
Association of Initial Antipsychotic Response to Clozapine and Long-Term Weight Gain
Abstract
Objective: The aim of this study was to test whether the initial antipsychotic response to clozapine is related to subsequent weight change. Method: This study was an 8-year retrospective chart review of 96 hospitalized patients with schizophrenia. Data on monthly weight change, initial clinical response, age, gender, clozapine dose, and concomitant use of mood stabilizers and other antipsychotics were analyzed. Results: Fifty-five (57.3%) of the patients received clozapine over the entire 8-year period; these subjects experienced an average weight gain of 11.7 kg (SD=1.6). Seventeen of these patients (30.9%) who had a significant initial clinical response (CGI improvement rating of 1 or 2 during the first 14 months) gained significantly more weight (13.8 kg [SD=8.4]) than did the 38 patients without a significant initial response (4.5 kg [SD=12.0]). Multiple linear regression analysis showed significant initial clinical response and lower baseline body mass index were associated with significantly more weight gain. Conclusions: The results show that initial antipsychotic response to clozapine is associated with subsequent long-term weight gain as measured over 8 years.
Clozapine is the most effective agent for treatment-resistant patients with schizophrenia (1) . However, treatment with clozapine has been associated with a number of metabolic disturbances. A 5-year naturalistic study with 82 patients confirmed that clozapine causes weight gain, a weight gain that continued approximately 46 months after initiation of treatment (2) . A relationship between weight gain and improvement in psychosis during treatment with clozapine was first suggested by Leadbetter et al. (3) , who reported that improvements in Brief Psychiatric Rating Scale (BPRS) total score was significantly greater for eight patients with marked weight gain than for 13 other patients with less weight gain. Subsequently, Lamberti et al. (4) reported a nearly significant correlation between decrease in BPRS total score and weight gain in 36 schizophrenia patients treated with clozapine for 6 months. Similar findings were reported by Czobor et al. (5) for 38 patients receiving clozapine for 14 weeks. Meltzer et al. (6) also found that increase in weight predicted improvement in psychosis after 6 weeks and after 6 months of clozapine treatment in 74 patients. On the other hand, no association between clinical response and weight gain with clozapine were reported by Umbricht et al. for 64, 45, and 19 schizophrenia patients treated for 4, 8, and 12 weeks, respectively (7) , by Bustillo et al. (8) for 19 patients treated with clozapine for 1 year, or by Hummer et al. in 31 patients treated for 12 weeks (9) . Meltzer et al. concluded that the relationship between weight gain and response was modest early in treatment but became significant in most long-term studies. Possible reasons for these inconsistent results may include failure to adjust for initial body weight and variability in outcome measures, reliability of assessment, concomitant medications, and clozapine dosage (10) .
Patients receiving clozapine frequently continue with this medication for years (11) . Previously, our team reported a significant correlation between weight gain and change in Clinical Global Impression (CGI) ratings in female but not male patients treated with clozapine for 14 months (12) . The aim of this study was to determine whether initial antipsychotic response predicts subsequent weight change. Because these inpatients lived in the same hospital over the course of the study, the potentially confounding factors of diet, activity level, and drug compliance were optimally controlled. Furthermore, the patients had no exposure to other atypical antipsychotics because clozapine was the first and only atypical antipsychotic used at that time in the hospital. These conditions provided a favorable setting for investigating long-term weight change with clozapine.
Method
This study was a retrospective chart review of 96 patients hospitalized with schizophrenia (per DSM-IV) at the largest psychiatric teaching hospital that offered long-term care to patients with refractory schizophrenia or patients with poor social support. These patients had undergone at least two typical antipsychotic trials of adequate dose and duration with no response. The patients were consecutively started on clozapine regimens between May 1995 and March 1997. All patients were weighed monthly by nurses, and continuous body weight records for the 8-year period were available for review. The initial clinical response for the first 14 months was rated by the psychiatrist-in-charge (Y.M.B.) using the CGI. Patients who received CGI improvement ratings of 1 (very much improved) or 2 (much improved) were considered to have a significant clinical response. Other patients were considered to have a nonsignificant response. Data on age, gender, clozapine dose, and concomitant use of mood stabilizers and other antipsychotics were obtained through retrospective chart review. To examine the relationship between weight gain and clinical response over the 8-year study period, a repeated measures analysis of covariance with baseline body mass index (BMI) was used. Multiple linear regression analysis was performed to investigate the factors associated with 8-year weight change.
Results
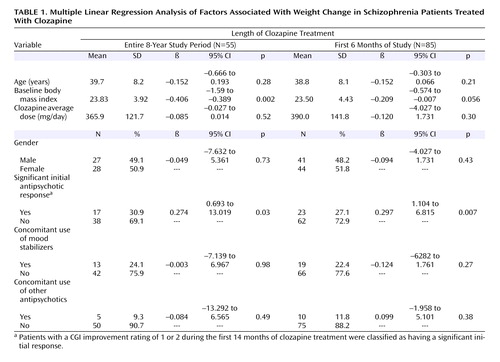
The 96 patients (46 women and 50 men) were 38.3 years old (SD=8) at clozapine initiation and had an average baseline BMI of 23.4 (SD=4.5). Fifty-five (57.3%) patients received clozapine for the entire 8-year study period. Forty-one patients were excluded because of incomplete weight records (N=10), unavailable medical records (N=4), discharge (N=4), death (N=4), or switch to other antipsychotics (N=19). Among the 19 patients switched to other antipsychotics, 17 had no response to clozapine and at the time of discontinuation, the average duration of clozapine treatment was 39.6 months (SD=29.3) and average weight gain was 4.5 kg (SD=15.1). The other two patients had responded, but one discontinued because of hypersalivation at the 48th month without weight change. The reason for the other patient’s discontinuation was unknown because the medical records were unavailable. There were no significant demographic differences or differences in initial 14-month weight change or clinical response between the 55 patients included in the analysis and the 41 who were excluded. For the 55 patients included in the study, the average weight gain was 11.7 kg (SD=1.6) over 8 years. Seventeen of these patients (30.9%) had a significant initial antipsychotic response (average CGI improvement rating: 2.0 [SD=0.6]). This group had an average 8-year weight gain of 13.8 kg (SD=8.4). The other 38 patients did not have a significant clinical response (average CGI improvement rating: 3.7 [SD=0.5]), and their average 8-year weight gain was 4.5 kg (SD=12.0). As seen in Figure 1 , there was a significant difference in BMI change over the 8-year study period between those with and those without a significant initial antipsychotic response. Multiple linear regression showed that two factors, significant initial clinical response and lower baseline BMI, were associated with greater weight gain. When a supplementary regression analysis was performed that expanded the number of subjects to include those participating in the study at the 6-month mark (N=85), the results still showed that clinical response and baseline BMI were the two factors associated with weight gain ( Table 1 ).

a Patients with a CGI improvement rating of 1 or 2 during the first 14 months of clozapine treatment were classified as having a significant initial response. Group difference by repeated measures analysis: F=13.11, df=1, p=0.001.
Discussion
The results show that in this patient group, the initial antipsychotic response to clozapine was associated with subsequent weight gain over an 8-year period. Previous studies have also shown evidence for an association between weight gain and clinical response with other atypical antipsychotic drugs (13) and typical antipsychotics (14 , 15) . These results suggest that the relationship found in our study between weight gain and antipsychotic response may be a more generalized phenomenon. The patients in our study who showed significant initial antipsychotic response gained up to 14 kg (30.8 lb), suggesting a morbidity concern for which a weight control program for these patients may be recommended from the start. Our results are consistent with previous reports that patients with a lower baseline BMI demonstrate greater weight gain associated with clozapine treatment (16) as well as with olanzapine treatment (17 – 19) . Our previous study noted the association between weight gain and clinical response in female but not male patients (11) . However, after baseline BMI was controlled, the gender difference no longer existed at 14 months and at 8 years, which indicated that future weight gain studies should control for baseline BMI.
To the best of our knowledge, this is the first study to report that initial antipsychotic response predicts long-term weight gain. However, the study was retrospective in nature and therefore selection bias may exist. But this concern might be alleviated by the similar characteristics between patients included in the study group and those who were excluded. Another concern is that the initial clinical response was determined only by the CGI. However, the ratings were all performed by one experienced psychiatrist-in-charge, who cared for these patients for years, which avoids the concern about interrater reliability. Moreover, the clinical response rate to clozapine was 30.9%, similar to the 30% that Kane et al. reported (20) . Considering the long-term health risks associated with excess weight gain, for patients with lower baseline BMI and a good initial clinical response, weight change and associated metabolic syndrome symptoms should be closely monitored.
1. Chakos M, Lieberman J, Hoffman E, Bradford D, Sheitman B: Effectiveness of second-generation antipsychotics in patients with treatment-resistant schizophrenia: a review and meta-analysis of randomized trials. Am J Psychiatry 2001; 158:518–526Google Scholar
2. Henderson DC, Cagliero E, Gray C, Nasrallah RA, Hayden DL, Schoenfeld DA, Goff DC: Clozapine, diabetes mellitus, weight gain, and lipid abnormalities: a five-year naturalistic study. Am J Psychiatry 2000; 157:975–981Google Scholar
3. Leadbetter R, Shutty M, Pavalonis D, Vieweg V, Higgins P, Downs M: Clozapine-induced weight gain: prevalence and clinical relevance. Am J Psychiatry 1992; 149:68–72Google Scholar
4. Lamberti JS, Bellnier T, Schwarzkopf SB: Weight gain among schizophrenic patients treated with clozapine. Am J Psychiatry 1992; 149:689–690Google Scholar
5. Czobor P, Volavka J, Sheitman B, Lindenmayer JP, Citrome L, McEvoy J, Cooper TB, Chakos M, Lieberman JA: Antipsychotic-induced weight gain and therapeutic response: a differential association. J Clin Psychopharmacol 2002; 22:244–251Google Scholar
6. Meltzer HY, Perry E, Jayathilake K: Clozapine-induced weight gain predicts improvement in psychopathology. Schizophr Res 2003; 59:19–27Google Scholar
7. Umbricht DS, Pollack S, Kane JM: Clozapine and weight gain. J Clin Psychiatry 1994; 55(suppl B):157–160Google Scholar
8. Bustillo JR, Buchanan RW, Irish D, Breier A: Differential effect of clozapine on weight: a controlled study. Am J Psychiatry 1996; 153:817–819Google Scholar
9. Hummer M, Kemmler G, Kurz M, Kurzthaler I, Oberbauer H, Fleischhacker WW: Weight gain induced by clozapine. Eur Neuropsychopharmacol 1995; 5:437–440Google Scholar
10. Meltzer HY, Perry E, Jayathilake K: Clozapine-induced weight gain predicts improvement in psychopathology. Schizophr Res 2003; 59:19–27Google Scholar
11. Gerlach J, Koppelhus P, Helweg E, Monrad A: Clozapine and haloperidol in a single-blind cross-over trial: therapeutic and biochemical aspects in the treatment of schizophrenia. Acta Psychiatr Scand 1974; 50:410–424Google Scholar
12. Bai YM, Lin CC, Chen JY, Lin CY: Weight gain among patients on clozapine. Psychiatr Serv 1999; 50:704–705Google Scholar
13. Basson BR, Kinon BJ, Taylor CC, Szymanski KA, Gilmore JA, Tollefson GD: Factors influencing acute weight change in patients with schizophrenia treated with olanzapine, haloperidol, or risperidone. J Clin Psychiatry 2001; 62:231–238Google Scholar
14. Singh MM, De Dios LV, Kline NS: Weight as a correlate of clinical response to psychotropic drugs. Psychosomatics 1970; 11:562–570Google Scholar
15. Holden JM, Holden UP: Weight changes with schizophrenic psychosis and psychotropic drug therapy. Psychosomatics 1970; 11:551–561Google Scholar
16. Covell NH, Weissman EM, Essock SM: Weight gain with clozapine compared to first generation antipsychotic medications. Schizophr Bull 2004; 30:229–240Google Scholar
17. Tran PV, Hamilton SH, Kuntz AJ, Potvin JH, Andersen SW, Beasley C Jr, Tollefson GD: Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders. J Clin Psychopharmacol 1997; 17:407–418Google Scholar
18. Purdon SE, Jones BD, Stip E, Labelle A, Addington D, David SR, Breier A, Tollefson GD: Neuropsychological change in early phase schizophrenia during 12 months of treatment with olanzapine, risperidone, or haloperidol. The Canadian Collaborative Group for Research in Schizophrenia. Arch Gen Psychiatry 2000; 57:249–258Google Scholar
19. Gureje O, Miles W, Keks N, Grainger D, Lambert T, McGrath J, Tran P, Catts S, Fraser A, Hustig H, Andersen S, Crawford AM: Olanzapine vs risperidone in the management of schizophrenia: a randomized double-blind trial in Australia and New Zealand. Schizophr Res 2003; 61:303–314Google Scholar
20. Kane J, Honigfeld G, Singer J, Meltzer H: Clozapine for the treatment-resistant schizophrenic: a double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988; 45:789–796Google Scholar

