly selected approximately 10% (N=397) of the male subjects in the original birth cohort for a follow-up study. Cluster analyses indicated that those with both early neuromotor deficits and unstable family environments had crime rates twice as high as those of the groups with only early neuromotor deficits or only unstable families. The group that had experienced both neuromotor deficits and unstable families in early childhood was characterized at the end of adolescence not only by higher rates of criminal behavior but also by more behavior and academic problems.
Thus far, no data have been published on the association between maternal smoking during pregnancy and criminality and psychobehavioral dysfunction among adult offspring. Further, the effect on the adult offspring of maternal smoking during pregnancy, in combination with other risk factors for offenses, has not been explored. The present study tested the hypothesis that maternal smoking during pregnancy, either alone or combined with other risk factors (sociodemographic characteristics of the family of origin, pregnancy and birth complications, developmental lags, and early family environment), is associated with a higher risk of nonviolent offenses, violent offenses, and persistent offenses in adulthood among male subjects.
METHOD
The Northern Finland 1966 Birth Cohort is an unselected, general population birth cohort ascertained during mid-pregnancy that includes 96% of all births (N=12,058) in the provinces of Lapland and Oulu during the year 1966. Before age 16, 284 subjects had died and 757 had left the country. The present study included 5,636 male subjects who were alive and living in Finland at the age of 16. The description of the cohort and the data collected prospectively from the sixth month of pregnancy up to age 28 have been described in detail earlier (14–16). Obstetrical variables were coded from hospital files. The mother was interviewed through use of a standardized protocol (17, 18) during her first visit to a prenatal clinic, at the time of the child’s birth, and during the child’s 1-year visit to a perinatal clinic, when the child’s development was assessed.
Data were collected from two sources: records of admissions to the children’s hospitals in the area during the years 1966 to 1972 and the Finnish Hospital Discharge Register thereafter.
It has been noted that the relationship between maternal smoking and behavior problems in offspring could be a false correlate of a causal relationship between characteristics (e.g., antisocial or psychopathological features) of women who smoke during pregnancy and behavioral problems in their children (3, 19, 20). As noted by Wakschlag et al. (1), the following four categories of risk factors for deviant behavior must be controlled to obtain evidence of a direct association between maternal smoking during pregnancy and conduct problems (or later criminality) in the offspring: demographic factors, parental mental disorders such as antisocial personality disorder, pregnancy and birth complications, and family and parenting.
In the present study, sociodemographic factors included the father’s socioeconomic status, the mother’s level of education, and family residence (urban, rural) at the time of the child’s birth. Pregnancy and birth variables included the mother’s smoking behavior (none, stopped before pregnancy, smoked daily during the entire duration of the pregnancy), the mother’s attitude toward the pregnancy (wanted the pregnancy, wanted the pregnancy later but not now, did not want the pregnancy), and the mother’s mood during pregnancy (as usual, felt depressed, felt very depressed). Obstetrical complications included low birth weight (less than 2,500 g), short gestation period (less than 37 weeks), perinatal brain damage, neonatal convulsions, neonatal asphyxia, and brain injury or intraventricular hemorrhage. Family and parenting risk factors included number of parents (two or one) (in some analyses single-parent families were divided into those in which there was one parent only at birth versus those in which there was one parent during the child’s upbringing and into those that were single-parent because of divorce or death of the other parent), number of children in the family (three or fewer, four or more), and the mother’s age (less than 20 years) at the time of the subject’s birth.
When the child was 1 year old, his motor development (walking without support at 10 months, 11 months, 12 months, after 13 months of age) was examined in a perinatal clinic by public health nurses and general practitioners. Speech development (no words, 1–2 words, 3–10 words, 11–20 words, over 20 words) was also examined at that time.
Data on criminal behavior to the end of 1992 were collected from computerized files maintained by the Ministry of Justice. This national register includes records of all crimes committed anywhere in Finland. The category of violent crimes includes homicide, assault, robbery, arson, sexual crime, and violation of domestic peace. All other crimes were defined as nonviolent. The prevalence of criminal offenders among the 5,636 male subjects at age 28 was 8.9% (2.9% for violent offenses, 6.0% for nonviolent offenses). Of all subjects who had committed violent offenses, 71.5% had also committed one or more nonviolent offenses, and 36.0% were recidivists. Of the recidivists, 49.7% had committed at least one violent offense.
Data on maternal smoking were available from the mothers of 5,514 boys. Because of missing data for other predictor variables, only 3,883 male subjects with complete data (70.4% of 5,514) were included in the logistic regression analyses. Of the men for whom complete data were available, 8.2% had a criminal record, as compared to 10.5% of the subjects with missing data. Three separate logistic regression analyses (21) were conducted in order to examine the association between criminality and maternal smoking during pregnancy after adjustment for pre- and perinatal factors, psychosocial factors, and neuromotor development. The dependent variables for the logistic regressions were 1) one conviction for a violent crime versus no record of criminal behavior, 2) a conviction for at least one nonviolent offense versus no record of criminal behavior, and 3) two or more convictions versus no record of criminal behavior. In order to explore the effect of maternal smoking during pregnancy on offenses in combination with other risk factors for offenses, odds ratios were calculated for violent, nonviolent, and persistent offenses for subjects characterized by various combinations of risk factors. Cross-tabulations with chi-square tests or Fisher’s exact tests, as appropriate, were used in assessing relationships among nominal variables.
RESULTS
At the age of 1 year, 91.1% (N=4,675) of the male subjects with no criminal record at age 28 and 87.7% (N=441) with a criminal record had visited the perinatal clinic (χ2=6.34, df=1, p=0.01). Of the subjects with complete data (N=3,883), 14.1% (N=522) of the mothers of noncriminal male offspring had smoked during pregnancy, compared with 26.0% (N=84) of the mothers of male offspring with a criminal record. Of those with missing data for some study variables (N=1,631), 12.8% (N=185) of the mothers of noncriminal male offspring, compared to 22.8% (N=39) of the mothers of male offspring with a criminal record, had smoked during pregnancy. Among male subjects with complete data, the prevalence of smoking among the mothers of those with a criminal record was 1.79 times that of mothers of subjects with no criminal record. In the group with missing data, the corresponding ratio was 1.78. (There was no significant difference between the groups with complete and missing data.)
Whereas more of the mothers of the criminals than the noncriminals had smoked during the pregnancy, the results of the univariate analyses suggested a more specific relationship. Whereas 14.1% (N=707) of the mothers of nonoffenders had smoked during the pregnancy, this was true of 21.1% (N=70) of the mothers of exclusively nonviolent offenders, 33.1% (N=53) of the mothers of violent offenders, and 31.4% (N=55) of the mothers of recidivists.
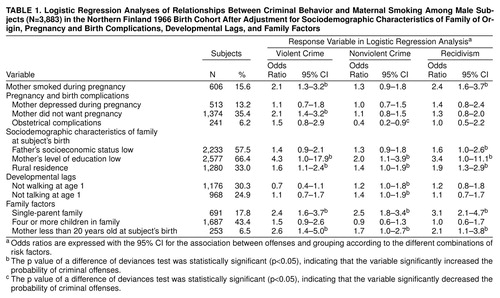
In order to test the strength of these associations, three logistic regressions were conducted. The relationship of the mother’s smoking during pregnancy to violent, nonviolent, and persistent offenses was examined, with control for the father’s socioeconomic status, the mother’s level of education, the child’s residence, whether the mother wanted the pregnancy, gestational age and birth weight, birth complications, speech and walking ability at 1 year of age, family type, parity (number of children in the family), and the mother’s age at the time of birth. The results of these analyses are presented in Table 1. Mothers who smoked during pregnancy were twice as likely as those who did not smoke to have a son who committed at least one violent crime (χ2=10.6, df=1, p=0.001) or who committed more than one offense (χ2=17.2, df=1, p<0.0001) before the age of 28. Maternal smoking during pregnancy increased the child’s risk of violent offenses by 4% (attributable risk fraction), but it was not significantly associated with nonviolent offenses.
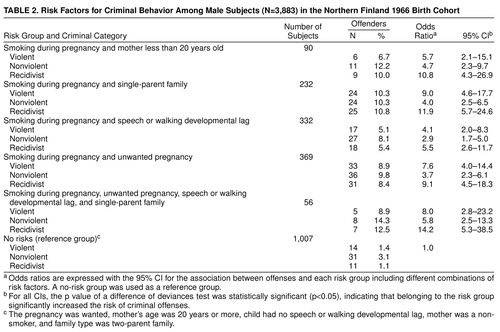
Descriptive analyses indicated that many of the sons of mothers who smoked during the pregnancy had also been exposed to other risk factors for offenses. In order to explore the effects of these combinations of risk factors, further analyses were undertaken. A risk factor was defined as a factor that significantly increased the odds of nonviolent, violent, or persistent offenses. These factors were maternal age less than 20 years at the child’s birth, single-parent family, lag in speech or walking development at age 1 year, and negative maternal attitude toward the pregnancy. As shown in Table 2, 90 men had mothers who smoked while pregnant and who were less than 20 years old at the time of their birth; 232 men had mothers who smoked while pregnant and who lived alone; 332 men had mothers who smoked while pregnant, and they had exhibited developmental lags at 1 year of age; and 56 men had mothers who smoked while pregnant, were less than 20 at the time of their birth, and lived alone, and they themselves had exhibited a developmental lag at 1 year of age. These four risk groups were compared to a reference group composed of 1,007 men whose mothers were not characterized by any of the four risk factors and whose neuromotor development at 1 year of age was within the normal range. Table 2 presents the results of these analyses with multiple risk factors. Maternal smoking during pregnancy, combined with a maternal age of less than 20, single-parent family, speech or walking developmental lag, or unwanted pregnancy, increased the odds ratios for violent crimes up to ninefold and for recidivism up to 14-fold. However, maternal smoking during pregnancy, together with one or more other biopsychosocial variables, increased the risk for nonviolent criminal behavior to a lesser degree (odds ratios=2.9–5.8).
DISCUSSION
In this study, the relationship between maternal smoking during pregnancy and violent and nonviolent criminal offenses by the male offspring in adulthood was examined for the first time. Findings obtained from 3,883 male subjects indicate that maternal smoking during pregnancy is associated with greater risk for violent offenses and for persistent offenses in adulthood but not for nonviolent offenses. In Finland, repeated serious violent offenses have been found to be strongly associated with antisocial personality disorder and alcoholism (22, 23). Since all of those adult subjects with severe antisocial behavior would have had conduct disorder in childhood or adolescence, our results are consistent with those of Wakschlag et al. (1), who observed that maternal smoking during pregnancy significantly increases the risk of conduct disorder among children. Both antisocial personality disorder (the adulthood manifestation) and conduct disorder (the childhood manifestation) are characterized by impulsivity, sensation seeking, or both. Impulsivity and sensation seeking are thought to be associated with low serotonergic brain activity (24, 25). Data from animal studies suggest that maternal smoking during pregnancy leads to reduced serotonin uptake (26) and alterations in the dopaminergic neurons in the fetal brain (27, 28). One possible explanation for our finding that maternal smoking during pregnancy increases the rate of violent offenses in male offspring as adults may be altered central nervous system monoamine function. This highly speculative hypothesis is further supported by findings of stable low levels of serotonin in the CSF of male adolescents diagnosed with conduct disorder (29) and in violent male offenders who are diagnosed with antisocial personality disorder (30, 31).
Another possible explanation for the study findings is that nicotine enhances dopamine release in the brain, especially in the nucleus accumbens and the ventral tegmental area (32). Data from an animal study indicate that aggressive behavior is associated with increased dopamine activity of the brain (33), and results from a recent study of schizophrenic patients imply that catechol-O-methyltransferase (an important enzyme in dopamine metabolism) gene polymorphism is associated with violent behavior (34). Since both nicotine and alcohol activate the dopaminergic system in the brain, it is possible that modulation of the common neurobiologic pathway of these psychoactive agents might explain why certain individuals who smoke (who have genetic factors in common with their mothers who smoke) are predisposed to alcoholism and violent criminal behavior. Epidemiological studies suggest that about 70% of recidivistic offenders committing the most severe offenses in Finland are type 2 alcoholics (22, 23), which implies that alcohol abuse may be a link between disturbed neuronal development and violent offenses.
This study also confirmed the previous findings from a smaller sample that male subjects characterized by early neuromotor deficits and maternal rejection were more likely to offend in adulthood than those with neither or only one risk factor (8, 11, 13). The results of the present investigation extend the previous findings by showing that the risk for violent offense and for recidivism increases up to 14-fold if these factors are combined with maternal smoking during pregnancy, which corresponds to a 13% prevalence for violent offenses and a 16% prevalence for persistent offenses in the high-risk groups. Further, the results of the present study indicate that maternal smoking during pregnancy, the mother not wanting the child, obstetrical complications, and the child not walking at 1 year of age significantly distinguished the violent and nonviolent male offenders.
This study presents other new findings. A single-parent family of origin doubled the risk for offenses among adult male subjects. The increase in risk was not modified by the duration of the single-parent status (during pregnancy or all the time) or by the reason for it (parental death, divorce). The father’s low socioeconomic status at the time of the child’s birth was associated with a higher rate of offenses among the male offspring but not as strongly as was the single-parent family type. The percentage of unwanted pregnancies among the mothers of the cohort members was high. In the total cohort, it was 36.7%. This may due to cultural and religious factors and the infrequent use of contraception in Northern Finland during the 1960s. Pregnancy and birth complications and developmental lags in walking and talking were not by themselves associated with criminal behavior, except for maternal smoking during pregnancy, which was directly associated with violent offenses and recidivism.
The present study is characterized by a number of strengths and weaknesses. One of the strengths is that an unselected birth cohort was followed from the sixth month of pregnancy prospectively to age 28. Information on the mother during the pregnancy, on the pregnancy and delivery, and on the offspring’s development was collected prospectively. Those evaluating the mothers and their offspring had no knowledge of the present study. Further, the mothers and their offspring were provided with high-quality perinatal care and health care and extensive social services throughout the 28 years of the study. Information on the dependent variables—violent, nonviolent, and persistent offenses—was available for all cohort members. Weaknesses include subject attrition—only 70.9% of the male subjects originally in the cohort had complete data and could therefore be entered into the regression analyses. However, analyses indicated that this attrition did not bias the remaining cohort as relates to any of the variables included in the present study. Unfortunately, the only variable that measured parental mental illness was the mother’s self-reported mood during pregnancy. Further studies should address in greater detail the combined effect of parental mental disorders and maternal smoking on the offspring’s criminality. In particular, woman who display a stable pattern of antisocial behavior may be more likely to disregard the advice of midwives and physicians regarding care of themselves during the pregnancy and care of their child. Finally, the measures of developmental lag (walking and talking) were taken when the subjects were 12 months old. This is probably too early for a valid assessment of developmental lags indicative of neuromotor abnormality. In addition, the absence of an association between violent criminality and obstetrical complications alone may be due to the small number of subjects with any obstetrical complications. For example, of the subjects who had committed crimes, only 8.8% had a gestational age under 37 weeks, 3.4% had a birth weight less than 2500 g, and 0.8% suffered from brain damage. In Finland, health care during pregnancy and delivery is excellent in both quality and quantity, free, and universally accessible, resulting in one of the lowest rates of birth complications in the industrialized world (35). The results suggest that criminality and other behavioral problems could be reduced in countries such as Finland that have relatively low crime rates by developing intervention programs for pregnant young women who smoke, are single, and who do not want their babies.
Received May 22, 1998; revision received Oct. 21, 1998; accepted Jan. 20, 1999. From the Department of Psychiatry and Department of Public Health Science and General Practice, University of Oulu, Oulu, Finland; Department of Epidemiology and Public Health, Imperial College, School of Medicine, London, England; Department of Psychology, University of Montréal, Québec, Canada; and Department of Forensic Psychiatry, University of Kuopio, Niuvanniemi Hospital, and Department of Clinical Physiology, Kuopio University Hospital, Finland. Address reprint requests to Dr. Tiihonen, Department of Forensic Psychiatry, University of Kuopio, Niuvanniemi Hospital, FIN-70240 Kuopio, Finland; [email protected] (e-mail)
 |
 |
1. Wakschlag LS, Lahey BB, Loeher R, Green SM, Gordon RA, Leventhal BL: Maternal smoking during pregnancy and the risk of conduct disorder in boys. Arch Gen Psychiatry 1997; 54:670–676Crossref, Medline, Google Scholar
2. Milberger S, Biederman J, Faraone SV, Chen L, Jones J: Is maternal smoking during pregnancy a risk factor for attention deficit hyperactivity disorder in children. Am J Psychiatry 1996; 153:1138–1142Google Scholar
3. Rantakallio P, Läärä E, Isohanni M, Moilanen I: Maternal smoking during pregnancy and delinquency of the offspring: An association without causation? Int J Epidemiol 1992; 21:1106–1113Google Scholar
4. Farrington DP, Loeber R: Transatlantic replicability of risk factors in the development of delinquency, in Historical and Geographical Influences on Psychopathology. Edited by Cohen P, Slomkowski C, Robins LN. Mahwah, NJ, Lawrence Erlbaum Associates, 1999, pp 1–50Google Scholar
5. Stattin H, Magnusson D: Onset of official delinquency: its co-occurrence in time with educational, behavioural, and interpersonal problems. Br J Criminol 1995; 35:417–449Crossref, Google Scholar
6. Denno DW: Biology and Violence: From Birth to Adulthood. New York, Cambridge University Press, 1990Google Scholar
7. Levine MD, Karniski WM, Palfrey JS, Meltzer LJ, Fenton F: A study of risk complexes in early adolescent delinquency. Am J Dis Child 1985; 139:50–56Medline, Google Scholar
8. Raine A, Brennan P, Mednick SA: Birth complications combined with early maternal rejection at age 1 year predispose to violent crime at age 18 years. Arch Gen Psychiatry 1994; 51:984–988Crossref, Medline, Google Scholar
9. Kandel E, Mednick SA: Perinatal complications predict violent offending. Criminology 1991; 29:519–529Crossref, Google Scholar
10. Rantakallio P, Moilanen I, Isohanni M: Perhetaustan yhteys nuoren miesten rikollisuuteen (Family background and juvenile crime). Sosiaalilääketieteellinen Aikakausilehti 1992; 29:13–20 (Finnish)Google Scholar
11. Raine A, Brennan P, Mednick SA: Interaction between birth complications and early maternal rejection in predisposing individuals to adult violence: specificity to serious, early-onset violence. Am J Psychiatry 1997; 154:1265–1271Google Scholar
12. Baker RL, Mednick BR: Long-term consequences for adolescent identified as at-risk at birth, in Influences on Human Development: A Longitudinal Perspective. Edited by Mednick SA. Boston, Nijhoff, 1984, pp 143–179Google Scholar
13. Raine A, Brennan P, Mednick B, Mednick SA: High rates of violence, crime, academic problems, and behavioral problems in males with both early neuromotor deficits and unstable family environments. Arch Gen Psychiatry 1996; 53:544–549Crossref, Medline, Google Scholar
14. Rantakallio P: The unwanted child. Acta Universitatis Ouluensis, Series D Medica, Number 8, 1974, pp 1–46Google Scholar
15. Rantakallio P: The longitudinal study of the Northern Finland birth cohort of 1966. Paediatr Perinat Epidemiol 1988; 2:59–88Crossref, Medline, Google Scholar
16. Myhrman A, Rantakallio P, Isohanni M, Jones P, Partanen U: Unwantedness of a pregnancy and schizophrenia in the child. Br J Psychiatry 1996; 169:637–640Crossref, Medline, Google Scholar
17. Rantakallio P, Jones P, Moring J, vonWendt L: The association between central nervous system infections during childhood and adult onset schizophrenia and other psychoses: a 28-year follow-up. Int J Epidemiol 1997; 26:837–843Crossref, Medline, Google Scholar
18. Järvelin MR, Läärä E, Rantakallio P, Moilanen I, Isohanni M: Juvenile delinquency: education and mental disability. Except Child 1994; 61:230–241Crossref, Google Scholar
19. Makin J, Fried P, Watkinson B: A comparison of active and passive smoking during pregnancy: long-term effects. Neurotoxicol Teratol 1991; 13:5–12Crossref, Medline, Google Scholar
20. Weitzman M, Gortmaker S, Sobol A: Maternal smoking and behavior problems of children. Pediatrics 1992; 90:342–349Medline, Google Scholar
21. Norusis MJ: SPSS Advances Statistics 6.1. Chicago, SPSS, 1994Google Scholar
22. Tiihonen J, Hakola P: Psychiatric disorders and homicide recidivism. Am J Psychiatry 1994; 151:436–438Link, Google Scholar
23. Eronen M, Hakola P, Tiihonen J: Factors associated with homicide recidivism in a 13-year sample of homicide offenders in Finland. Psychiatr Serv 1996; 47:403–406Link, Google Scholar
24. Schalling D: Neurochemical correlates of personality disorders with habitual violence and impulsivity, in Mental Disorder and Crime. Edited by Hodgins S. Newbury Park, Calif, Sage Publications, 1993, pp 208–226Google Scholar
25. Klinteberg BA: Biology and personality: findings from a longitudinal project, in Psychopathy: Theory, Research and Implications for Society. Edited by Cooke DJ, Forth AE, Hare RD. Dordrecht, The Netherlands, Kluwer Academic, 1998, pp 139–160Google Scholar
26. King J, Davila-Garcia M, Azmitia E, Strand F: Differential effects of prenatal and postnatal ACTH or nicotine exposure on 5-HT high affinity uptake in the neonatal rat brain. Int J Dev Neurosci 1991; 9:281–286Crossref, Medline, Google Scholar
27. Richardson S, Tizabi Y: Hyperactivity in the offspring of nicotine-treated rats: role of the mesolimbic and nigostriatal dopaminergic pathways. Pharmacol Biochem Behav 1994; 47:331–337Crossref, Medline, Google Scholar
28. Fung Y, Lau Y: Effects of prenatal nicotine exposure on rat striatal dopaminergic and nicotinic systems. Pharmacol Biochem Behav 1989; 33:1–6Crossref, Medline, Google Scholar
29. Kruesi MJP, Hibbs ED, Zahn TP, Keysor CS, Hamburger SD, Bartko JJ, Rapoport JL: A 2-year prospective follow-up study of children and adolescents with disruptive behavior disorders. Arch Gen Psychiatry 1992; 49:429–435Crossref, Medline, Google Scholar
30. Virkkunen M, Kallio E, Rawlings R, Tokola R, Poland RE, Guidotti A, Nemeroff C, Bissette G, Kalogeras K, Karonen S-L, Linnoila M: Personality profiles and state aggressiveness in Finnish alcoholic, violent offenders, fire setters and healthy volunteers. Arch Gen Psychiatry 1994; 51:28–33Crossref, Medline, Google Scholar
31. Virkkunen M, Rawlings R, Tokola R, Poland RE, Guidotti A, Nemeroff C, Bissette G, Kalogeras K, Karonen SL, Linnoila M: CSF biochemistries, glucose metabolism and diurnal activity rhythms in alcoholic, violent offenders, fire setters and healthy volunteers. Arch Gen Psychiatry 1994; 51:20–27Crossref, Medline, Google Scholar
32. Noble EP: The DRD2 gene, smoking, and lung cancer. J Natl Cancer Inst 1998; 90:343–345Crossref, Medline, Google Scholar
33. Lycke E, Modigh K, Roos BE: Aggression in mice associated with changes in the monoamine-metabolism of the brain. Experimentia 1969; 25:951–953Crossref, Medline, Google Scholar
34. Lachman HM, Nolan KA, Mohr P, Saito T, Volavka J: Association between catechol O-methyltransferase genotype and violence in schizophrenia and schizoaffective disorder. Am J Psychiatry 1998; 155:835–837Abstract, Google Scholar
35. Official Statistics of Finland: Statistical Yearbook of Finland 1995, volume 90. Helsinki, Official Statistics of Finland, 1995Google Scholar

