
Decreased Caudate Volume in Neuroleptic-Naive Psychotic Patients
Abstract
OBJECTIVE: Previous studies, mostly involving neuroleptic-treated patients, have suggested enlarged basal ganglia size in schizophrenia. The authors sought to examine basal ganglia volume in neuroleptic-naive psychotic patients. METHOD: Magnetic resonance imaging volumetric studies were conducted in newly diagnosed neuroleptic-naive schizophrenic and nonschizophrenic psychotic patients and in matched healthy comparison subjects. RESULTS: Both patient groups had bilaterally reduced caudate, but not putamen, volumes, compared to the healthy subjects, after adjustment for intracranial volume. CONCLUSIONS: Decreases in caudate volume in newly diagnosed psychotic patients may be related to the primary pathophysiology of these disorders; prior observations of increased caudate volume may reflect effects of neuroleptic treatment.
Pharmacological, neurobehavioral, and clinical research point to the possible implication of basal ganglia in schizophrenia. The basal ganglia represent target fields for dopaminergic tracts presumed to be important in the pathogenesis of schizophrenia. Basal ganglia play a critical role in higher cognitive functions such as attention, working memory, and goal-directed behavior (1, 2). Lesions of basal ganglia may result in disturbances in thinking and behavior reminiscent of schizophrenia (3). Involuntary movements were described in schizophrenia long before the era of neuroleptics (4); unusual movements are also seen in preschizophrenic children long before illness onset (5). Despite this compelling theoretical evidence, however, neuropathological studies of the basal ganglia have thus far revealed largely equivocal results (3).
Magnetic resonance imaging (MRI) allows noninvasive in vivo examination of the structural abnormalities of the basal ganglia. Several MRI studies have appeared in the literature (6–23), and the results are conflicting (also see review by Shenton et al. [24]). Jernigan et al. (6) first reported an increase in lenticular nuclei volume in schizophrenia. Since then, seven other studies have reported increased volume of one or other basal ganglia structures (7–11, 13, 14). Five studies have shown no differences in basal ganglia size (12, 15, 16, 20, 23). Four studies have shown a reduction in caudate size in subpopulations of schizophrenic subjects characterized by tardive dyskinesia (17, 18), negative symptoms (19), or drug-induced parkinsonism (21). These inconsistencies may be related to methodological issues, e.g., use of thick slices with interslice gaps, making it difficult to avoid partial volume effects (8, 15, 20), or use of only area measures in some studies (20, 21). Further, most of these studies involved previously treated schizophrenic patients, which suggests that the observed changes may be related to neuroleptic treatment.
Two studies have examined basal ganglia volume in early psychoses. DeLisi et al. (8) observed a trend for reduced caudate volume in first-episode schizophrenic patients by comparison with chronic schizophrenic and healthy comparison subjects. Chakos et al. (12) did not find differences between first-episode schizophrenic and healthy comparison subjects. In both of those studies, most patients had received neuroleptic medications before the baseline MRI scan. Few studies have examined basal ganglia volumes in neuroleptic-naive schizophrenic patients. Such studies can help clarify whether basal ganglia abnormalities are secondary to neurolep~tic treatment or whether they are primary to the illness.
In this study, we conducted MRI morphometric studies of the basal ganglia in newly diagnosed neuroleptic-naive schizophrenic and matched healthy comparison subjects. We also examined a group of neuroleptic-naive non~schizophrenic psychotic patients in order to address the issues of diagnostic specificity. Follow-up neuroimaging data have been previously published from a subset of these data (22). In this report, we provide new data on basal ganglia volume measures at baseline. We have focused on the caudate and putamen nuclei, since they are the most easily and reliably measured among basal ganglia nuclei. We were unable to obtain satisfactory interrater reliability with the globus pallidus and therefore did not measure this structure.
METHOD
Sixteen first-episode neuroleptic-naive schizophrenic patients (schizophrenia, N=13; and schizoaffective disorder, N=3), nine nonschizophrenic psychotic patients (bipolar disorder with psychotic features, N=3; major depression with psychotic features, N=3; and psychotic disorders not otherwise specified, N=3), and 17 normal comparison subjects were studied. All subjects provided fully informed written consent. The patients were diagnosed by DSM-III-R criteria at consensus meetings incorporating all clinical, follow-up, and Structured Clinical Interview for DSM-III-R (SCID) (25) data. Normal comparison subjects were recruited from neighborhoods in which the patients resided, were assessed with the SCID (nonpatient version), and were matched, as a group, with the schizophrenic patients for age, sex, race, and parental socioeconomic status (26). Exclusion criteria included significant medical illness, substance abuse or dependence, prior neuroleptic treatment, and IQ lower than 70. Illness durations were computed from the onset of prodromal symptoms to entry into the study. In order to obtain the onset dating as accurately as possible, we timed the dates of onset of the first identifiable psychotic and prodromal symptoms on the basis of a best-estimate approach using data gathered from multiple sources, including the medical record, direct patient interview, and, when possible, a family interview. Dating of the onset of the first prodromal or psychotic symptom was estimated to the closest month (estimated range of error=±1 month), when possible. The duration for the schizophrenic group (N=15) was 301.35 weeks (SD=269.14, range=8–823). For one patient, it was difficult to determine the age at onset. The illness duration in the nonschizophrenic psychotic group was 155.06 weeks (SD=159.04, range=6–463).
MRI scans were conducted with a 1.5-Tesla General Electric Signa system (General Electric Medical Systems, Milwaukee) at the University of Pittsburgh Medical Center. A spin echo sagittal scout scan and axial scans (slice thickness=2.8 mm; no interslice gap; three-dimensional spoiled gradient recalled acquisition pulse sequence; TR=40 msec; TE=20 msec) were acquired. They were identified by scan number alone to retain blindness and were analyzed on a MacIntosh workstation with IMAGE software (version 1.55) (27) by trained raters, through use of a semiautomated segmentation algorithm (28). The right and left caudate nuclei were measured by using a manual tracing technique (22, 29). Intracranial volume was calculated by summing up areas of successive axial slices including gray matter, white matter, and CSF and multiplying by slice thickness. Mean number of slices was as follows: right caudate, 11.5; left caudate, 11.5; right putamen, 7.1; and left putamen, 7.2. Intrarater reliabilities (N=10) ranged from 0.90 to 0.97 for caudate and from 0.92 to 0.94 for putamen. Interrater reliabilities in our laboratory (W. Bagwell, E. Dick, M. Zeigler, and T. Kisler) (N=10; intraclass r) were high for caudate (r=0.94), putamen (r=0.97), and intracranial volume (r=0.99) but were poor for globus pallidus (r=0.26).
Separate measurements were obtained for the left and right caudate nuclei through use of a manual tracing technique. The head and body of the caudate were measured, whereas the tail was excluded. The caudate nucleus is delineated medially and superiorly by the lateral ventricle and elsewhere by frontal white matter; it is separated from the putamen by the white matter tracts of the anterior limb of the internal capsule. We included the nucleus accumbens, which merges inferiorly with the caudate; it is hard to reliably demarcate this structure from the caudate nucleus. All regions were measured in the axial plane.
Separate measurements were obtained for the left and right putamen by using manual tracing. The putamen is delineated medially by the globus pallidus and laterally and inferiorly by white matter tracts of the external capsule. The caudate and the putamen are connected inferiorly by gray matter bridges; because of the partial volume effects, these are excluded from the measurements. Measurements of the putamen were performed in the axial plane (figures 1 and 2).
We conducted analysis of covariance (ANCOVA), with intracranial volume as a covariate, and Newman-Keuls post hoc tests to examine significant differences between diagnostic groups; we used Pearson's correlations and partial correlations to examine the relation among age, illness duration, and caudate and putamen volume. For dichotomous variables such as sex and handedness, we used the Kruskal-Wallis analysis of variance (ANOVA). All significance values reported are two-tailed.
RESULTS
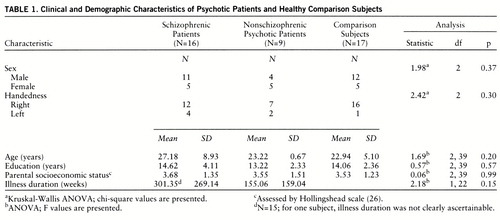
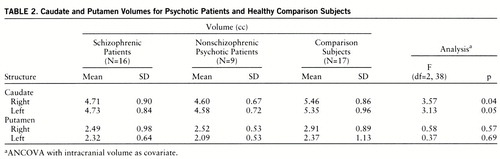
There were no significant differences among the three groups in age, sex, education, handedness, or parental socioeconomic status (table 1). Age did not correlate with caudate and putamen volumes in any of the diagnostic groups. Intracranial volume was not significantly different among the groups (schizophrenic patients: mean=1476.99 cc, SD=185.33; nonschizophrenic psychotic patients: mean=1528.93 cc, SD=17.68; comparison subjects: mean=1576.57 cc, SD=172.97) (F=1.41, df=2,39, p=0.26). ANCOVA, with intracranial volume as a covariate, revealed significant intergroup differences in both left and right and in total caudate volume (table 2). Post hoc tests revealed that both patient groups had smaller right and left caudate volumes than the comparison subjects. Illness duration (after intracranial volume was partialled out) was unrelated to caudate or putamen in both the schizophrenic and the nonschizophrenic psychotic groups (all partial r values <0.5). No significant differences were seen between the subject groups for right or left putamen.
DISCUSSION
Significant reductions (about 14%) were seen in caudate volumes in neuroleptic-naive schizophrenic patients. These findings may be diagnostically nonspecific, since similar volume reductions were also seen in nonschizophrenic psychotic patients; reduced caudate volume has also been described in depression (30). In a prospective study of a subset of these first-episode psychotic patients, we (22) and others (10) have found that caudate volumes increase following treatment with neuroleptics. Previous observations of increased caudate volume in schizophrenia may therefore reflect neuroleptic effects. Thus, caudate volume reduction in the neuroleptic-naive patients may reflect primary pathophysiology of schizophrenia and may account for some of the cognitive and psychomotor abnormalities in this illness.
Our observations of caudate, but not putamen, volume reductions in neuroleptic-naive psychotic patients deserve comment. The putamen mainly receives projections from cortical regions involved in motor control (31, 32). On the other hand, recent studies in primates have shown that the caudate nuclei are clearly activated during working memory-related tasks (2). Thus, this structure may be part of a distributed neuronal network subserving functions associated with the dorsolateral prefrontal cortex, implicated in the pathogenesis of schizophrenia. Our observations are also consistent with functional neuroimaging research. Significantly reduced basal ganglia metabolism has been observed in unmedicated schizophrenic patients through use of positron emission tomography (33–35) and single photon emission tomography (36). On the other hand, treated schizophrenic patients had higher blood flow in basal ganglia (37, 38). Indeed, one study showed decreased caudate metabolism at baseline that reversed following institution of neuroleptic treatment (34).
The lack of association between caudate volume and illness duration should be viewed with caution, since studies of patients with longer duration of illness may reveal the effects of chronicity. Nevertheless, this finding and the observation of caudate volume reduction early in the illness provide some indirect support for neurodevelopmentally mediated pathology in schizophrenia (39) and possibly in affective disorder (40). An exaggeration of periadolescent synaptic pruning, perhaps in glutamatergic corticosubcortical neurons, may be involved (41). Reduced activity in these cortico~striatal neurons, by diminishing trophic effects on the striatum, could conceivably lead to reduced synaptic neuropil, and thereby reduced size; this view is consistent with a recent observation of reduced striatal dendritic spine size in postmortem brains of schizophrenic patients (42).
Many brain regions have been implicated in the neuroanatomy of schizophrenia. Our findings suggest that the relevant brain circuits underlying the pathophysiology of schizophrenia are likely to include the caudate nuclei; however, several other regions and abnormal patterns of interregional cross-talk may be involved in this disorder. Our findings must be considered preliminary in view of the relatively small study group size. Further studies of basal ganglia structure and metabolism, through use of state-of-the-art neuroimaging techniques, are clearly warranted.
 |
 |
Received May 20, 1997; revision received Nov. 10, 1997; accepted Nov. 25, 1997. From Western Psychiatric Institute and Clinic. Address reprint requests to Dr. Keshavan, Western Psychiatric Institute and Clinic, 3811 O'Hara St., Pittsburgh, PA 15213-2593; [email protected] (e-mail). Supported in part by NIMH grants MH-01372, MH-42969, and MH-45156 and by a Scottish Rite Foundation grant. Wright Bagwell, B.A., Tanya Kisler, B.S., Melissa Zeigler, B.S., and Elizabeth Dick, B.S., conducted morphometric measurements; Drs. Gretchen Haas and Nina Schooler helped in the study's clinical aspects.

FIGURE 1. An Axial MRI Slice Showing the Demarcation of the Caudate Nucleus in a Healthy Comparison Subject

FIGURE 2. An Axial MRI Slice Showing the Demarcation of the Putamen in a Healthy Comparison Subject
1 Middleton FA, Strick PL: Anatomical evidence for cerebellar and basal ganglia involvement in higher cognitive function. Science 1994; 266:458–461Crossref, Medline, Google Scholar
2 Levy R, Friedman HR, Davachi L, Goldman-Rakic PS: Differential activation of the caudate nucleus in primates performing spatial and nonspatial working memory tasks. J Neurosci 1997; 17:3870–3882Crossref, Medline, Google Scholar
3 Heckers S: Neuropathology of schizophrenia: cortex, thalamus, basal ganglia, and neurotransmitter-specific projection systems. Schizophr Bull 1997; 23:403–421Crossref, Medline, Google Scholar
4 Kraepelin E: Dementia Praecox and Paraphrenia. Edinburgh, E & S Livingstone, 1919Google Scholar
5 Walker E, Lewine RJ: Predictions of adult-onset schizophrenia from childhood home movies of the patients. Am J Psychiatry 1990; 147:1052–1056Link, Google Scholar
6 Jernigan TL, Zisook S, Heaton RK, Moranville JT: Magnetic resonance imaging abnormalities in lenticular nuclei and cerebral cortex in schizophrenia. Arch Gen Psychiatry 1991; 48:881–890Crossref, Medline, Google Scholar
7 Breier A, Buchanan RW, Elkashef A, Munson RC, Kirkpatrick B, Gellad F: Brain morphology and schizophrenia: a magnetic resonance imaging study of limbic, prefrontal cortex, and caudate structures. Arch Gen Psychiatry 1992; 49:921–926Crossref, Medline, Google Scholar
8 DeLisi LE, Hoff AL, Schwartz JE, Shields GW, Halthore SN, Gupta SM, Henn FA, Anand AK: Brain morphology in first-episode schizophrenic-like psychotic patients: a quantitative magnetic resonance imaging study. Biol Psychiatry 1991; 29:159–175Crossref, Medline, Google Scholar
9 Gordon CT, Frazier JA, McKenna K, Giedd J, Zametkin A, Zahn T, Hommer D, Hong W, Kaysen D, Albus KE: Childhood-onset schizophrenia: an NIMH study in progress. Schizophr Bull 1994; 20:697–712Crossref, Medline, Google Scholar
10 Swayze VW II, Andreasen NC, Alliger RJ, Yuh WT, Ehrhardt JC: Subcortical and temporal structures in affective disorder and schizophrenia: a magnetic resonance imaging study. Biol Psychiatry 1992; 31:221–240Crossref, Medline, Google Scholar
11 Hokama H, Shenton ME, Nestor PG, Kikinis R, Levitt JJ, Metcalf D, Wible CG, O'Donnell BF, Jolesz FA, McCarley RW: Caudate, putamen, and globus pallidus volume in schizophrenia: a quantitative MRI study. Psychiatry Res 1995; 61:209–229Crossref, Medline, Google Scholar
12 Chakos MH, Lieberman JA, Bilder RM, Borenstein M, Lerner G, Bogerts B, Wu H, Kinon B, Ashtari M: Increase in caudate nuclei volumes of first-episode schizophrenic patients taking antipsychotic drugs. Am J Psychiatry 1994; 151:1430–1436Link, Google Scholar
13 Frazier JA, Giedd JN, Hamburger SD, Albus KE, Kaysen D, Vaituzis AC, Rajapakse JC, Lenane MC, McKenna K, Jacobsen LK, Gordon CT, Breier A, Rapoport JL: Brain anatomic magnetic resonance imaging in childhood-onset schizophrenia. Arch Gen Psychiatry 1996; 53:614–624Crossref, Google Scholar
14 Buchanan RW, Breier A, Kirkpatrick B, Elkashef A, Munson RC, Gellad F, Carpenter WT Jr: Structural abnormalities in deficit and nondeficit schizophrenia. Am J Psychiatry 1993; 150:59–65Link, Google Scholar
15 Kelsoe JR Jr, Cadet JL, Pickar D, Weinberger DR: Quantitative neuroanatomy in schizophrenia: a controlled magnetic resonance imaging study. Arch Gen Psychiatry 1988; 45:533–541Crossref, Medline, Google Scholar
16 Corey-Bloom J, Jernigan T, Archibald S, Harris MJ, Jeste DV: Quantitative magnetic resonance imaging of the brain in late-life schizophrenia. Am J Psychiatry 1995; 152:447–449Link, Google Scholar
17 Mion CC, Andreasen NC, Arndt S, Swayze VW II, Cohen GA: MRI abnormalities in tardive dyskinesia. Psychiatry Res 1991; 40:157–166Crossref, Medline, Google Scholar
18 Dalgalarrondo P, Gattaz WF: Basal ganglia abnormalities in tardive dyskinesia: possible relationship with duration of neuroleptic treatment. Eur Arch Psychiatry Clin Neurosci 1994; 244:272–277Crossref, Medline, Google Scholar
19 Young AH, Blackwood DH, Roxborough H, McQueen JK, Martin MJ, Kean D: A magnetic resonance imaging study of schizophrenia: brain structure and clinical symptoms. Br J Psychiatry 1991; 158:158–164Crossref, Medline, Google Scholar
20 Blackwood DH, Young AH, McQueen JK, Martin MJ, Roxborough HM, Muir WJ, St Clair DM, Kean DM: Magnetic resonance imaging in schizophrenia: altered brain morphology associated with P300 abnormalities and eye tracking dysfunction. Biol Psychiatry 1991; 30:753–769Crossref, Medline, Google Scholar
21 Brown KW, Wardlaw JM, White T, Walker N: Caudate nucleus area in drug-induced parkinsonism. Acta Psychiatr Scand 1996; 94:348–351Crossref, Medline, Google Scholar
22 Keshavan MS, Bagwell WW, Haas GL, Sweeney JA, Schooler NR, Pettegrew JW: Changes in caudate volume with neuroleptic treatment (letter). Lancet 1994; 344:1434Crossref, Medline, Google Scholar
23 Flaum M, Swayze VW II, O'Leary DS, Yuh WTC, Ehrhardt JC, Arndt SV, Andreasen NC: Effects of diagnosis, laterality, and gender on brain morphology in schizophrenia. Am J Psychiatry 1995; 152:704–714Link, Google Scholar
24 Shenton ME, Wible CG, McCarley RW: A review of magnetic resonance imaging studies of brain abnormalities in schizophrenia, in Brain Imaging in Clinical Psychiatry. Edited by Krishnan KRR, Doraiswamy PM. New York, Marcel Dekker, 1997, pp 297–380Google Scholar
25 Spitzer RL, Williams JBW: Structured Clinical Interview for DSM-III-R (SCID). New York, New York State Psychiatric Institute, Biometrics Research, 1985Google Scholar
26 Hollingshead AB: Four-Factor Index of Social Status. New Haven, Conn, Yale University, Department of Sociology, 1975Google Scholar
27 Rasband W: NIH Image Manual. Bethesda, Md, National Institutes of Health, 1993Google Scholar
28 Keshavan MS, Anderson S, Beckwith C, Nash K, Pettegrew J, Krishnan KRR: A comparison of stereology and segmentation techniques for volumetric measurements of brain ventricles. Psychiatry Res Neuroimaging 1995; 61:53–60Crossref, Medline, Google Scholar
29 Rosenberg D, Keshavan MS, O'Hearn KM, Dick EL, Bagwell W, Seymour A, Montrose DM, Pierri JN, Birmaher B: Frontostriatal measurement in treatment-naive children with obsessive-compulsive disorder. Arch Gen Psychiatry 1997; 54:824–830Crossref, Medline, Google Scholar
30 Krishnan KRR, McDonald WM, Escalona PR, Doraiswamy PM, Na C, Husain MM, Figiel GS, Boyko OB, Ellinwood EH, Nemeroff CB: Magnetic resonance imaging of the caudate nuclei in depression: preliminary observations. Arch Gen Psychiatry 1992; 49:553–557Crossref, Medline, Google Scholar
31 Goldman PS, Nauta WJH: Prefronto-caudate projection in the rhesus monkey. J Comp Neurol 1977; 171:369–385Crossref, Google Scholar
32 Cote L, Crutcher MD: The basal ganglia, in Principles of Neural Science. Edited by Kandel ER, Schwartz JH, Jessell TM. New York, Elsevier, 1991, pp 647–659Google Scholar
33 Weisel FA, Wilk G, Sjorgren I, Blomquist G, Greitz T: Altered relationships between metabolic rates of glucose in brain regions of schizophrenic patients. Acta Psychiatr Scand 1987; 76:642–647Crossref, Medline, Google Scholar
34 Buchsbaum MS, Potkin SG, Siegel BV Jr, Lohr J, Katz M, Gott~schalk LA, Gulasekaram B, Marshall JF, Lottenberg S, Teng CY: Striatal metabolic rate and clinical response to neuroleptics in schizophrenia. Arch Gen Psychiatry 1992; 49:966–974Crossref, Medline, Google Scholar
35 Siegel BV Jr, Buchsbaum MS, Bunney WE Jr, Gottschalk LA, Haier RJ, Lohr JB, Lottenberg S, Najafi A, Nuechterlein KH, Potkin SG, Wu JC: Cortical-striatal-thalamic circuits and brain glucose metabolic activity in 70 unmedicated male schizophrenic patients. Am J Psychiatry 1993; 150:1325–1336Link, Google Scholar
36 Vita A, Bressi S, Perani D, Invernizzi G, Giobbio GM, Dieci M, Garbarini M, Del Sole A, Fazio F: High-resolution SPECT study of regional cerebral blood flow in drug-free and drug-naive schizophrenic patients. Am J Psychiatry 1995; 152:876–882Link, Google Scholar
37 Szechtman HNC, Nahmias C, Garnett S, Firnau G, Brown GM, Kaplin RD: Effect of neuroleptics on altered cerebral glucose metabolism in schizophrenia. Arch Gen Psychiatry 1988; 45:523–532Crossref, Medline, Google Scholar
38 Wik G, Wiesel FA, Sjogren I, Blomquist G, Greitz T, Stone-Elander S: Effects of sulpiride and chlorpromazine on regional cerebral metabolism in schizophrenic patients as determined by positron emission tomography. Psychopharmacology (Berl) 1989; 97:309–318Crossref, Medline, Google Scholar
39 Weinberger DR: Implications of normal brain development for the pathogenesis of schizophrenia. Arch Gen Psychiatry 1987; 44:660–669Crossref, Medline, Google Scholar
40 Nasrallah HA: Neurodevelopmental models of affective disorders, in Neurodevelopment and Adult Psychopathology. Edited by Keshavan MS, Murray RM. London, Cambridge University Press, 1997, pp 199–206Google Scholar
41 Keshavan MS, Anderson S, Pettegrew JW: Is schizophrenia due to excessive synaptic pruning in the prefrontal cortex? the Feinberg hypothesis revisited. J Psychiatr Res 1994; 28:239–265Crossref, Medline, Google Scholar
42 Roberts RC, Conley R, Kung L, Peretti FJ, Chute DJ: Reduced striatal spine size in schizophrenia: a postmortem ultrastructural study. Neuroreport 1996; 7:1214–1218Crossref, Medline, Google Scholar

