
Gender, Poverty, and Postnatal Depression: A Study of Mothers in Goa, India
Abstract
OBJECTIVE: This study described the natural history of depression in mothers who recently gave birth in a low-income country and to investigate the effect of risk factors, particularly related to infant gender bias, on the occurrence and outcome of depression. METHOD: The authors studied a group of pregnant mothers recruited during their third trimester of pregnancy from a district hospital in Goa, India. The mothers were interviewed at recruitment, 6–8 weeks, and 6 months after childbirth. Interview data included presence of antenatal and postnatal depression, obstetric history, economic and demographic characteristics, and gender-based variables (preference for male infant, presence of marital violence). RESULTS: Depressive disorder was detected in 59 (23%) of the mothers at 6–8 weeks after childbirth; 78% of these patients had had clinically substantial psychological morbidity during the antenatal period. More than one-half of the patients remained ill at 6 months after delivery. Economic deprivation and poor marital relationships were important risk factors for the occurrence and chronicity of depression. The gender of the infant was a determinant of postnatal depression; it modified the effect of other risk factors, such as marital violence and hunger. Depressed mothers were more disabled and were more likely to use health services than nondepressed mothers. CONCLUSIONS: Maternal and infant health policies, a priority in low-income countries, must integrate maternal depression as a disorder of public health significance. Interventions should target mothers in the antenatal period and incorporate a strong gender-based component.
Postnatal depression generally occurs within 6–8 weeks after childbirth. One meta-analysis (1) has shown an average prevalence of postpartum depression of 13% (95% confidence interval [CI]=12.3–13.4) in the general population. In developed countries, the risk factors for postnatal depression are past history of psychological disorder, psychological disorder during pregnancy, low socioeconomic status, complicated delivery, and poor marital relationship (1). Women in many countries whose populations have low incomes face considerable inequalities, ranging from fewer opportunities in education and employment to less control over personal decisions, such as the use of contraception to plan pregnancies. In India, the cultural view that male children are preferred over female children is an important reason that the sex ratio is unbalanced in favor of men (2).
There are few studies regarding the influence of gender-based factors on the risk for and outcome of postnatal depression. The objective of this study was to describe the natural history of postnatal depression in a developing country in which gender inequality is deeply entrenched. This study aimed to examine the etiological role of risk factors recognized to be relevant to the onset of postpartum depression in developed societies, as well as those that reflect the poverty and gender inequality faced by women in India.
Method
The study group consisted of women from Goa, India, in their last trimester of pregnancy who were followed up at 6–8 weeks and 6 months postpartum. Goa is one of India’s smallest states and has a population of 1.4 million. In the 1992–1993 Family Health Survey (3), Goa recorded an infant mortality rate of 20 per 1,000 live births, a literacy rate of 67% among women, and a rate of 87% for supervised births. Asilo Hospital is the main district hospital in the town of Mapusa, which is in North Goa. All of the mothers were patients at the antenatal clinic at Asilo Hospital and were more than 30 weeks pregnant.
A total of 270 mothers were recruited consecutively. Mothers who were transient visitors or did not speak any of the study languages (Konkani, Marathi, Hindi, or English) were excluded. After complete description of the study to the subjects, written consent was obtained in the presence of a hospital nurse.
All women were interviewed at recruitment with the General Health Questionnaire, a 12-item measure of overall general psychological health (4). The Konkani version of the questionnaire has been validated for use in Goa (5). A semistructured interview was used to elicit data regarding demographic characteristics (age, religion, education, employment, and economic data regarding such topics as experience of hunger and level of debt). Data regarding availability of social support, quality of marital relationship, marital violence (lifetime and during pregnancy), and relationships with in-laws were collected. Also recorded were obstetric histories, including numbers of living children and information about previous abortions and miscarriages. Details of the current pregnancy (whether it was planned or not and if a particular gender of infant was favored) were also gathered.
At 6–8 weeks after birth, the mothers were administered the Edinburgh Postnatal Depression Scale, a widely used screening questionnaire for the detection of postnatal depression (6). Scores on this measure range from 0 to 30. Versions of the scale in the Konkani language were developed by use of the translation–back-translation method from English and Hindi versions developed earlier (7). The validity of the Konkani version of the Edinburgh Postnatal Depression Scale was evaluated in a two-stage pilot study that compared patients diagnosed with depression on this scale with patients diagnosed with major depressive disorder on the basis of the Revised Clinical Interview Schedule (5, 8), a standardized psychiatric interview for the measurement and diagnosis of common mental disorders in nonpsychiatric settings. A cutoff score of 11 or 12 on the Edinburgh Postnatal Depression Scale was found to detect depression with a specificity of 85% and sensitivity of 92%. Similar validity coefficients have been reported with the use of the Edinburgh Postnatal Depression Scale in other Asian cultures (9).
Obstetric histories included information about the current pregnancy, including type of delivery, prematurity of infant, infant gender, infant illness, infant hospital admission, and infant death. Questions about infant behavior included data regarding infant crying, sleeping, feeding, and need to be carried. Data were also obtained about maternal support from the patient’s husband, mother, and mother-in-law.
At the 6-month follow-up, the mothers were administered the Edinburgh Postnatal Depression Scale and the Brief Disability Questionnaire, which provides an objective measure of disability in the form of a continuous score and two independent measures for number of days sick or spent in bed related to illness (10). A Konkani version of the scale has been used in previous studies (11). Also assessed was use of health services during the previous 3 months, including consultations with doctors, hospital admissions, results of diagnostic tests, and medication use.
Analyses were aimed at answering each of the research objectives. The occurrence of postnatal depression was estimated by using scores on the Edinburgh Postnatal Depression Scale at 6–8 weeks after delivery; women who scored 12 or more were considered to have postnatal depression. The incidence of depression in the postnatal period was determined from the proportion of mothers who developed a de novo depressive disorder after childbirth. Univariate associations (relative risk, Wald’s chi-square) between antenatal and postnatal variables and postnatal depression were considered to be predictors of postnatal depression. Variables that were significantly (p≤0.01) associated with postnatal depression were entered into multivariate logistic regression models for two types of variables, antenatal and postnatal.
The outcome for mothers with postnatal depression was determined from univariate comparisons of antenatal and early postnatal variables with the persistence of postnatal depression at 6 months for the mothers who were depressed at 6–8 weeks. Data regarding the association of persistent morbidity (in mothers who were depressed both at 6–8 weeks and 6 months) with disability and health care usage were collected at 6 months after birth.
Results
A total of 297 mothers were eligible to participate in the study. Of these, 27 mothers (9%) refused to participate. Thus, 270 mothers who were at an average gestational age of 34 weeks were recruited. The average age of the women was 26 years (SD=4, range=18–40). Most (78%) of the mothers were literate, married (99%), and Hindu (89%). Fewer than half (42%) were primigravid. Most (66%) lived in extended families. Only 8.5% of the women worked outside the home. Most (98%) of the fathers worked outside the home, but the most common types of jobs involved manual labor and semiskilled occupations such as farming. The average monthly income of the fathers was 2,140 rupees (U.S. equivalent=$47).
A total of 252 of the mothers (93%) were reexamined at 6–8 weeks (mean=7.4, SD=1.9) after childbirth. Of these mothers, 59 (23%) were considered to have postnatal depression. Of the mothers who did not have antenatal depression (N=146), 12 (8%) developed depression in the postnatal period. Thus, of the 59 mothers with postnatal depression, only 13 (22%) had depression that arose in the puerperium. A total of 235 (87%) of the 270 mothers were examined at 6 months postpartum; of these, 51 (22%) of the mothers were depressed. Of these mothers, 34 (67%) were considered to be chronically depressed (depressed at 6–8 weeks and at 6 months postpartum). Thus 14% (34 of 235) of the mothers had chronic depression in the postpartum period.
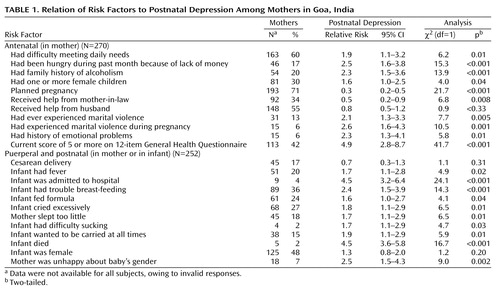
Of the sociodemographic characteristics examined, maternal employment was found to be a predictor of postnatal depression (relative risk=1.9; χ2=4.1, df=1, p=0.04), while number of years of maternal education (relative risk=0.5; χ2=4.4, df=12, p=0.03) and paternal employment (relative risk=0.3; χ2=9.1, df=1, p=0.002) were found to be protective factors against depression in the postpartum. Table 1 shows the univariate association of risk factors at recruitment and 6–8 weeks after delivery with postnatal depression in the mothers. After adjustment for all significantly associated antenatal risk factors, the positive association of antenatal psychiatric morbidity (odds ratio=6.02; χ2=20.9, df=1, p<0.001) and the negative association of planned pregnancy (odds ratio=0.3; χ2=6.9, df=1, p=0.007) remained significantly related to risk for postnatal depression. After adjustment for all significant postnatal variables, the positive associations of problems with breast-feeding the infant (odds ratio=3.1, χ2=3.1, df=1, p=0.001), infant hospital admission (odds ratio=36.3; χ2=9.3, df=1, p=0.002), and sadness about the infant’s gender (odds ratio=3.3; χ2=6.4, df=1, p=0.01) remained significant risk factors for depression. A cutoff score of four out of five items on the General Health Questionnaire had a sensitivity of 78% and specificity of 69% in predicting postnatal depression (receiver operating characteristic: area under the curve=0.79).
There was significant modification of the influence of various risk factors for postnatal depression on the basis of the gender of the infant; for example, the risk of postnatal depression in the mothers who had experienced marital violence was significantly greater if the infant was a girl, but it was significantly lower if the infant was a boy (Table 2).
Univariate analyses were performed on data for all variables gathered at recruitment and at the 6–8-week follow-up to determine risk factors for chronicity in the group of mothers who were depressed at 6–8 weeks and reexamined at 6 months postpartum (N=58). A score of more than 4 on certain items on the General Health Questionnaire (antenatal psychiatric morbidity: relative risk=2.1, 95% CI=1.0–5.2; χ2=5.3, df=1, p=0.02; marital violence: relative risk=1.9, 95% CI=1.4–2.7; χ2=1.9, df=1, p=0.002; antenatal hunger: relative risk=1.9, 95% CI=1.3–2.8; χ2=8.7, df=1, p=0.003; and having a living female child: relative risk=1.8, 95% CI=1.2–2.7; χ2=7.1, df=1, p<0.001) were found to be predictors of chronic morbidity. Violence in the postpartum period was reported by six mothers, all of whom had chronic postpartum depression. The effect of the gender of the infant on these associations was evident. For example, the high risk of persistent depression in mothers who had experienced marital violence was greater if the new infant was a girl (relative risk=1.9, 95% CI=1.2–2.8), but it was lower if the new infant was a boy (relative risk=1.7, 95% CI=0.8–3.5; χ2=1.4, df=1, p=0.26).
The mothers who were considered chronically depressed (N=34) were more likely to have consulted their primary care doctor (odds ratio=4.1, 95% CI=1.6–10.2; χ2=8.1, df=1, p=0.003) or the general outpatient clinic at the hospital (odds ratio=5.5, 95% CI=1.6–19.2; χ2=6.4, df=1, p=0.01) than the other mothers. Two mothers were admitted to the hospital in the period since the 6–8-week follow-up, but neither had postpartum depression. Scores on the Brief Disability Questionnaire were significantly higher in the chronically depressed mothers (mean=8.8, 95% CI=6.5–11.2) than in the other mothers (mean=3.3, 95% CI=2.7–3.9) (t=–6.3, df=230, p<0.001). The depressed mothers spent about twice the number of days in the previous 30 days unable to complete their daily activities (mean=3.2, 95% CI=0.9–5.5) than the other mothers (mean=1.7, 95% CI=1.0–2.4) (t=–1.5, df=230, p=0.12).
Discussion
To our knowledge, this article describes the first prospective study of postnatal depression in South Asia. Its objectives were to describe the natural history of depression after childbirth and to investigate the role of gender-based factors on the risk and outcome of depression. Given that the majority of low-income mothers in the study area delivered their babies in a public hospital and that the rate of refusal was low and the rates of follow-up were high, we are confident that the study findings are representative of the low-income population of Goa, India. All of the measures had been validated for use in the Konkani language with women in Goa. The key findings of the study are that postnatal depression is a common mental illness in this area; it is usually a consequence of preexisting antenatal morbidity; it is a chronic disorder for one-half of the women who suffer from the illness; and it is associated with greater maternal disability and use of health services. A total of 78% (N=46) of the women with postnatal depression had clinically substantial psychological morbidity during the antenatal period. This study replicated the role of established risk factors, such as poor marital relationship and antenatal psychiatric morbidity. The findings also demonstrate that in the cultural setting of the study, there was a significant risk associated with gender-based factors, mediated by the preference for male children and the existence of marital violence. The association of depression with poverty-related variables, such as hunger and low level of education, as reported from other studies in developing countries (12), were replicated.
There are few epidemiological investigations of maternal depression in developing countries. A recent well-designed study of an urban township in South Africa (13) reported a similarly high rate of postpartum depression (34.7%). The rates of postnatal depression that we found in our study are no higher than those reported in relatively recent population and primary care studies in low-income countries (14–16), including Goa itself (11). The finding that the majority of mothers had an onset of antenatal depression is also consistent with evidence from other prospective studies (17, 18). Thus, “postnatal depression” simply describes the presence of a depressive disorder in the period after childbirth. It does not, however, indicate any specific risk or etiological role of childbirth in the onset of the depressive disorder.
The study confirms our hypothesis that gender-based factors are important determinants of postnatal depression. Violence against women, a major public health concern in a country in which more than one-third of women report being beaten by their husbands (19), was found to be common and, not surprisingly, a significant risk factor for postnatal depression. The preference for male children is deeply rooted in Indian society; such gender bias and the limited control a woman has over her reproductive health may make pregnancy a stressful experience for some women. Thus, women who already have a female child face greater stress because of their wish that their new infant be a boy. In the event that the child is a girl, the risk of depression is greater. Mothers may be blamed for the birth of a female child. Analyses show that there is a strong interaction among many risk factors, such as economic deprivation, marital violence, and the infant’s gender. Although the precise mechanism of how these stressors operate differentially according to the gender of the infant remains unclear, it is plausible that the family’s collective joy at the arrival of a male infant helps support the mother and negates the risk associated with other stressors.
The implications of the findings of this study for policy and practice is that mental health must be integrated into maternal health care in low-income countries. Given the shortage of mental health manpower, the role of care will need to be met by midwives, gynecologists, and pediatricians. Parent counseling to promote marital communication and to reduce the preference for male children must be an essential component of routine antenatal care. Future research should focus on studies examining the efficacy of interventions delivered in the antenatal period on the prevention of postnatal depression. Improving marital communication and reducing gender preference should be important components of any such interventions.
 |
 |
Received July 28, 2000; revisions received Dec. 4, 2000, and April 26, 2001; accepted June 13, 2001. From the Sangath Centre for Child Development & Family Guidance; and the London School of Hygiene & Tropical Medicine, London. Address reprint requests to Dr. Patel, Sangath Centre, 841/1 Alto Porvorim, Goa 403521, India; [email protected] (e-mail). Funded by a MacArthur Foundation Fellowship for Population Innovations. The authors thank the Directorate of Health Services (government of Goa) for allowing research at Asilo Hospital, the doctors and patients of Asilo Hospital for their help, and Lucy Martins and Wilma D’Silva for data collection.
1. O’Hara MW, Swain AM: Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatry 1996; 8:37-54Crossref, Google Scholar
2. Cohen A: Excess female mortality in India: the case of Himachal Pradesh. Am J Public Health 2000; 90:1369-1371Crossref, Medline, Google Scholar
3. National Family Health Survey (MCH and Family Planning), 1992-1993. Goa, India, Population Research Centre, JSS Institute of Economic Research, International Institute for Population Sciences, 1995Google Scholar
4. Goldberg DP, Williams P: The User’s Guide to the General Health Questionnaire. Slough, UK, National Foundation for Educational Research-Nelson, 1988Google Scholar
5. Patel V, Pereira J, Mann A: Somatic and psychological models of common mental disorders in India. Psychol Med 1998; 28:135-143Crossref, Medline, Google Scholar
6. Cox JL: Detection of postnatal depression: development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 1987; 150:782-786Crossref, Medline, Google Scholar
7. Cox J, Holden J (eds): Perinatal Psychiatry: Use and Misuse of the Edinburgh Postnatal Depression Scale. London, Gaskell (Royal College of Psychiatrists), 1994Google Scholar
8. Lewis G, Pelosi A, Araya R, Dunn G: Measuring psychiatric disorder in the community: a standardized assessment for use by lay interviewers. Psychol Med 1992; 22:465-486Crossref, Medline, Google Scholar
9. Ghubash R, Abou-Saleh MT, Daradkeh TK: The validity of the Arabic Edinburgh Postnatal Depression Scale. Soc Psychiatry Psychiatr Epidemiol 1997; 32:474-476Medline, Google Scholar
10. VonKorff M, Ustun TB, Ormel J, Kaplan I, Simon G: Self-report disability in an international primary care study of psychological illness. J Clin Epidemiol 1996; 49:297-303Crossref, Medline, Google Scholar
11. Patel V, Pereira J, Coutinho L, Fernandes R, Fernandes J, Mann A: Poverty, psychological disorder and disability in primary care attenders in Goa, India. Br J Psychiatry 1998; 171:533-536Crossref, Google Scholar
12. Patel V, Araya R, Lima MS, Ludermir A, Todd C: Women, poverty and common mental disorders in four restructuring societies. Soc Sci Med 1999; 49:1461-1471Crossref, Medline, Google Scholar
13. Cooper P, Tomlinson M, Swartz L, Woolgar M, Murray L, Molteno C: Post-partum depression and the mother-infant relationship in a South African peri-urban settlement. Br J Psychiatry 1999; 175:554-558Crossref, Medline, Google Scholar
14. Patel V, Abas M, Broadhead J, Todd C, Reeler AP: Depression in developing countries: lessons from Zimbabwe. Br Med J 2001; 322:482-484Crossref, Medline, Google Scholar
15. Mumford DB, Saeed K, Ahmad I, Latif S, Mubbashar M: Stress and psychiatric disorder in rural Punjab: a community survey. Br J Psychiatry 1997; 170:473-478Crossref, Medline, Google Scholar
16. Reichenheim ME, Harpham T: Maternal mental health in a squatter settlement in Rio de Janeiro. Br J Psychiatry 1991; 159:683-690Crossref, Medline, Google Scholar
17. Nhiwatiwa S, Patel V, Acuda SW: Predicting postnatal mental disorder with a screening questionnaire: a prospective cohort study from a developing country. J Epidemiol Community Health 1998; 52:262-266Crossref, Medline, Google Scholar
18. Najman JM, Andersen MJ, Bor W, O’Callaghan MJ, Williams GM: Postnatal depression—myth or reality?: maternal depression before and after the birth of a child. Soc Psychiatry Psychiatr Epidemiol 2000; 35:19-27Crossref, Medline, Google Scholar
19. Jejeebhoy S: Wife-beating in rural India: a husband’s right? evidence from survey data. Economic and Political Weekly, April 11, 1998, pp 855-862Google Scholar

