
Trajectories of PTSD: A 20-Year Longitudinal Study
Abstract
Objective: This study assessed the psychopathological effects of combat in veterans with and without combat stress reaction. Method: Veterans (N=214) from the 1982 Lebanon War were assessed in a prospective longitudinal design: 131 suffered from combat stress reaction during the war, and 83 did not. They were evaluated 1, 2, 3, and 20 years after the war. Results: Combat stress reaction is an important vulnerability marker. Veterans with combat stress reaction were 6.6 times more likely to endorse posttraumatic stress disorder (PTSD) at all four measurements, their PTSD was more severe, and they were at increased risk for exacerbation/reactivation. A qualitative analysis of the profile of PTSD symptoms revealed some time-related changes in the symptom configuration of veterans who did not suffer from combat stress reaction. In both groups, the course fluctuated; PTSD rates dropped 3 years postwar and rose again 17 years later; 23% of veterans without combat stress reaction reported delayed PTSD. Conclusions: These findings suggest that the detrimental effects of combat are deep and enduring and follow a complex course, especially in combat stress reaction casualties. The implications of aging and ongoing terror in impeding recovery from the psychological wounds of war are discussed.
The massive pressures of war have long been recognized to produce both immediate (acute) and long-term (chronic and delayed) psychopathology (e.g., references 1 , 2) . On the battlefield, the most common acute reaction is combat stress reaction, also known as battle shock, battle fatigue, and other names. Combat stress reaction consists of various polymorphic and labile psychiatric and somatic symptoms and is diagnosed based on impaired functioning by trained clinicians (2) . Among the symptoms that may characterize this condition are paralyzing fear of death, emotional and physical numbness, withdrawal, severe depression, and impaired combat functioning (1) . Combat stress reaction can be seen as a specific type of acute stress disorder. With the end of a war, the debilitating effects of combat stress may abate in many cases, either spontaneously or with the help of professional intervention, whereas in others, acute stress reaction crystallizes into profound and prolonged psychopathological sequelae in the form of posttraumatic stress disorder (PTSD) and other comorbidities. Yet individuals who have had an acute reaction are at increased risk for chronic and recurrent/reactivated disorder (3) . In some cases, individuals who initially appeared to respond adaptively to combat stress develop psychopathology after an asymptomatic latency (e.g., references 4 , 5) that, according to DSM–IV, lasts at least 6 months. The course of PTSD fluctuates, but recovery can be expected in the majority of cases. In a small proportion of patients, the condition may show a chronic course over many years.
Current knowledge regarding the long-term course and stability of PTSD is based primarily on seminal large-scale retrospective American epidemiological studies (e.g., reference 6 ), comprehensive follow-ups of veterans that commenced years after the Vietnam War (e.g., reference 7 ) and therefore did not assess acute reactions, and several important longitudinal studies of selected groups of civilians (e.g., references 8 , 9) . The introduction of acute stress disorder in DSM–IV has been followed by a growing number of prospective studies (e.g., references 10 , 11) assessing the relationship between acute stress disorder and PTSD. However, this is a relatively new diagnosis, and therefore, the follow-up period in these studies is relatively short. This implies that at least some of our knowledge as reflected, for example, in DSM–IV requires further scientific validation.
The present study uses data from a prospective study of a cohort of Israeli veterans—with and without antecedent combat stress reaction—who participated in the 1982 Lebanon War and were followed up for 20 years. The study assesses posttraumatic symptoms in veterans 1, 2, 3, and 20 years after their combat experience. Our main hypothesis was that combat stress reaction casualties would be at a higher risk for PTSD than veterans without combat stress reaction at all four points of measurement. Beyond this hypothesis, we attempted to address other questions that have major implications for the understanding of etiology, phenomenology, and treatment outcomes and remain to a great extent unanswered: What is the recovery rate from PTSD in veterans with and without combat stress reaction? What is the typical symptom profile in veterans with and without combat stress reaction? Are the profiles different from each other at different points in time? Which symptoms are most prominent shortly after the war and which many years later? What are the trajectories of PTSD in casualties with and without combat stress reaction? What is the relative risk of both veterans with and those without combat stress reaction to suffer from PTSD and to recover completely? What is the respective relative risk for reactivated and delayed PTSD?
Method
Participants
Two groups of veterans participated in this study. The subjects with combat stress reaction were Israeli soldiers who had fought in the Lebanon War and had been identified by military mental health personnel as psychiatric casualties. Criteria for inclusion in this group were: 1) participation in frontline battles during the war, 2) a referral for psychiatric intervention made by the soldier’s battalion surgeon during the war, 3) a diagnosis of combat stress reaction made on the battlefield by clinicians trained and experienced in the diagnosis of combat-related reactions, and 4) no indication in the clinician’s report of serious physical injury and other psychiatric disorders. The research staff determined eligibility by using records of clinicians’ diagnoses made on the battlefield.
The comparison group consisted of soldiers who had participated in combat in the same units as the combat stress reaction group but were not identified as suffering from combat stress reaction.
Although it is difficult to control for the subjective stressfulness of any combat experience, the sampling procedure used here was chosen to ensure that soldiers in both groups were exposed to a similar amount and type of objective stress. All the soldiers in the combat stress reaction and comparison groups underwent stringent physical and psychiatric screening before commencing their military service, and no indication of diagnosable premorbid symptoms was recorded in their medical files. The soldiers’ age in 1983 (the first wave of measurement) ranged from 18 to 37 (mean=25.81, SD=4.72, median=26). Sixteen percent of the participants had completed only eighth grade, 27% had at most some high school, 39% had completed only high school, and 18% had studied beyond high school. The comparison subjects and the veterans with combat stress reaction did not significantly differ in age, education, military rank, and assignment.
The subjects were assessed at four points in time: year 1, year 2, year 3, and year 20 after the Lebanon War. The data in this study are based on the responses of subjects who participated in all four assessments to enable the assessment of the longitudinal trajectory of PTSD. The complete four-wave measurement data set included 131 combat stress reaction casualties and 83 comparison subjects representing 71% of those who responded at times 1–3 and 30% of those who started the study at time 1. Details concerning how many veterans completed the scales at each of the first three waves of measurement are presented by Solomon (3) .
The attrition rate may raise doubts about the unbiased nature of the group. However, high attrition is a common and well-recognized problem in prospective studies. Furthermore, data retrieved from official military records and from the questionnaires filled out at year 1 revealed that the men who participated at all four points in time did not significantly differ from those who declined to participate at times 2, 3, or 4 in sociodemographic and military background, premilitary adjustment, intelligence, or mental and somatic health 1 year after the war.
Measures
The PTSD Inventory is a self-report instrument based on DSM–III, which was the standard used when the study commenced. It was employed at all four points to enable comparison over time. It consists of DSM–III PTSD symptoms as adapted for war trauma. The respondent was asked to indicate whether or not he had experienced each of the described symptoms within the past month. These symptoms were divided into three categories corresponding to the following three DSM–III criteria for the diagnosis of PTSD: 1) reexperiencing of the trauma; 2) numbing of responsiveness to or reduced involvement with the external world; and 3) additional symptoms, including hyperalertness, sleep disturbance, and memory difficulties (12) . The inventory has proven psychometric properties in terms both of high test-retest reliability and concurrent validity compared with clinical diagnosis (e.g., reference 13 ). All the items of the scale showed adequate kurtosis and skewness, implying no violation of normal distribution. Details concerning the reliability of the PTSD inventory over time are presented by Solomon (3) .
DSM–III criteria for PTSD did not include any requirement of disability or distress, which was later added to DSM–IV as criterion F. Throughout the 20 years of this study, we assessed both disability and distress. In the current study, self-reported distress was defined as the global severity index of the commonly used SCL-90. A score of at least 1.26 (13) represented a level of clinical distress commonly observed in treatment seekers. Self-reported dysfunction at work or in social relations was measured by the Social Functioning Problem Scale (14) . Assessment of PTSD was therefore performed in two ways. The first was composed of DSM–III symptom criteria and the second of both symptom criteria and a measure of distress and disability (criterion F).
Procedure
One, 2, and 3 years after their participation in the 1982 Lebanon War, the participants were asked to report to the Headquarters of the Surgeon General to take part in this study. The participants filled out a battery of questionnaires in small groups. Twenty years after the war, data were collected at the veterans’ homes. The participants’ informed consent was obtained, and they were informed that the data would remain confidential and in no way influence their status in military or civilian life.
Results
PTSD Rates
As just noted, the PTSD measure was constructed here in two ways: the first, corresponding to DSM–III symptom criteria, and the second, including the F criterion, as proposed in DSM–IV. Table 1 presents PTSD rates, odds ratios, and confidence intervals according to both sets of criteria in the combat stress reaction and comparison groups at all four time points.
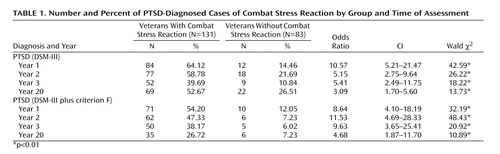
The results show that in the first year, the combat stress reaction group had a 10.57 higher odds of meeting DSM–III PTSD criteria than the comparison subjects. In the following 2 years, the odds among the veterans with combat stress reactions were 5.15 and 5.41 higher, respectively, than those among comparison subjects. After 20 years, the odds among veterans with combat stress reaction were 3.09 higher than among those of the comparison subjects. When criterion F was added, the odds among combat stress reaction casualties of meeting criteria in the 3 years after the war were 8.64, 11.53, and 9.63, respectively, higher than those among comparison subjects, and 4.68 higher 20 years after the war.
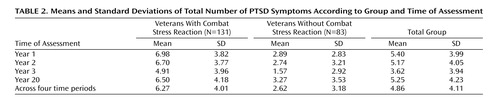
Number of PTSD Symptoms
DSM criteria are customarily used dichotomously to determine the presence or absence of PTSD. In the current study, however, we went beyond the dichotomous diagnosis and took into consideration the number of positively endorsed symptoms in the PTSD inventory as a further index of severity. Table 2 presents the average number of symptoms reported by the participants who met criteria in each study group at each time of measurement. A two-way analysis of variance for study group and time of measurement, with time as a within-subject repeated factor, yielded significant main effects for study group (F=78.91, df=1, 212, p<0.01) and time of measurement (F=23.57, df=3, 636, p<0.01). The interaction term was not significant. As seen in Table 2 , veterans who had had a combat stress reaction endorsed more PTSD symptoms across the four measurement times than those in the comparison group. In addition, Scheffé tests for repeated measures revealed a significantly lower endorsement of PTSD symptoms at year 3 than at year 1 and year 2 and a subsequent significant increase in the endorsement of these symptoms at year 20 ( Table 2 ).
A Qualitative Assessment of Symptom Profiles
This section presents a qualitative analysis of the contribution of combat stress reaction and measurement time to symptom profiles. Figure 1 presents the profile of the individual symptoms in terms of the percentage of subjects in each study group endorsing each symptom at each point of time. Assessment was based on 13 PTSD symptoms, as guilt was defined as both survivor guilt and guilt about functioning.
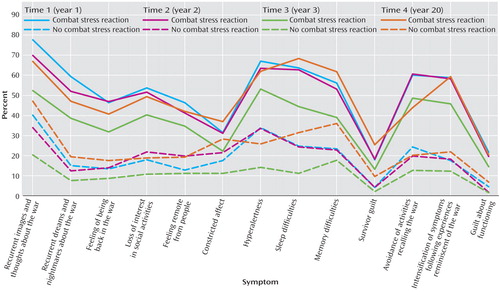
The symptom profile for the combat stress reaction group revealed the following patterns. First, all four curves are almost parallel. Whether symptoms were highly endorsed or less endorsed, they received relatively proportional endorsement at all four points of time. Second, the curves also show that some symptoms are more prevalent than others. Some symptoms, such as recurrent images and thoughts about the war, were endorsed by most of the veterans over the four waves, whereas others, such as survivor guilt, constricted affect, and guilt about functioning, were endorsed by few. Third, PTSD was generally more severe—that is, characterized by a greater number of symptoms—at times 1, 2, and 4 than in year 3.
The symptom profile for the comparison group revealed that the four curves are not so parallel. That is, in the comparison group, the passage of time changed not only the severity of posttraumatic symptoms but also their structure. PTSD at times 1 and 2 was basically characterized by recurrent images and thoughts about the war, hyperalertness, sleep and memory difficulties, avoidance of activities recalling the war, and intensification of symptoms after experiences reminiscent of the war. At year 3, PTSD was characterized by a somewhat different cluster of symptoms. Some of the earlier symptoms continued to be salient (e.g., recurrent images and thoughts about the war, avoidance of activities recalling the war), whereas loss of interest in social activities, feeling remote from people, sleep difficulties, and memory difficulties became relatively more prominent. In year 20, constricted affect and memory difficulties increased.
Trajectories of PTSD
Figure 2 presents the individual trajectories of PTSD in the two study groups. Inspection of the charts reveals that the two groups clearly differed in their longitudinal course of disease. A total of 19.8% (N=26) of the combat stress reaction group versus 61.4% (N=51) of the comparison subjects did not meet criteria at any of the four study waves (χ 2 =38.17, df=1, p<0.01), 11.5% (N=15) of the combat stress reaction group versus 16.8% (N=14) of the comparison subjects met criteria at any one point (χ 2 =1.27, df=1, n.s.), 21.3% (N=28) of the veterans with combat stress reaction and 12% (N=10) of the comparison subjects at any two points (χ 2 =3.03, df=1, n.s.), 27.5% (N=32) of the veterans with combat stress reaction versus 6% (N=5) of the comparison subjects at any three points (χ 2 =15.10, df=1, p<0.01), and 19.8% (N=26)of the veterans with combat stress reaction versus only 3.6% (N=3) of the comparison subjects at all four points of time (χ 2 =11.43, df=1, p<0.01). These results show that posttraumatic residues in the combat stress reaction group were not only more severe but also more stable than among comparable veterans without antecedent combat stress reaction. Although the comparison group was resilient, the combat stress reaction group seemed vulnerable to PTSD.
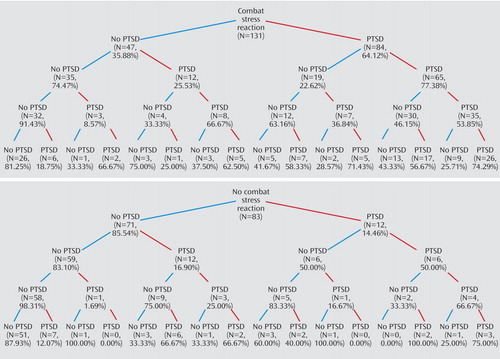
a Figures represent number and percent of veterans meeting criteria for PTSD diagnosis at each point in time for each of the two study groups.
Inspection of the PTSD trajectories presented in Figure 2 revealed fluctuations of PTSD in both groups. Delayed onset, defined here as onset at any point of time after nonendorsement at year 1, was endorsed by 23.8% (N=20) of the comparison subjects and 16.1% (N=21) of combat stress reaction casualties. Of these, 8.4% (N=7) of the comparison subjects and 4.6% (N=6) of the veterans with combat stress reaction endorsed PTSD only at year 20, 1.2% (N=1) of the comparison subjects and 0.8% (N=1) of the veterans with combat stress reaction only at year 3, and 3.6% (N=3) of the comparison subjects and 2.3% (N=3) of the veterans with combat stress reaction only at year 2.
A fluctuating course characterized by relapses/reactivations and remissions was observed in the two study groups. In the combat stress reaction group, 7.6% (N=10) endorsed PTSD once after one remission; in 4.6% (N=6), PTSD reemerged after two remissions; and in 3.8% (N=5), PTSD reemerged after three remissions. Complete remission was observed in 3.8% (N=5), 16.8% (N=22) had two remissions, and 23.7% (N=31) had one remission. In the comparison group, PTSD emerged once in 13.3% (N=11) of the participants, twice in 8.4% (N=7), and three times in 2.4% (N=2). In 3.6% (N=3), there was complete remission; in 3.6% (N=3), PTSD remitted twice; and in 3.6% (N=3), it remitted once.
To assess the prediction of a given trajectory based on group membership (with or without combat stress reaction), a series of logistic regressions was performed. Odds ratios were calculated by dividing the odds of suffering from PTSD in the combat stress reaction group by those in the group without combat stress reaction. The results show that the odds of combat stress reaction casualties endorsing PTSD uninterruptedly are 6.6 times higher than those of veterans without combat stress reaction (odds ratio=6.6, confidence interval [CI]=1.9–22.6; Wald χ 2 =9.05, p<0.01). The odds among casualties without combat stress reaction of not suffering from PTSD at any of the four time points were 6.44 higher than the odds among veterans with combat stress reaction (odds ratio=6.44, CI=3.48–11.92; Wald χ 2 =35.07, p<0.01). The odds of combat stress reaction casualties to relapse once and twice are 8.27 (CI=2.44–28.03; Wald χ 2 =11.50, p<0.01) and 5.88 (CI=1.56–18.60; Wald χ 2 =7.07, p<0.01), respectively, higher than those of veterans without antecedent combat stress reaction.
Discussion
Assessments performed 1, 2, 3, and 20 years after combat revealed both considerable posttraumatic residues in the two groups and overwhelmingly more enduring posttraumatic symptoms among combat stress reaction casualties than among veterans without combat stress reaction.
Although posttraumatic symptoms among the combat stress reaction casualties appear to be high, there is little in the literature to serve as a normative basis for comparison. Other than studies conducted by our group in Israel (e.g., reference 3 ), we know of no study that directly assessed the connection between combat stress reaction and PTSD. Nonetheless, studies of Vietnam veterans (without reference to whether or not they had had a combat stress reaction episode) found PTSD rates ranging from 15% to 48% (e.g., references 7 , 15) . Large-scale epidemiological studies of American civilians (e.g., reference 6 ) also found combat exposure to be associated with a high probability of PTSD.
The rates of posttraumatic symptoms in our comparison group must be interpreted cautiously. This group was chosen on the basis of its similarity to the combat stress reaction group and may or may not be a representative sample of Israeli combatants who fought in the Lebanon War. The possibility that some of the comparison soldiers may have suffered an unreported combat stress reaction incident cannot be negated. However, the characteristics of battle make it impossible to obtain better criteria than the referral to psychiatric intervention. Furthermore, since a combat stress reaction episode is quite visible and thus unlikely to be overlooked on the battlefield where it endangers other people, there is good reason to believe that the number of unidentified combat stress reaction cases in the comparison group is quite negligible. It should be noted that the majority of the comparison veterans did not exhibit PTSD. This is in line with previous studies (e.g., references 16 , 17) and suggests that, in general, resilience in the face of trauma is a common response.
The differences in PTSD observed in the combat stress reaction and comparison groups were both quantitative and qualitative. The two groups differed not only in rates but also in the number of symptoms. At all four times, the veterans with combat stress reaction endorsed more posttraumatic symptoms than the veterans without combat stress reaction, and these symptoms were more severe.
One possible explanation is that the severe psychological distress on the battlefield is not a minor wound but represents a major rupture. Combat stress reaction is the culmination and epitome of a process in which the individual is stripped of his sense of safety and mastery and experiences the full thrust of his vulnerability and existential helplessness. Conversely, the more enduring and intense PTSD among the combat stress reaction casualties might be indicative of this group’s greater initial vulnerability. It is conceivable that people who had both severe emotional difficulties in combat and suffered a subsequent posttraumatic disorder were initially less resilient than soldiers who did not suffer from such difficulties on the battlefield. Practically speaking, however, the combat stress reaction and comparison groups did not significantly differ in premilitary screening of physical and psychiatric symptoms. Based on these data, one cannot negate any of these explanations, but it is more likely that in our group, combat stress reaction is implicated in the genesis of PTSD and does not necessarily imply prewar vulnerability. In any event, these findings suggest that individuals who succumb to battle stress need and deserve clinical monitoring and attention.
Combat stress reaction, unlike acute stress disorder, is diagnosed solely on the basis of dysfunction rather than a defined set of symptoms and reflects the individual’s inability to contain his fear response and restore homeostasis. Therefore, we suggest that this peritraumatic impaired functioning may be an important vulnerability marker.
Our longitudinal data show that in both study groups the number of symptoms dropped radically in the third year and rose again in the fourth wave—17 years later. Such a drop in symptoms has been reported in several retrospective (e.g., reference 6 ) and prospective (e.g., reference 8 ) studies and was explained by the healing effect of time. The unexpected increase in posttraumatic symptoms 20 years after the war may be related to the interplay of posttraumatic residual vulnerability, the course of disease, the aging process, and the unremitting threats of terror in Israel. The chronic nature of PTSD renders trauma victims vulnerable for life, and midlife is a particularly high-risk period for either delayed onset or reactivated PTSD. Midlife generally entails some reduction in activity and a shift from planning to reminisce and from occupation with current events to the review and rethinking of one’s life. In the course of this transition, the altered perspective may force the forgotten or suppressed traumatic memories up to the foreground again (18) . In addition, aging inevitably entails many losses and exit events, from retirement through disease. Such painful events entail loss of structure, routine, self-esteem, status, and social interaction and bring down some of the protective shields that trauma survivors have against being flooded by memories. Finally, the fourth wave of measurement took place during the most stressful period of intifada-related terrorist attacks (the summer of 2002) that continuously confronted these men with major new trauma experienced by civilians and by young soldiers who were mostly of their own age at the time of the Lebanon War. The precarious security situation permeated every area of life and was extensively covered by the media. Such a constant undercurrent of threat inevitably causes distress, especially for combat stress reaction casualties who are highly sensitized to anything that recalls their war experience and may exacerbate their symptoms. Research has consistently indicated that the recovery environment plays an important role in the maintenance and reactivation of symptoms (3 , 19 , 20) .
Of interest, the addition of the F criterion changed the pattern of results. In the combat stress reaction group, whereas symptoms increased from year 3 to year 20, the inclusion of disability/distress led to a decrease in the PTSD rate. In the comparison group, however, a marked increase in symptoms was noted in year 20, and when the F criterion was added, the rate of PTSD was lowered, but still an increase between year 3 and year 20 was observed. It seems that time may have a different effect on veterans who initially coped well and were able to contain their responses.
Qualitative analyses of the longitudinal data also suggest that the composition of symptoms in the comparison group somewhat varied between the four waves of measurement. Why this variation was mainly found in the comparison group and not in the combat stress reaction group requires further explanation. One possibility involves the fact that all the men in the combat stress reaction group received at least some treatment after a visible and disturbing emotional response. It is reasonable to suppose that psychotherapy would have kept the traumatic event well in recall and discouraged suppression. Another explanation is that the trauma of the combat stress reaction itself may have made the trauma of the war harder to suppress.
The two study groups also differed in the course of PTSD. Veterans with antecedent combat stress reaction were 6.6 times more likely to endorse posttraumatic symptoms uninterruptedly at all four time points compared to veterans with no such history. Fluctuations in the course of PTSD were found in both study groups. Yet the veterans with combat stress reaction were at a much higher risk for exacerbation/reactivation at all four time points. Even when veterans with combat stress reaction did not meet symptom criteria, they had some residual symptoms that did not remit. Similarly, McFarlane and Papay (9) found that the chronic course of symptoms differed in a clinical sample from that of a nonclinical sample.
Delayed onset in the comparison group was quite prevalent (23.8%) and increased with time. Previous studies had reported a wide range of prevalence of delayed onset in a variety of populations, ranging from 5% (21) to 20% (22 , 23) . Delayed onset of PTSD, which is often met with skepticism in medicolegal circles, is evidently empirically documented. Rates of delayed onset vary according to the population studied, the nature of the traumatic event, the posttraumatic environment, and the length of follow-up. It is plausible that the relatively longer follow-up in the present study and aging may account for the preponderance of delayed onset. This finding, which needs to be validated in long-term follow-ups in other cohorts, calls for professional attention to be given to aging individuals who were severely traumatized in their youth.
This study suffers from a number of methodological limitations, such as its attrition rate, outcome measures based on the outdated DSM–III, self-report measures, and the use of data of only veterans who participated in the four waves of measurement. It is possible that the use of self-report measures might have contributed to an inflation in the report of PTSD symptoms. Accordingly, it is possible that those veterans with combat stress reaction who participated in the four waves of measurement showed more difficulties in recovering from PTSD than those who did not participate, thereby contributing to an inflation of endorsement of PTSD symptoms. In addition, the postwar environment and particularly the recent intifada may have affected the results, reactivating war-related memories and then exacerbating the report of PTSD symptoms 20 years after the Lebanon War. Finally, our measurements did not cover the entire span of 20 years since the war. Therefore, we were unable to monitor the entire spectrum of changes in the course of PTSD between 1985 and 2002, and we cannot explore the possible impact of different war-related events (e.g., withdrawal from Lebanon, the first intifada, the Gulf War, the second intifada) on PTSD severity. Despite these limitations, however, the contribution of this prospective study to the understanding of PTSD cannot be underestimated. The findings here suggest that the detrimental effects of combat are deep and enduring and follow a complex course, especially in combat stress reaction casualties. PTSD, being the only disorder that distinctly stems from exposure to an external traumatic event, often entails medicolegal and political implications for soldiers who are sent by their nations to war. Our findings suggest that these men need long-term monitoring and professional attention. Finally, the exacerbating effects of aging that reawake past traumatic wounds, as well as the implications of a stressful postwar environment such as the ongoing state of terror, raise the need to increase awareness with regard to war-induced PTSD.
1. Kardiner A: War Stress and Neurotic Illness. New York, Paul Hoeber, 1947Google Scholar
2. Grinker RR, Spiegel JP: Men Under Stress. Philadelphia, Blakiston, 1945Google Scholar
3. Solomon Z: Combat Stress Reaction—The Enduring Toll of War. New York, Plenum, 1993Google Scholar
4. Horowitz MJ, Solomon GF: Delayed stress response syndromes in Vietnam veterans, in Stress Disorders Among Vietnam Veterans: Theory, Research and Treatment. Edited by Figley CR. New York, Brunner/Mazel, 1978, pp 268–280Google Scholar
5. Van Dyke C, Zilberg NJ, McKinnon JA: Posttraumatic stress disorder; a thirty-year delay in a World War II veteran. Am J Psychiatry 1985; 142:1070–1073Google Scholar
6. Kessler RC, Broment E, Hughes M: Posttraumatic stress disorder in the national comorbidity survey. Arch Gen Psychiatry 1995; 52:1048–1060Google Scholar
7. Kulka RA, Schlenger WE, Fairbank JA, et al: Trauma and the Vietnam War Generation: Report of Findings from the National Vietnam Veterans Readjustment Study. New York, Brunner/Mazel, 1990Google Scholar
8. Grace MC, Green BL, Lindy JD, et al: The Buffalo Creek disaster: a 14-year follow-up, in International Handbook of Traumatic Stress Syndromes. Edited by Wilson JP, Raphael B. New York, Plenum, 1993, pp 441–449Google Scholar
9. McFarlane AC, Papay P: Multiple diagnoses in posttraumatic stress disorder in the victims of a natural disaster. J Nerv Ment Dis 1992; 180:498–504Google Scholar
10. Harvey AG, Bryant RA: The relationship between acute stress disorder and posttraumatic stress disorder: a 2-year prospective evaluation. J Consult Clin Psychol 1999; 67:985–988Google Scholar
11. Barton KA, Blanchard EB, Hickling EJ: Antecedents and consequences of acute stress disorder among motor vehicle accident victims. Behav Res Ther 1996; 34:805–813Google Scholar
12. Solomon Z, Benbenishty R: The role of proximity, immediacy, and expectancy in frontline treatment of combat stress reaction among Israelis in the Lebanon War. Am J Psychiatry 1986; 143:613–617Google Scholar
13. Derogatis LR: The SCL-90-R Manual I: Scoring, Administration, and Procedure for the SCL-90. Baltimore, Johns Hopkins University, School of Medicine, 1977Google Scholar
14. Solomon Z, Mikulincer M: Combat stress reaction, PTSD and social adjustment: a study of Israeli veterans. J Nerv Ment Dis 1987; 175:277–285Google Scholar
15. Egendorf A, Kadushin C, Laufer R: Legacies of Vietnam: Comparative of Veterans and Their Peers. Vol I.IV, U5. Washington, DC, US Government Printing Office, 1981Google Scholar
16. Bonnano GA: Loss, trauma and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol 2004; 59:20–28Google Scholar
17. Elder GH Jr, Clipp EC: Combat experience and emotional health: impairment and resilience in later life. J Pers 1989; 57:311–341Google Scholar
18. Green BL, Lindy JD, Grace MC, et al: Buffalo creek survivors in the second decade: stability of stress symptoms. Am J Orthopsychiatry 1990; 60:43–54Google Scholar
19. Brewin CR, Dalglish T, Joseph SA: A dual representation theory of posttraumatic stress disorder. Psychol Rev 1996; 103:670–686Google Scholar
20. Hertz DG: Trauma and nostalgia: new aspects on the coping of aging holocaust survivors. Isr J Psychiatry Relat Sci 1990; 27:189–198Google Scholar
21. Bryant RA, Harvey AG: Delayed-onset posttraumatic stress disorder: a prospective evaluation. Aust NZ J Psychiatry 2002; 36:205–209Google Scholar
22. McFarlane AC: The longitudinal course of posttraumatic morbidity: the range of outcomes and their predictors. J Nerv Ment Dis 1988; 176:30–39Google Scholar
23. Wolfe J, Erickson DJ, Sharkansky EJ, et al: Course and predictors of posttraumatic stress disorder among gulf veterans: a prospective analysis. J Consult Clin Psychol 1999; 67:520–528Google Scholar

