Clinical Genetics, VII: From Genetics to Pathophysiology: Positional Cloning
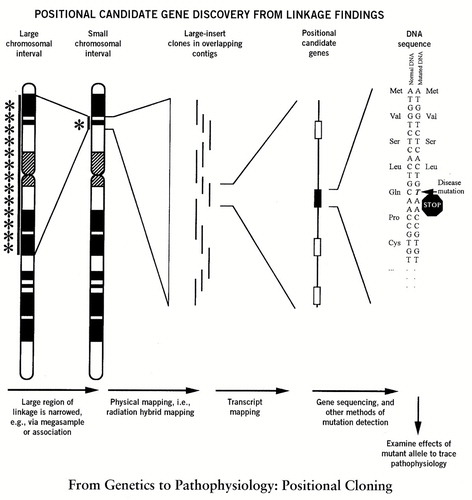
Positional cloning solves problems that are largely intractable under older paradigms, in this case, the problem of identification of causative biological abnormalities in disease. It moves from identification of an abnormal human gene to its associated biological aberration. The process of positional cloning is sketched above. A representative human chromosome ideogram is displayed, with the indicated genetic intervals becoming progressively smaller as the process of positional cloning advances across the figure from the left side to the right, where a disease mutation is discovered. First, genetic mapping (linkage analysis) is carried out in families with affected individuals. This allows identification of the chromosomal region of a susceptibility gene. Once this has been completed, the region containing the gene must be narrowed, candidate genes in the region must be identified, and the functional mutation in the abnormal gene must be determined. Narrowing of the region can be accomplished by massive sampling of families, by detection of association (linkage disequilibrium) of the disease to a gene within the region, or by a fortunate choice (based on known function) of a gene within the region. When considering how many markers to examine in a particular region for association, one must take population history into account. In an isolated population only a few generations from a hypothesized disease mutation, a sparse coverage of markers should be adequate to detect an association, but it will be difficult to narrow the area a great deal because of relatively large unrecombined segments of a chromosome. However, in a larger and outbred population, the association (linkage disequilibrium), if detectable, would span a much smaller interval. Hence, detection would require more densely spaced markers than in the former case, yet would also provide much more assistance in narrowing the region of interest.
Positional cloning culminates in the discovery of a disease mutation in an affected individual (in the figure above), a premature stop codon. Following completion of these efforts, the biological action of the disease gene can then be determined, and thus one cause of illness predisposition is revealed. The benefits of this finding may be precise diagnostic tests for susceptibility to specific types of diseases, treatment based on case-specific diagnostic test information, drugs focused on biological cause, and, ultimately, gene therapy for some types of illness.
Address reprint requests to Dr. Tamminga, Maryland Psychiatric Research Center, P.O. Box 21247, Baltimore, MD 21228. Figure adapted from G.D. Schuler, M.S. Boguski, E.A. Stewart, et al.: A Gene Map of the Human Genome. Science 1996; 274:540–546, and F.S. Collins: Positional Cloning Moves From Perditional to Traditional. Nature Genetics 1995; 9:347–350.