
Rapid Cycling in Women and Men With Bipolar Manic-Depressive Disorders
Abstract
Objective:This study investigated risks for rapid cycling, as defined by DSM-IV, in women and men with bipolar disorders. Method:The results of 10 studies with a total of 2,057 bipolar patients were meta-analyzed by pooled contingency methods. Results:The proportions of women and men among rapid-cycling cases averaged 72% and 28%, respectively, but the risk of rapid cycling was inconsistently more frequent among women (29.6%) than among men (16.5%). The mean number of episodes per year was much higher in rapid-cycling patients before and during lithium treatment but was similar in rapid-cycling men and women.Conclusions:Rapid cycling was only moderately, and inconsistently, more common in bipolar women than men. Am J Psychiatry 1998; 155: 1434-1436
A rapid-cycling course (1, 2), with at least four major affective episodes in a year, is included in DSM-IV as a diagnostic specifier for the criteria for bipolar manic-depressive disorders. Rapid cycling appears to be a diagnostically reliable phenomenon (3-5), is particularly common among patients with type II bipolar disorders, is associated with high rates of morbidity with potentially severe disability, and may predict an unsatisfactory response to lithium maintenance treatment (6-10). The reported incidence of rapid-cycling patients among persons with bipolar disorders is about 15%, although this rate may be somewhat inflated because of sampling from specialized mood disorders clinics where such difficult patients may be overrepresented (1-10).
It is widely accepted that women with a bipolar disorder are at particularly high risk of rapid cycling (6, 7). Women have accounted for 72.6% (range=58%–92%) of rapid-cycling bipolar patients (9, 10). However, these rates do not necessarily represent the sex-specific risk of a rapid-cycling course, since clinical samples may contain dissimilar proportions of women and men at risk. In an attempt to clarify this remaining uncertainty, we evaluated the relative risk of rapid cycling in women and men with a bipolar disorder.
METHOD
Reports containing data on the sex distribution of patients with rapid-cycling (four or more episodes in a year) and non-rapid-cycling bipolar disorder were located by means of a computerized literature search (MEDLINE) supplemented by previous reports (1-10) and their citations. The studies that were included in this analysis provided data to permit specific comparisons of rates of rapid cycling in bipolar women and men. To the nine reports that were found we added new data on 355 patients with bipolar disorder from the Lucio Bini mood disorders research center in Cagliari, Sardinia, evaluated as described previously (11). Sex distribution was analyzed by comparing rates of rapid-cycling cases in women and men within, across, and between studies by Mantel-Haenszel (chi-square) methods for pooling contingency tables in meta-analyses (12, 13).
RESULTS
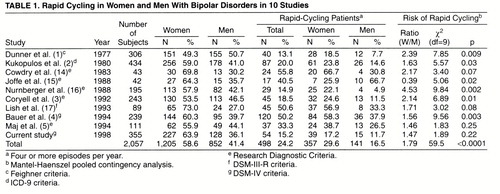
A total of 10 studies (1-5, 14-17) with 2,057 bipolar disorder patients provided suitable data (table 1). There were more female subjects than male subjects, with no evidence of sex bias in case selection. A rapid-cycling course was found in 24.2% of the patients, but this rate was probably inflated by selection of rapid-cycling cases in some studies (4, 14, 15, 17) that had unusually high proportions of such cases (40.5%–55.8%). Women and men, respectively, represented 71.7% (357/498) and 28.3% (141/498) of rapid-cycling cases (a 2.53-fold difference), but rapid cycling occurred in only 29.6% of women and 16.6% of men. This 1.78-fold difference was statistically highly significant when all available data were pooled. However, significant sex differences in the risk of a rapid-cycling course were found in only six of the 10 studies (table 1), and there was highly significant inconsistency of results across studies (for lack of homogeneity, χ2=40.2, df=9, p<0.0001).
Among our own unselected bipolar subjects, 15.2% had rapid cycling. The cycling rate (episodes per year) before maintenance treatment was 2.52 times higher among the 54 rapid-cycling patients (mean=3.85, SD=3.78) than among the 301 non-rapid-cycling patients (mean=1.53, SD=1.61) (t=7.42, df=353, p<0.0001). The rapid-cycling patients also had a 2.17 times higher average cycling rate during lithium maintenance treatment (mean=1.38, SD=1.99, versus mean=0.63, SD=0.70; t=4.54, df=353, p<0.001). However, there was little difference in cycling rates between the 15 rapid-cycling men and the 39 rapid-cycling women before lithium maintenance treatment (mean=4.94, SD=4.58, and mean=3.41, SD=3.38, respectively; t=1.33, df=52, n.s.) or during lithium maintenance treatment (mean=1.21, SD=2.37, and mean=1.45, SD=1.85, respectively; t=0.39, df=52, n.s.).
DISCUSSION
This analysis included all of the studies we found that had data permitting computation of rates of rapid cycling in bipolar women and bipolar men. It was limited by variance in patient selection and diagnoses and possible underreporting of rapid-cycling men, given a widespread impression that rapid cycling is much more common in women (1-10). More women than men (2.53-fold) were found among the rapid-cycling bipolar patients. However, the sex difference favoring women was inconsistent (six of 10 studies) and more moderate (1.79-fold) than suggested by analyses based on the frequency of women and men among rapid-cycling bipolar patients (1-10). Moreover, cycling rates (average number of episodes per year) were similar in rapid-cycling men and women both before and during lithium maintenance treatment.
Evidently, estimates of risk based on the proportion of women among rapid-cycling patients can be misleading, perhaps because of sampling factors, including possible overrepresentation of women among patients treated for major mood disorders. Although the reported sex ratio of risk for bipolar disorders is close to 1.0 (7, 18), women may more often seek and accept treatment for major mood disorders, including lithium for bipolar disorders (7) and antidepressants for nonbipolar major depression (19). In turn, some of the risk for rapid cycling in women may reflect excessive use of antidepressants without adequate mood-stabilizing treatment (2, 4, 7, 20). In conclusion, the present findings indicate that rapid cycling in bipolar disorders occurs in both men and women, with somewhat greater risk in women, but at similar cycling rates before and during lithium maintenance treatment in both sexes.
Received Dec. 1, 1997; revision received Feb. 23, 1998; accepted April 17, 1998. From the International Consortium for Bipolar Disorder Research, Department of Psychiatry and Neuroscience Program, Harvard Medical School, and Mailman Research Center, McLean Division of Massachusetts General Hospital, Boston; and the Centro Lucio Bini, a Stanley Foundation European Psychiatric Research Center, Sardinia, Italy.. Address reprint requests to Dr. Baldessarini, Mailman Research Center, McLean Hospital, 115 Mill St., Belmont, MA 02178. Supported by NIMH grant MH-47370 and awards from the National Alliance for Research on Schizophrenia and Depression, the Theodore and Vada Stanley Foundation of the National Alliance for the Mentally Ill, the Consiglio Nazionale delle Ricerche, the Bruce J. Anderson Foundation, and the McLean Private Donors Neuropharmacology Research Fund.The authors thank Adele C. Viguera, M.D., for her comments.
 |
1. Dunner DL, Vijayalakshmy P, Fieve RR: Rapid cycling manic depressive patients. Compr Psychiatry 1977; 18:561–566Crossref, Medline, Google Scholar
2. Kukopulos A, Reginaldi D, Laddomada P, Floris G, Serra G, Tondo L: Course of the manic-depressive cycle and changes caused by treatments. Pharmakopsychiatrie Neuropsychopharmakologie 1980; 13:156–167Medline, Google Scholar
3. Coryell W, Endicott J, Keller M: Rapidly cycling affective disorder. Arch Gen Psychiatry 1992; 49:126–131Crossref, Medline, Google Scholar
4. Bauer MS, Calabrese J, Dunner DL, Post R, Whybrow PC, Gyulai L, Tay LK, Younkin SR, Bynum D, Lavori P, Price RA: Multisite data reanalysis of the validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry 1994; 151:506–515Link, Google Scholar
5. Maj M, Magliano L, Pirozzi R, Marasco C, Guarneri M: Validity of rapid cycling as a course specifier for bipolar disorder. Am J Psychiatry 1994; 151:1015–1019Link, Google Scholar
6. Alarcon RD: Rapid cycling affective disorders: a clinical review. Compr Psychiatry 1985; 26:522–540Crossref, Medline, Google Scholar
7. Goodwin FK, Jamison KR: Manic-Depressive Illness. New York, Oxford University Press, 1990, pp 157–185, 665–724, 746–762Google Scholar
8. Faedda GL, Baldessarini RJ, Tohen M, Strakowski SM, Waternaux C: Episode sequence in bipolar disorder and response to lithium treatment. Am J Psychiatry 1991; 148:1237–1239Link, Google Scholar
9. Leibenluft E: Women with bipolar illness: clinical and research issues. Am J Psychiatry 1996; 153:163–173Link, Google Scholar
10. Leibenluft E: Issues in the treatment of women with bipolar illness. J Clin Psychiatry 1997; 58(suppl 15):5–11Google Scholar
11. Tondo L, Baldessarini RJ, Hennen J, Floris G: Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry 1998; 155:638–645Link, Google Scholar
12. Hedges LV, Olkin I: Statistical Methods for Meta-Analysis. Orlando, Fla, Academic Press, 1985Google Scholar
13. Janicak PG, Davis JM, Gibbons RD, Ericksen S, Chang S, Gallagher P: Efficacy of ECT: a meta-analysis. Am J Psychiatry 1985; 142:297–302Link, Google Scholar
14. Cowdry RW, Wehr TA, Zis AP, Goodwin FK: Thyroid abnormalities associated with rapid-cycling bipolar illness. Arch Gen Psychiatry 1983; 40:414–420Crossref, Medline, Google Scholar
15. Joffe RT, Kutcher S, MacDonald C: Thyroid function and bipolar affective disorder. Psychiatry Res 1988; 25:117–121Crossref, Medline, Google Scholar
16. Nurnberger J, Guroff JJ, Hamovit J, Berrettini W, Gershon E: A family study of rapid-cycling bipolar illness. J Affect Disord 1988; 15:87–91Crossref, Medline, Google Scholar
17. Lish JD, Gyulai L, Resnick SM, Kirtland A, Amsterdam JD, Whybrow PC, Price RA: A family history study of rapid-cycling bipolar disorder. Psychiatry Res 1993; 48:37–45Crossref, Medline, Google Scholar
18. Weissman MM, Leaf PJ, Tischler GL, Blazer DG, Karno M, Bruce ML, Florio LP: Affective disorders in five United States communities. Psychol Med 1988; 18:141–153Crossref, Medline, Google Scholar
19. Hohmann AA: Gender bias in psychotropic drug prescribing in primary care. Med Care 1989; 27:478–490Crossref, Medline, Google Scholar
20. Wehr TA, Sack DA, Rosenthal NE, Cowdry KW: Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry 1988; 145:179–184Link, Google Scholar

