
Disrupted Reinforcement Signaling in the Orbitofrontal Cortex and Caudate in Youths With Conduct Disorder or Oppositional Defiant Disorder and a High Level of Psychopathic Traits
Abstract
Objective:
Dysfunction in the amygdala and orbitofrontal cortex has been reported in youths and adults with psychopathic traits. The specific nature of the functional irregularities within these structures remains poorly understood. The authors used a passive avoidance task to examine the responsiveness of these systems to early stimulus-reinforcement exposure, when prediction errors are greatest and learning maximized, and to reward in youths with psychopathic traits and comparison youths.
Method:
While performing the passive avoidance learning task, 15 youths with conduct disorder or oppositional defiant disorder plus a high level of psychopathic traits and 15 healthy subjects completed a 3.0-T fMRI scan.
Results:
Relative to the comparison youths, the youths with a disruptive behavior disorder plus psychopathic traits showed less orbitofrontal responsiveness both to early stimulus-reinforcement exposure and to rewards, as well as less caudate response to early stimulus-reinforcement exposure. There were no group differences in amygdala responsiveness to these two task measures, but amygdala responsiveness throughout the task was lower in the youths with psychopathic traits.
Conclusions:
Compromised sensitivity to early reinforcement information in the orbitofrontal cortex and caudate and to reward outcome information in the orbitofrontal cortex of youths with conduct disorder or oppositional defiant disorder plus psychopathic traits suggests that the integrated functioning of the amygdala, caudate, and orbitofrontal cortex may be disrupted. This provides a functional neural basis for why such youths are more likely to repeat disadvantageous decisions. New treatment possibilities are raised, as pharmacologic modulations of serotonin and dopamine can affect this form of learning.
Youths with conduct disorder and oppositional defiant disorder show high rates of aggressive and antisocial behaviors (1). A subset of these youths also display callousness and psychopathic traits, including lack of guilt, empathy, and remorse (2, 3). This subset of youths is at highest risk for recurrent antisocial acts and future criminal behaviors (3–6). While psychopathic traits are detectable early in childhood and persist into adulthood (7), little is known about the pathophysiology (8–10).
The presence of psychopathic traits has long been linked to problems in emotional learning (11, 12). Specifically, it has been argued that these traits reflect impairment in stimulus-reinforcement learning and in decision making (13, 14). An early task indexing this impairment was the passive avoidance task (11, 15, 16). Passive avoidance tasks require participants to learn to respond to (i.e., approach) stimuli that engender reward and refrain from responding to (i.e., passively avoid) stimuli that engender punishment. Adults and youths with psychopathic traits show a deficient capability to learn to avoid the stimuli that predict punishment regardless of whether the punishment is shock, loss of money, or loss of points (11, 15, 16).
Passive avoidance learning tasks are particularly informative, as both electrophysiologic and lesion studies map its neural basis, implicating the amygdala, orbitofrontal cortex, and striatum (17–21). In addition, a functional magnetic resonance imaging (fMRI) study of a passive avoidance task has confirmed the importance of these regions in healthy human adults (22). It is argued that the amygdala allows the formation of stimulus-reinforcement associations, determining which of the stimuli are “good” and which “bad,” and that this information is fed forward as reinforcement expectations to the orbitofrontal cortex (19–21), potentially via the ventral striatum (23). The orbitofrontal cortex is critical for the representation of this reinforcement-expectation information, thereby facilitating successful decision making (24, 25). The orbitofrontal cortex and caudate are also critical for error prediction, which facilitates learning of reward or punishment contingencies (26–28). The detection of prediction errors prompts enhanced reinforcement-based learning (29). These prediction errors are maximal after the individual's first exposure to the cue and reinforcement but rapidly lessen (unless the reinforcement contingency changes) as the individual develops an expectation of the reinforcement associated with the cue (29).
Originally, the deficits shown by individuals with psychopathic traits on passive avoidance tasks were attributed to less processing of punishment information (11). However, work has shown that individuals with psychopathic traits appropriately use punishment information to modify responses immediately following an error. Instead, it is argued that the deficits arise from impairment in the formation and use of stimulus-reinforcement associations in decision making (30). The individual with psychopathic traits is less able to use reinforcement information to change his or her representation of the outcome associated with the response and consequently is less able to use reinforcement expectancies to guide behavior (13). A deficit in stimulus-reinforcement processing is thought to result from dysfunction in the integrated functioning of the amygdala and orbitofrontal cortex (13). In line with this model, recent fMRI work has indicated less amygdala responding and less amygdala-orbitofrontal cortex functional connectivity in response to fearful expressions in youths with psychopathic traits than in comparison subjects (8, 9). Moreover, anomalous neural responses in the orbitofrontal cortex to reversal errors have also been identified in this population (10).
The goal of the current study was to assess the nature of the functional irregularities within the amygdala, orbitofrontal cortex, and striatum of youths with conduct disorder or oppositional defiant disorder plus psychopathic traits. Specifically, the study tested three hypotheses. First, we hypothesized that early reinforcement processing would be abnormal in these youths. For initial exposures to reinforced outcomes, prediction errors are high; the participant has no reinforcement expectancy associated with the stimulus, and thus all reinforcement received is unexpected (29). Healthy individuals show marked increases in activity, particularly within the orbitofrontal cortex and striatum, in response to unexpected reinforcements (26–28). We predicted, however, that this initial heightened responding to early trials would not be seen in the subjects with conduct disorder or oppositional defiant disorder plus psychopathic traits, at least within the orbitofrontal cortex. Our second hypothesis was that the signaling associated with reward and punishment outcomes would be abnormal in this group. Several studies have documented heightened responses to rewarded relative to punished outcomes within the amygdala, orbitofrontal cortex, and striatum during decision making (23, 24, 31). We predicted that this heightened responding to rewarded outcomes would be seen only in the healthy youths and not in those with conduct disorder or oppositional defiant disorder plus psychopathic traits.
Method
Participants
Thirty youths participated in this study: 15 youths with psychopathic traits and either conduct disorder or oppositional defiant disorder and 15 healthy comparison youths (Table 1). Youths were recruited from the community through newspaper ads, fliers, and referrals from mental health practitioners in the area. Statements of informed assent and consent were obtained from the participating children and parents. This study was approved by the institutional review board of the National Institute of Mental Health.
| Characteristic | Youths With Conduct Disorder or Oppositional Defiant Disorder Plus Psychopathic Traits (N=15) | Healthy Comparison Group (N=15) | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age (years) | 14.1 | 1.8 | 13.2 | 1.1 |
| IQa | 100.3 | 10.5 | 108.2 | 14.6 |
| Scores on pediatric psychopathy scales | ||||
| Antisocial Process Screening Device (32) | 28.9 | 4.0 | 6.9 | 4.1 |
| Psychopathy Checklist: Youth Version (5) | 24.7 | 3.1 | — | |
| N | % | N | % | |
| Male sex | 9 | 60 | 9 | 60 |
| DSM-IV diagnoses (current) | ||||
| Conduct disorder | 9 | 60 | 0 | 0 |
| Oppositional defiant disorder | 6 | 40 | 0 | 0 |
| Attention deficit hyperactivity disorder | 10 | 67 | 0 | 0 |
TABLE 1. Characteristics of Youths With Conduct Disorder or Oppositional Defiant Disorder Plus Psychopathic Traits and Healthy Youths
All youths and parents completed the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL) (33) with an experienced clinician trained and supervised by expert child psychiatrists, with good interrater reliability (kappa higher than 0.75 for all diagnoses). IQ was assessed with the Wechsler Abbreviated Scale of Intelligence (two-subtest form). The exclusion criteria were pervasive developmental disorder, Tourette's syndrome, depression, bipolar disorder, generalized, social, or separation anxiety disorder, posttraumatic stress disorder, neurologic disorder, lifetime history of psychosis, history of head trauma, and an IQ under 80. In addition, the parents also completed the Antisocial Process Screening Device (32), a measure of psychopathic traits. Youths meeting the K-SADS-PL criteria for conduct disorder or oppositional defiant disorder who had scores of 20 or higher on the Antisocial Process Screening Device returned to complete the Psychopathy Checklist: Youth Version (5). Youths scoring 20 or higher on this instrument were included in the psychopathic traits group; those scoring less than 20 were excluded from the study. The comparison subjects did not meet the criteria for any K-SADS-PL diagnosis and scored below 20 on the Antisocial Process Screening Device.
Clinical Measures
Antisocial Process Screening Device.
This is a 20-item parent-completed rating of callous-unemotional traits and conduct and impulsivity problems (32), designed to detect antisocial processes in youths. A three-factor structure has been characterized and comprises the following dimensions: callous/unemotional, narcissism, and impulsivity (32). There is no established cutoff score for classification of a high level of psychopathic traits (32, 34, 35). For research purposes, studies of adolescents have used a cutoff score of 20 (8, 10, 36), median splits (higher than 11 for males, 9 for females) (37), or percentile rankings (top one-third, score above 18) (35). Following our previous work (8, 10), we used a score of 20 or higher in this study. All of the healthy comparison subjects scored less than 15 on this measure.
Psychopathy Checklist: Youth Version.
This is a 20-item rating scale for assessing interpersonal, affective, and behavioral features related to psychopathic traits in adolescents (5). It is based on a semistructured interview and collateral information. A score of 20 or higher was used to define the group with high levels of psychopathic traits (8, 10), as there are no standard cutoff scores for classifying youths on this measure to date (5).
The fMRI passive avoidance task.
A modified version of the previously reported fMRI passive avoidance task was used (Figure 1) (22, 38). The characteristics of the task were equivalent to those used in a previous study (38) with the exception that eight stimuli, rather than 12, were presented in each fMRI run. Each of the four runs involved a new set of eight stimuli for the participant to learn about. Trials began with the presentation for 1,100 msec of one of these eight stimuli (Snodgrass line drawings [39] on a black background). Button press responses to four of the stimuli engendered a reward (“You WIN 100 points”). Button presses in response to the other four stimuli engendered punishment (“You LOSE 100 points”). If no response was made, a fixation cross was presented in lieu of reinforcement. The reinforcement phase (reward, punishment, or fixation cross) lasted for 1,000 msec. Following this, there was a 200-msec fixation cross before the commencement of the next trial. The participant's goal was to win as many points as possible; the subject had to learn to respond to the stimuli engendering reward and withhold from responding to the stimuli engendering punishment.
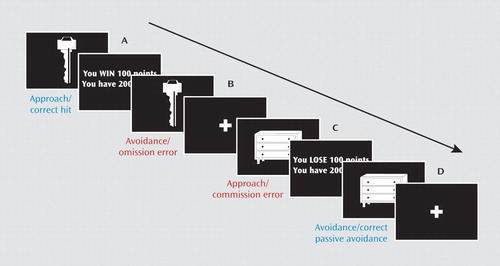
a Participants received the following instructions: “In this task, you are going to be presented with a series of images. Some of these images are good and will gain you points if you press the button when they are showing. Some are bad and will lose you points if you press the button when they are showing. If you do nothing you will neither gain nor lose points. Your goal is to win as many points as you can.” Four types of events were possible. Event A demonstrates a correct hit: the participant is presented with a stimulus (key) associated with reward. Upon responding to this stimulus with a mouse click (“approach”), the participant is presented with positive feedback. Event B represents an omission error: upon presentation of a stimulus associated with reward, the participant does not make any response (“avoidance”). A fi xation cross is presented during the feedback interval. Event C shows a commission error: a stimulus (dresser) associated with punishment is presented, and the participant responds with a mouse click, resulting in the display of negative feedback. Event D demonstrates correct passive avoidance: the participant refrains from responding to a stimulus associated with punishment, and a fixation cross is presented during the feedback interval.
The stimuli were presented in random order once per block for eight acquisition blocks. After the eight acquisition blocks, the reinforcement value associated with one-half of the stimuli changed (this extinction component of the study will be considered in a separate article). Within each block of eight stimuli, there were an additional four fixation point trials (with 2,300 msec of the fixation point) to serve as a baseline. Each of the fMRI runs contained a different set of eight stimuli.
Each participant completed a brief practice session and then four runs of the task in a scanner. Four versions of the task were developed to counterbalance the reinforcements associated with each of the stimuli. The task version and run order were randomized across participants.
MRI Characteristics
During task performance the participants were scanned with a 3.0-T GE Signa scanner (GE Healthcare Systems, Fairfield, Conn.). A total of 189 functional images per run were taken with a gradient echo planar imaging (EPI) sequence, with a repetition time of 2,300 msec, echo time of 23 msec, 64×64 matrix, flip angle of 90°, and 24-cm field of view. Whole-brain coverage was obtained with 34 axial slices (thickness, 3.3 mm). A high-resolution anatomical scan (three-dimensional fast spoiled gradient echo sequence; repetition time=6 msec, echo time=2.5 msec, field of view=24 cm, flip angle=12°, 124 axial slices, thickness=1.0 mm, 224×224 matrix) in register with the EPI data set and covering the whole brain was obtained.
Imaging Data Preprocessing
Imaging data were preprocessed and analyzed with AFNI software (40). At the individual level, functional images from the first five volumes of each run, collected before equilibrium magnetization was reached, were discarded. Functional images from the four time series were motion corrected and spatially smoothed with a 6-mm full-width half-maximum Gaussian filter. The time series were normalized by dividing the signal intensity of a voxel at each time point by the mean signal intensity of that voxel for each run and multiplying the result by 100. The resultant regression coefficient represented a percentage signal change from the mean.
Following this, regressors characterizing the trial and response types were generated: correct hits (responses to stimuli associated with reward), commission errors (responses to stimuli associated with punishment), correct avoidances (no response to stimuli associated with punishment), and omission errors (no response to stimuli associated with reward). To examine differential responsiveness to initial exposures, as opposed to later learning, we evaluated neural responses during the exposures to the stimulus-reinforcement associations in block 1 in comparison to exposures in blocks 2–8.
All regressors were created by convolving the train of stimulus events with a gamma-variate hemodynamic response function to account for the slow hemodynamic response. Linear regression modeling was performed by using the aforementioned regressors plus regressors to model a first-order baseline drift function. This produced a beta coefficient and associated t statistic for each voxel and regressor. In accordance with findings that normalization of brain volumes from age 7–8 years onward does not introduce major age-related distortions in localization or time course of the blood-oxygen-level-dependent (BOLD) signal in event-related fMRI (41, 42), the participants' anatomical scans were individually registered to the Talaraich and Tournoux atlas (43). The individuals' functional imaging data were then registered to their Talaraich-fit anatomical scans within AFNI.
fMRI Data Analysis
The group analysis of the BOLD data was then performed on the regression coefficients from the analyses for the individual subjects by means of a 2×2×2 analysis of variance (ANOVA). The three variables were diagnosis (psychopathic traits versus comparison subjects), response type (correct hits versus commission errors), and learning phase (early [block 1] versus late [blocks 2–8]). The initial probability threshold was set at p<0.005 (corrected at p<0.05 for multiple comparisons). Extent-threshold correction for multiple comparisons was done by using the AlphaSim program in AFNI. Average percentage signal change was measured within each significant cluster of 547 mm3 or greater. Post hoc analysis of significant interactions was performed with planned ANOVAs within SPSS (SPSS, Chicago).
Results
Behavioral Results
There were no significant group differences in age or IQ (Table 1). The 2×2×2 analysis of group differences in -omission and commission errors revealed the expected interaction of diagnosis, learning phase, and error type (F=4.6, df=1, 28, p<0.05). The youths with conduct disorder or oppositional defiant disorder plus psychopathic traits made significantly more commission errors than the comparison subjects during the late learning phase (F=5.4, df=1, 28, p<0.05) (Figure 2); the mean numbers of commission errors per block in the early phase were 3.31 (SD=0.39) and 3.65 (SD=0.62), respectively, and during the late phase the mean numbers were 1.15 (SD=0.79) and 0.05 (SD=0.23). There was also a significant interaction of diagnosis and learning phase (F=10.5, df=1, 28, p<0.005); the youths with psychopathic traits made significantly more errors during the late learning phase than the comparison subjects (F=7.4, df=1, 28, p<0.01). There was no main effect of diagnosis.
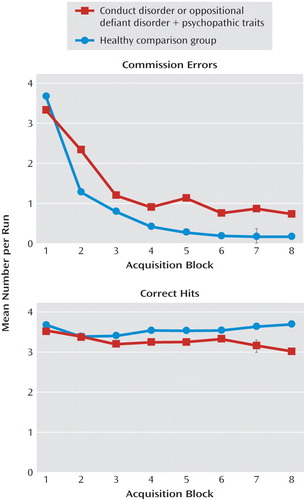
a The youths with psychopathic traits made significantly more errors in the late blocks (blocks 2–8) compared with the healthy youths.
“Meghan” is a 14-year-old girl with a history of disruptive behaviors since the age of 5. Her parents report that despite being a bright and charming child, she has a long history of delinquent behaviors, including shoplifting expensive items, joyriding alone in her parents' car, threatening her little sister with a knife, and promiscuous sexual behavior. Her parents describe her as completely self-centered, extremely manipulative, and a pathologic liar. She does not demonstrate empathy for her family and according to her parents, shows no remorse or guilt for her actions. Meghan describes herself as popular and smart and able to get A's in school when she wants to. However, according to her parents she receives mainly C's and D's on her report card and has had no significant friendships.
fMRI Results
The goal of the current study was to assess the nature of the functional irregularities within the amygdala, orbitofrontal cortex, and striatum in youths with conduct disorder or oppositional defiant disorder plus psychopathic traits during passive avoidance learning. We examined this issue through a 2×2×2 ANOVA conducted on the BOLD response data, with diagnosis (conduct disorder or oppositional defiant disorder plus psychopathic traits versus comparison subjects), learning phase (early or late: block 1 versus blocks 2–8), and response type (commission error versus correct hit) (Table 2). The key interactions with respect to our predictions (diagnosis-by-phase and diagnosis-by-response interactions) and the main effect of diagnosis are described in the following to provide results for the test of our a priori hypotheses. No significant finding occurred for the three-way diagnosis-by-phase-by-response interaction.
| Coordinates of Peak Activationc | |||||||
|---|---|---|---|---|---|---|---|
| Regiona,b | Left/Right | Brodmann's Areaa | x | y | z | F (df=1, 28) | Volume (mm3) |
| Diagnosis-by-phase interactions | |||||||
| Orbitofrontal cortex | Right | 11 | 23 | 36 | −13 | 14.4 | 675 |
| Middle frontal gyrus | Left | 10 | −32 | 41 | 25 | 24.0 | 3,834 |
| Superior frontal gyrus | Left | 8 | −17 | 46 | 44 | 15.5 | 4,863 |
| Left | 6 | −29 | −4 | 45 | 15.2 | 1,269 | |
| Inferior frontal gyrus | Right | 46 | 50 | 38 | 11 | 17.7 | 3,942 |
| Left | 44 | −59 | 13 | 20 | 14.4 | 1,836 | |
| Inferior parietal lobule | Left | 7 | −41 | −69 | 45 | 16.8 | 3,159 |
| Middle temporal gyrus | Right | 39 | 47 | −58 | 10 | 18.9 | 2,808 |
| Right | 21 | 44 | 3 | −33 | 21.0 | 2,106 | |
| Middle temporal/angular gyrus | Left | 39 | −50 | −54 | 3 | 19.4 | 8,289 |
| Caudate | Left | −2 | 16 | 13 | 13.3 | 1,458 | |
| Cerebellum | Left | −4 | −50 | −25 | 27.6 | 7,371 | |
| Diagnosis-by-response type interactionsd | |||||||
| Orbitofrontal cortex | Right | 10 | 5 | 64 | −8 | 12.3 | 162 |
| Middle frontal gyrus | Left | 8 | −44 | 12 | 49 | 13.6 | 486 |
| Parahippocampal gyrus | Right | 37 | 35 | −41 | −10 | 11.9 | 216 |
| Main effect of diagnosis | |||||||
| Superior frontal gyrus | Right | 6 | 11 | 26 | 66 | 17.4 | 2,538 |
| Left | 6 | −8 | 1 | 68 | 17.3 | 6,183 | |
| Right | 6 | 47 | 2 | 49 | 18.5 | 1,701 | |
| Right | 6 | 37 | 14 | 66 | 15.8 | 1,269 | |
| Medial frontal gyrus | Right | 8 | 11 | 27 | 43 | 13.2 | 1,134 |
| Middle frontal gyrus | Left | 10 | −35 | 47 | 28 | 12.3 | 1,350 |
| Inferior frontal gyrus/insula | Right | 44 | 44 | 13 | 13 | 12.6 | 945 |
| Insula | Left | 13 | −41 | 14 | 0 | 14.6 | 2,295 |
| Superior parietal lobule | Left | 7 | −35 | −72 | 45 | 18.7 | 5,508 |
| Superior temporal gyrus | Left | 22 | −53 | −33 | 4 | 20.5 | 7,992 |
| Middle temporal gyrus | Right | 39 | 44 | −64 | 19 | 16.5 | 4,482 |
| Lingual gyrus | Left | 18 | −20 | −88 | −13 | 14.1 | 1,890 |
| Fusiform gyrus | Right | 19 | 32 | −81 | −20 | 23.8 | 13,041 |
| Amygdala | Right | 20 | −10 | −26 | 10.7 | 216 | |
| Caudate | Left | −8 | 7 | 16 | 16.8 | 12,204 | |
| Thalamus/pulvinar | Right | 5 | −30 | 8 | 13.9 | 1,026 | |
TABLE 2. Brain Regions Demonstrating Differential BOLD Responses During Acquisition of Passive Avoidance Learning in 15 Youths With Conduct Disorder or Oppositional Defiant Disorder Plus Psychopathic Traits and 15 Healthy Youths
Our first interaction of interest, the diagnosis-by-phase interaction, examined whether the youths with conduct disorder or oppositional defiant disorder plus psychopathic traits showed atypical BOLD responses during early trial learning. In line with predictions, significant diagnosis-by-phase interactions were observed within the orbitofrontal cortex and the caudate (although not within the amygdala). In addition, significant diagnosis-by-phase interactions were seen in a network of attentional regions, including the inferior frontal cortex, middle frontal gyrus, and inferior parietal lobule (Table 2). In all the regions identified by this interaction, the comparison subjects showed greater activity during the early, but not late, trials relative to the youths with a disruptive behavior disorder plus psychopathic traits. Findings for the orbitofrontal cortex (Brodmann's area 11) (early: t=3.2, df=28, p<0.005; late: n.s.) and the caudate (early: t=4.2, df=28, p<0.001; late: n.s.) are shown in Figure 3.

a The early phase was defined as block 1; the late phase was defined as blocks 2–8. In both regions, the youths with one of the behavior disorders plus psychopathic traits had less mean BOLD activation during the early learning phase in comparison to the healthy youths.
Our second interaction of interest, the diagnosis-by-response type interaction, examined whether the youths with a behavior disorder plus psychopathic traits showed atypical BOLD responses to rewarded correct hits relative to the responses to punished commission errors. Significant diagnosis-by-response type interactions were observed within an anterior region of the orbitofrontal cortex, middle frontal gyrus, and parahippocampal gyrus (Table 2). Within the orbitofrontal cortex, the youths with psychopathic traits showed less activation during rewarded correct hits than the comparison subjects (F=4.6, df=1, 29, p<0.05) (Figure 4), while the responses during punished commission errors were comparable (F<1.0, df=1, 29, p=0.82). In contrast, in the left middle frontal and right parahippocampal gyrus, the comparison subjects showed greater activation during commission errors than did the youths with a behavior disorder plus psychopathic traits (left middle frontal gyrus: F=14.2, df=1, 29, p<0.001; right parahippocampal gyrus: F=5.4, df=1, 29, p<0.05), while activation during correct hits was comparable in the two groups (F<1.0, df=1, 29).
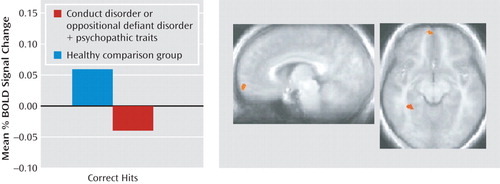
a Brodmann's area 10.
b In comparison to the healthy youths, those with psychopathic traits showed less activation during rewarded responses.
In addition, there was a significant main effect of diagnosis within the amygdala, caudate, insula, and a network of regions implicated in attention processes, including the dorsolateral prefrontal cortex and parietal cortex (Table 2, figure in online data supplement). In all of these regions, the youths with a behavior disorder plus psychopathic traits showed significantly less activation than the comparison subjects.
To account for possible effects of medication use on the BOLD responses, the preceding analysis was repeated without the seven youths in the group with psychopathic traits who were taking medication and their seven age- and IQ-matched comparison subjects. The preceding effects of interest were replicated. Thus, the diagnosis-by-phase interaction was replicated in the middle orbitofrontal cortex; the group with psychopathic traits showed less early activation than the comparison subjects. Similarly, the diagnosis-by-response type interaction was observed in the orbitofrontal cortex. Moreover, the main effects of diagnosis in the amygdala, caudate, and dorsolateral prefrontal cortex again revealed less activation in the youths with conduct disorder or oppositional defiant disorder plus psychopathic traits than in the comparison subjects.
Discussion
The goal of the current study was to assess the nature of the irregularities within the amygdala, orbitofrontal cortex, and striatum in youths with conduct disorder or oppositional defiant disorder plus psychopathic traits during passive avoidance learning. Specifically, this study examined group differences in neural responses to two features critical to emotional learning: the level of experience with the stimulus (early versus late trials) and the type of response and reinforcement (rewarded correct responses versus punished incorrect responses). The results revealed that the youths with psychopathic traits, relative to healthy youths, showed significantly less activity within the orbitofrontal cortex and caudate in response to early exposures to reinforced outcomes. Moreover, in response to rewarded correct responses, the group with psychopathic traits showed significantly less activity within the orbitofrontal cortex than did the comparison youths. These task measures did not reveal group differences within the amygdala, although the group with psychopathic traits had generally lower activity within this region across the task.
Impairments in passive avoidance have been repeatedly reported in individuals with psychopathic traits (11, 15, 16, 44). Our model of passive avoidance learning and its dysfunction in individuals with psychopathic traits is highly influenced by the work of Schoenbaum, Gallagher, and colleagues (19, 45, 46). In essence, we assume that in healthy individuals prediction errors in response to unexpected reinforcements (mediated by the orbitofrontal cortex and caudate) serve to initiate rapid stimulus-reinforcement learning in the amygdala. As learning progresses, more accurate reinforcement expectancies are fed from the amygdala to the orbitofrontal cortex, where their representation allows successful decision making to occur, initiating approaches to objects associated with reward and avoidance of those associated with punishment. In individuals with high levels of psychopathic traits, deficits in prediction error signaling lead to slower and weaker stimulus-reinforcement learning, which in turn leads to weaker and less accurate reinforcement expectancies being fed forward to the orbitofrontal cortex. Individuals become progressively less accurate in their decisions relative to comparison individuals because they are less able to represent the reward expectancy value associated with the presented stimulus and respond accordingly (13).
Previous work has indicated dysfunction of the orbitofrontal cortex in individuals with psychopathic traits (47, 48). The current study extends this by providing information on the nature of the functional impairment. In line with the model, youths with conduct disorder or oppositional defiant disorder plus psychopathic traits, relative to comparison youths, showed significantly lower orbitofrontal cortex responses during early trial learning and to rewarded responses. The first of these findings is compatible with the suggestion of disrupted prediction error signaling in the orbitofrontal cortex in the youths with psychopathic traits (see reference 28). Prediction errors are maximal after the individual's first exposure to the relationship between the cue and the reinforcement but rapidly lessen as the individual develops an expectation of the reinforcement associated with the cue (29). In this regard it is notable that we have previously documented lower orbitofrontal cortex responses, relative to those in comparison groups, to unexpected failures to receive rewards in children with conduct disorder or oppositional defiant disorder plus psychopathic traits (10). The finding of lower orbitofrontal cortex responses to rewarded responses is consistent with the suggestion that this population is less able to represent reward expectancy values. As such, these data are consistent with results from a previous study examining youths with conduct disorder, undifferentiated by psychopathic traits (49). This study also showed lower responsiveness to reward outcome information within the orbitofrontal cortex in the youths with conduct disorder.
Neurobiological accounts of psychopathic traits (13, 50, 51) have neglected consideration of the caudate (and for that matter, the ventral tegmental area and ventral striatum), despite the critical role of these regions in prediction error signaling and/or reinforcement-based learning (26, 27, 52). Part of this likely reflects the choice of cognitive functions examined in the majority of previous fMRI work with youths or adults with psychopathic traits, i.e., expression processing (8, 9, 53), emotional memory (54), and moral reasoning (55). However, the current study revealed lower responsiveness in the caudate (but not the ventral tegmental area or ventral striatum) to early reinforced outcomes relative to later trials in the youths with psychopathic traits. This is compatible with the suggestion of disrupted prediction error signaling in the caudate in youths with conduct disorder or oppositional defiant disorder plus psychopathic traits. Indeed, it is notable that the only previous study examining operant responding in individuals with psychopathic traits also showed dysfunctional responding to reversal errors in the caudate but not ventral striatum among children with conduct disorder or oppositional defiant disorder plus psychopathic traits (10). This pattern is echoed by recent structural MRI work also indicating selective structural abnormalities within the dorsal striatum in adults with psychopathic traits (56). A recent study of healthy adults focused on the nucleus accumbens and found that individuals scoring higher on the impulsive aggressivity components of the Psychopathic Traits Inventory had greater pharmacologically triggered dopamine release and greater activity in response to reward (57). Although intriguing results, these data were somewhat inconsistent with those from the only previous study of which we are aware that showed ventral striatal abnormalities in adults meeting criteria for psychopathy (54). This latter study showed lower ventral striatum activity in response to emotional stimuli in the adults with psychopathy—albeit in response to a very different task. The current study also did not identify any regions demonstrating greater activity during rewarding trials in the youths with psychopathic traits. These differences may reflect the hypothesized distinction between individuals showing heightened aggressive impulsivity in the absence of the core callous traits of psychopathy (who are believed to demonstrate heightened limbic responsiveness [14]) and those who do show these core callous traits (who show low limbic responsiveness).
The dorsal anterior cingulate cortex has been implicated in conflict monitoring (58) and the use of error signals and the integration of reinforcement history to select between competing responses (59, 60). The current study was not designed to distinguish between these models. However, it is important to note that the significant main effect of response type, i.e., commission error versus correct hit, identified in this region (see table in online data supplement) was not modulated by a main effect of group or a group-by-response type interaction. These data suggest that the responses of the dorsal anterior cingulate cortex to the conflict initiated by punishment/error feedback remain intact in youths with conduct disorder or oppositional defiant disorder plus psychopathic traits. Notably, this replicates prior results in similar subjects during a reversal learning paradigm, where both groups showed appropriate recruitment of the dorsal anterior cingulate cortex in response to punished reversal errors (10). In contrast, functional (10) and now structural (56) abnormalities have been reported in these populations in the dorsal striatum (caudate), indicating that abnormalities in reward processing may arise from deficits in the amygdala-insula-orbitofrontal-caudate circuit.
The main effect of diagnosis revealed reduced activation in several brain regions in the youths with psychopathic traits. This could indicate less engagement with the task. In contrast, the regions showing a main effect of response type and phase (i.e., regions where both groups showed appropriate responses as a function of task measures) include the dorsal anterior cingulate cortex and inferior frontal cortex/anterior insula. It is important to note that these data suggest that an engagement explanation appears unsatisfactory, as there is no reason why less task engagement would lead to appropriate recruitment of systems necessary for response change but selectively less recruitment of regions implicated in decision making based on stimulus reinforcement.
One caveat of the present study is that although there were high rates of comorbidity of attention deficit hyperactivity disorder (ADHD) with conduct disorder and oppositional defiant disorder, we did not include a second ADHD comparison group in the current study because neither of our previous studies indicated that youths with ADHD have pathophysiology in the amygdala or orbitofrontal cortex, although this was seen in children with conduct disorder or oppositional defiant disorder plus psychopathic traits (8, 10). Rubia and colleagues have shown dysfunction in orbitofrontal cortex reward signaling in youths with conduct disorder who do not have ADHD but not in youths with ADHD (49). Second, the youths with conduct disorder or oppositional defiant disorder plus psychopathic traits made significantly more commission errors during the late learning phase, which could produce stronger parameter estimates for late commission errors for this group. However, it should be noted that the groups differed not in BOLD responses to late commission errors but, rather, in responses during early trials and in responses to rewarded correct hits.
In short, the current results are highly compatible with developmental models of conduct disorder with psychopathic traits that stress that this disorder reflects a fundamental disruption in the neural systems necessary for appropriate decision making in regard to stimulus reinforcement (14). Problems in this basic form of emotional learning will create difficulties for the child in socializing; the child will be less likely to “learn from his or her mistakes.” Moreover, children will learn from emotional feedback more slowly—this is notable in the present study both in the behavioral data and in the lower sensitivity within both the orbitofrontal cortex and the caudate to early reinforcement information. Appropriate representation of such information is critical for rapid, early emotional learning. In addition, the dysfunction in the signaling of reinforcement outcomes in the orbitofrontal cortex, documented in this study, will be associated with poor decision making. This will lead to the selection of nonoptimal behavioral choices (actions that harm others and actions that are likely to result in individuals being frustrated and potentially reactively aggressive because they do not meet their goals).
These data have clear treatment implications. Specifically, they suggest that the development of pharmacologic or behavioral therapeutic approaches that augment the capacity to make decisions based on stimulus reinforcement may enable youths with high levels of psychopathic traits to overcome their functional deficiencies. In this regard, it is notable that both serotonergic (61) and dopaminergic (62) manipulations influence the performance of the task described in this study as well as its neural substrates. Moreover, a recent report indicated that prediction error signaling in the amygdala facilitates learning by increasing orienting and attention to the stimulus during the subsequent trial (63), and an interesting behavioral approach might be to train youths to direct their attention to explicitly form predictions about the expected reward from a particular action and to explicitly attend to the difference between their verbalized prediction and the actual outcome for both advantageous and disadvantageous actions.
In summary, the current data support previous suggestions of dysfunction in the amygdala and orbitofrontal cortex in youths with conduct disorder or oppositional defiant disorder plus psychopathic traits. More important, they indicate that such individuals are marked by a compromised sensitivity to early reinforcement information in both the orbitofrontal cortex and caudate and to reward outcome information within the orbitofrontal cortex. In conjunction with established models of stimulus-reinforcement instrumental learning, they suggest that the integrated functioning of the amygdala, caudate, and orbitofrontal cortex may be disrupted in individuals with conduct disorder or oppositional defiant disorder plus psychopathic traits.
1. : Aggression and disruptive behavior disorders in children and adolescents. Expert Rev Neurother 2004; 4:623–632Crossref, Medline, Google Scholar
2. : The importance of callous-unemotional traits for extending the concept of psychopathy to children. J Abnorm Psychol 2000; 109:335–340Crossref, Medline, Google Scholar
3. : Callous-unemotional traits and conduct problems in the prediction of conduct problem severity, aggression, and self-report delinquency. J Abnorm Child Psychol 2003; 31:457–470Crossref, Medline, Google Scholar
4. : Disentangling the underlying dimensions of psychopathy and conduct problems in childhood: a community study. J Consult Clin Psychol 2005; 73:400–410Crossref, Medline, Google Scholar
5. : The Psychopathy Checklist: Youth Version. Toronto, Multi-Health Systems, 2003 Google Scholar
6. : The role of callous and unemotional traits in the diagnosis of conduct disor-der. J Child Psychol Psychiatry 2010; 51:688–695Crossref, Medline, Google Scholar
7. : Longitudinal evidence that psychopathy scores in early adolescence predict adult psychopathy. J Abnorm Psychol 2007; 116:155–165Crossref, Medline, Google Scholar
8. : Reduced amygdala re-sponse to fearful expressions in children and adolescents with callous-unemotional traits and disruptive behavior disorders. Am J Psychiatry 2008; 165:712–720Link, Google Scholar
9. : Amygdala hypoactivity to fearful faces in boys with conduct problems and callous-unemotional traits. Am J Psychiatry 2009; 166:95–102Link, Google Scholar
10. : Abnormal ventromedial prefrontal cortex function in children with psychopathic traits during reversal learning. Arch Gen Psychiatry 2008; 65:586–594Crossref, Medline, Google Scholar
11. : A study of anxiety in the sociopathic personality. J Abnorm Soc Psychol 1957; 55:6–10Crossref, Google Scholar
12. : Psychopathy: Theory and Research. New York, John Wiley & Sons, 1970 Google Scholar
13. : The amygdala and ventromedial prefrontal cortex in morality and psychopathy. Trends Cogn Sci 2007; 11:387–392Crossref, Medline, Google Scholar
14. : Dysfunctions of medial and lateral orbitofrontal cortex in psychopathy. Ann NY Acad Sci 2007; 1121:461–479Crossref, Medline, Google Scholar
15. : Passive avoidance learning in psychopathic and nonpsychopathic offenders. J Abnorm Psychol 1986; 95:252–256Crossref, Medline, Google Scholar
16. : Passive avoidance in syndromes of disinhibition: psychopathy and extraversion. J Pers Soc Psychol 1985; 48:1316–1327Crossref, Medline, Google Scholar
17. : Neural topography and chronology of memory consolidation: a review of functional inactivation findings. Neurobiol Learn Mem 1999; 71:1–18Crossref, Medline, Google Scholar
18. : Role of ventral hippocampus in acquisition, consolidation and retrieval of rat's passive avoidance response memory trace. Brain Res 1997; 768:242–248Crossref, Medline, Google Scholar
19. : Orbitofrontal cortex, associative learning, and expectancies. Neuron 2005; 47:633–636Crossref, Medline, Google Scholar
20. : Changes in functional connectivity in orbitofrontal cortex and basolateral amygdala during learning and reversal training. J Neurosci 2000; 20:5179–5189Crossref, Medline, Google Scholar
21. : Orbitofrontal cortex and representation of incentive value in associative learning. J Neurosci 1999; 19:6610–6614Crossref, Medline, Google Scholar
22. : The role of the amygdala and rostral anterior cingulate in encoding expected outcomes during learning. Neuroimage 2006; 29:1161–1172Crossref, Medline, Google Scholar
23. : Ventral striatal neurons encode the value of the chosen action in rats deciding between differently delayed or sized rewards. J Neurosci 2009; 29:13365–13376Crossref, Medline, Google Scholar
24. : Choosing the lesser of two evils, the bet-ter of two goods: specifying the roles of ventromedial prefrontal cortex and dorsal anterior cingulate cortex in object choice. J Neurosci 2006; 26:11379–11386Crossref, Medline, Google Scholar
25. : Is avoiding an aversive outcome rewarding? neural substrates of avoidance learning in the human brain. PLoS Biol 2006; 7 4(8):e233Crossref, Medline, Google Scholar
26. : Predictive neural coding of reward preference involves dissociable responses in human ventral midbrain and ventral striatum. Neuron 2006; 49:157–166Crossref, Medline, Google Scholar
27. : Different neural correlates of reward expectation and reward expectation error in the putamen and caudate nucleus during stimulus-action-reward association learning. J Neurophysiol 2006; 95:948–959Crossref, Medline, Google Scholar
28. : Temporal difference models and reward-related learning in the human brain. Neuron 2003; 38:329–337Crossref, Medline, Google Scholar
29. : A theory of Pavlovian conditioning: variations in the effectiveness of reinforcement and nonreinforcement, in Classical Conditioning II. Edited by Black AHProkasy WF. New York, Appleton-Century-Crofts, 1972, pp 64–99 Google Scholar
30. : Impaired reversal but intact acquisition: probabilistic response reversal deficits in adult individuals with psycho-pathy. J Abnorm Psychol 2006; 115:552–558Crossref, Medline, Google Scholar
31. : Explicit neural signals reflecting reward uncertainty. Philos Trans R Soc Lond B Biol Sci 2008; 363:3801–3811Crossref, Medline, Google Scholar
32. : The Antisocial Process Screening Device. Toronto, Multi-Health Systems, 2001 Google Scholar
33. : Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 1997; 36:980–988Crossref, Medline, Google Scholar
34. : Assessment of “juvenile psychopathy” and its association with violence: a critical review. Behav Sci Law 2001; 19:53–80Crossref, Medline, Google Scholar
35. : Psychopathy screening of incarcerated juveniles: a comparison of measures. Psychol Assess 2002; 14:390–396Crossref, Medline, Google Scholar
36. : Response reversal and children with psychopathic tendencies: success is a function of salience of contingency change. J Child Psychol Psychiatry 2005; 46:972–981Crossref, Medline, Google Scholar
37. : Deficient behavioral inhibition and anomalous selective attention in a community sample of adolescents with psychopathic traits and low-anxiety traits. J Abnorm Child Psychol 2005; 33:461–470Crossref, Medline, Google Scholar
38. : Dissociable roles of medial orbital frontal cortex in human operant extinction learning. Neuroi-mage 2008; 43:748–755Crossref, Medline, Google Scholar
39. : A standardized set of 260 pictures: norms for name agreement, image agreement, familiarity, and visual com-plexity. J Exp Psychol Hum Learn 1980; 6:174–215Crossref, Medline, Google Scholar
40. : AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res 1996; 29:162–173Crossref, Medline, Google Scholar
41. : Comparison of functional activation foci in children and adults using a common stereotactic space. Neuroimage 2003; 19:16–28Crossref, Medline, Google Scholar
42. : The feasibility of a common stereotactic space for children and adults in fMRI studies of development. Neuroimage 2002; 17:184–200Crossref, Medline, Google Scholar
43. : Co-Planar Stereotaxic Atlas of the Human Brain. New York, Thieme Medical, 1988 Google Scholar
44. : Passive avoidance learning in individuals with psychopathy: modulation by reward but not by punishment. Pers Individ Dif 2004; 37:1179–1192Crossref, Google Scholar
45. : Neural encoding in orbitofrontal cortex and basolateral amygdala during olfactory discrimination learning. J Neurosci 1999; 19:1876–1884Crossref, Medline, Google Scholar
46. : Encoding predicted outcome and acquired value in orbitofrontal cortex during cue sam-pling depends upon input from basolateral amygdala. Neuron 2003; 39:855–867Crossref, Medline, Google Scholar
47. : Deficient fear conditioning in psychopathy: a functional magnetic reso-nance imaging study. Arch Gen Psychiatry 2005; 62:799–805Crossref, Medline, Google Scholar
48. : Neural correlates of social cooperation and non-cooperation as a function of psychopathy. Biol Psychiatry 2007; 61:1260–1271Crossref, Medline, Google Scholar
49. : Disorder-specific dissociation of orbitofrontal dysfunction in boys with pure conduct disorder during reward and ventrolateral prefrontal dysfunction in boys with pure ADHD during sustained attention. Am J Psychiatry 2009; 166:83–94Link, Google Scholar
50. : Neuro-cognitive models of aggression, the antisocial personality disorders and psychopathy. J Neurol Neurosurg Psychiatry 2001; 71:727–731Crossref, Medline, Google Scholar
51. : A cognitive neuroscience perspective on psychopathy: evidence for paralimbic system dysfunction. Psychiatry Res 2006; 142:107–128Crossref, Medline, Google Scholar
52. : Dissociable roles of ventral and dorsal striatum in instrumental condition-ing. Science 2004; 304:452–454Crossref, Medline, Google Scholar
53. : Psychopathy and functional magnetic resonance imaging blood oxygenation level-dependent responses to emotional faces in violent patients with schizophrenia. Biol Psychiatry 2009; 66:570–577Crossref, Medline, Google Scholar
54. : Limbic abnormalities in affective processing by criminal psycho-paths as revealed by functional magnetic resonance imaging. Biol Psychiatry 2001; 50:677–684Crossref, Medline, Google Scholar
55. : The neural correlates of moral decision-making in psychopathy. Mol Psychiatry 2008; 14:5–6Crossref, Google Scholar
56. : Increased volume of the striatum in psychopathic individuals. Biol Psychiatry 2010; 67:52–58Crossref, Medline, Google Scholar
57. : Mesolimbic dopamine reward system hypersensitivity in individuals with psychopathic traits. Nat Neurosci 2010; 13:419–421Crossref, Medline, Google Scholar
58. : Conflict monitoring and anterior cingulate cortex: an update. Trends Cogn Sci 2004; 8:539–546Crossref, Medline, Google Scholar
59. : Dorsal anterior cingulate cortex integrates reinforcement history to guide voluntary behavior. Cortex 2008; 44:548–559Crossref, Medline, Google Scholar
60. : Contrasting roles for cingulate and orbitofrontal cortex in decisions and social behav-iour. Trends Cogn Sci 2007; 11:168–176Crossref, Medline, Google Scholar
61. : The impact of tryptophan depletion and 5-HTTLPR genotype on passive avoidance and response reversal instrumental learning tasks. Neuropsycho-pharmacology 2007; 32:206–215Crossref, Medline, Google Scholar
62. : Impairments of probabilistic response reversal and passive avoidance following catecholamine depletion. Neuropsychopharmacology 2009; 34:2691–2698Crossref, Medline, Google Scholar
63. : Neural correlates of variations in event processing during learning in basolateral amygdala. J Neurosci 2010; 30:2464–2471Crossref, Medline, Google Scholar

