
Cognitive Substrates of Thought Disorder, II: Specifying a Candidate Cognitive Mechanism
Abstract
Objective:In part I of this series, the authors found that semantic knowledge and organization accounted for most of the variance in thought disorder in a group of chronic schizophrenic patients. In the present study, they examined a possible cognitive mechanism within the semantic system that might produce thought disorder.Method:Twenty patients with chronic schizophrenia and 21 normal comparison subjects were assessed on priming (the ability to respond to a stimulus word more quickly when it is preceded by a semantically related word than when it is preceded by an unrelated word). The patients were divided into subgroups with high (N=9) and low (N=11) levels of thought disorder. The word pairs in the priming paradigm differed in their degree of association but shared a categorical membership. The paradigm involved short stimulus onset asynchronies to maximize automatic processing and required pronunciation of words to minimize decision making. All subjects were also administered neuropsychological tests to assess language, executive function, real-world knowledge, and mental status. Results:Comparison subjects showed appropriate priming in stepwise fashion at the three different levels of word association, as did the patients with mild thought disorder. The patients with high thought disorder showed inhibited responses to high and medium associates compared with their baseline reaction times. Correlations between priming and cognitive variables were significant only with measures of semantic processing. Priming abnormalities were uniformly related to ratings of global thought disorder.Conclusions:These results suggest that aberrations in the automatic spread of activation or facilitation in semantic networks may be a candidate cognitive mechanism in semantic accounts of thought disorder. Am J Psychiatry 1998; 155: 1677-1684
In part I of this study, which appears in this issue of the Journal (1), we found that the difference between semantic fluency and phonologic fluency, as well as a marker of semantic knowledge, significantly predicted the likelihood of thought disorder in schizophrenic patients. In fact, these two variables accounted for 43% of the variance in ratings of thought disorder—more than any other cognitive variable, including those of attention and executive function, which are also characteristically impaired in these patients. Thus, it appeared that thought disorder might reflect semantic processing abnormalities and might not be secondary to failures based on executive function (working memory) or distractibility.
A number of recent studies have also suggested that thought disorder might be related to impaired semantic functioning, rather than impairments in working memory or attentional functions. Feinstein et al. (2) administered a semantic fluency test to patients with schizophrenia and found that their impaired performance on this test was not improved by semantic cueing, an aid to strategic retrieval. Gourovitch et al. (3) demonstrated a specific semantic fluency impairment over and above general impairments on retrieval tests. They showed that while the normal comparison subjects manifested an advantage of semantic fluency over phonologic fluency, no such advantage was shown by the schizophrenic patients. A subsequent study by Aloia et al. (4) examined the organization of the semantic network in schizophrenic patients. The patients were asked to rapidly generate animal names in a fluency task. The proximity with which they clustered certain animals was then compared with the clustering patterns of normal subjects. It was noted that the patients grouped items less consistently and in a less organized manner, again indicating the possibility of semantic disorganization in this population. Taken together, these studies provide strong evidence that semantic storage, utilization, and especially organization may be impaired in patients with schizophrenia.
The goal of part II of this study was to specify the cognitive mechanisms that might account for the semantic abnormality found in part I by experimentally assessing semantic activation in patients with greater and lesser degrees of formal thought disorder. The experimental procedure used a semantic priming paradigm to study automatic spread of activation throughout a semantic network without the effects of conscious attentional processing.
Priming refers to the ability to respond to a transient stimulus more quickly when it is preceded by a related stimulus than when it is preceded by an unrelated stimulus. For example, people tend to respond more quickly to the word “lime” when it immediately follows the word “lemon” than when it follows the word “desk.” When priming occurs within a semantic or associative category (e.g., like “fruit” in the example above), it is called semantic priming.
Priming as an experimental paradigm found its origin in the theory of spreading of activation through a semantic network (5). The crux of this theory is that words, sometimes considered nodes, can excite or inhibit each other. Therefore, related nodes excite each other, so that the elicitation of one is likely to increase the probability of eliciting the other. Some collateral inhibition may also occur, and this inhibition can result in a decreased probability of eliciting or accessing the inhibited node.
Priming may be viewed as a means by which to examine the organization of activational spread through a semantic system. Studies have suggested that when the time interval between two words is relatively short, priming takes place without the use of attentional functions (i.e., is automatic) (6, 7). This suggests that priming is a measure of on-line linguistic production rather than linguistic attention or memory. If one accepts such a spreading of activation model, it is not difficult to see how disorganization of the fundamental associations between words could result in disorganized and convoluted speech.
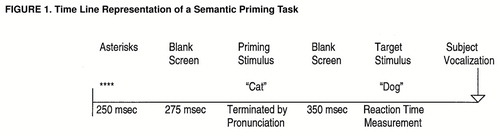
A common method of measuring priming effects is through lexical decision tasks. These priming experiments differ from the paradigm shown in figure 1 (and the one used in this study) in that they require the subject only to judge whether the target stimuli are real words. For example, when “lime” is presented, the subject must respond “yes.” On the other hand, when a nonword, such as “glime,” is presented, she or he must respond “no.” Three such studies (8–10) have reported no differences between normal comparison subjects and schizophrenic patients. Although baseline reaction times for the patient groups were longer in all of the studies, semantic priming was similar to that of the normal comparison groups. However, other investigators (11–13) have found abnormal facilitation in patients with schizophrenia on lexical decision tasks. These researchers found that schizophrenic patients with thought disorder prime more, or “hyperprime,” to directly or indirectly semantically related words (e.g., sweet-lemon) when compared with patients without thought disorder and with normal subjects. However, in the study by Manschreck et al. (11), patients had more rapid absolute reaction times, an anomalous finding that raises issues about the study group. In the study by Spitzer et al. (13), the principal analysis of variance (ANOVA) was not significant (although a trend was present). Moreover, while hyperpriming could suggest that thought-disordered patients may easily become derailed because of spreading activation and/or failures to inhibit, it would not predict relative impairments in semantic fluency as observed in part I of the current study.
There are also two methodological components of priming that must be addressed. First, as stated above, in order to remove the effects of attention, priming should be conducted with the use of short interstimulus intervals (i.e., less than 400 msec) (7). Second, the aforementioned findings came in the context of lexical decision paradigms. The problems with this technique are twofold. First, the subject is asked to perceive the word and then engage in a completely separate process, lexical decision making. Abnormalities in decision making rather than semantic access may skew results. In addition, there is no certainty that the subject is accurately perceiving the word. Therefore, the subject’s response could be artifactual. By requiring the subject to read the words aloud (pronunciation priming) as they appear on the screen and using only correct trials to calculate the priming scores, these problems can be minimized (7).
Two studies (7,14) have directly compared lexical decision and word pronunciation priming in patients with schizophrenia. In the first of these studies (7), the researchers compared patients and normal subjects on lexical decision and word pronunciation priming with the use of short interstimulus intervals and equivalent lists of words. While there were no differences between groups on either of the tasks, patients showed normal priming on the word pronunciation task but showed no priming effect on the lexical decision task. The authors suggested that these findings reflect a deficit in the decision-making process rather than an abnormality of the organization of associations. They did not, however, attempt to reconcile their findings with those of the hyperpriming studies cited above. In the second study (14), these investigators compared the two methods at short interstimulus intervals but using different semantic tasks. One task consisted of words related “vertically,” while the other consisted of words related “horizontally.” Vertical relations meant that the pair consisted of one category name and one category exemplar (e.g., furniture-chair). Horizontal relations consisted of two category exemplars, chosen regardless of relatedness (e.g., table-sofa). Consistent with the previous findings, patients with schizophrenia did not differ from normal comparison subjects on the priming tasks, but they did show a lack of priming on the horizontal, lexical decision task. Similarly, Barch et al. (15) found that patients at short stimulus onset asynchronies displayed priming equivalent to that of normal and psychiatric comparison subjects on a word pronunciation task. Word pairs were “related” but were not intracategorical in nature.
In the present study we sought to identify a cognitive mechanism that might give rise to, and in a sense explain, thought disorder. It should provide a mechanistic explanation, rather than a redescription, of the phenomenon under study (i.e., thought disorder). Evidence for such a candidate mechanism should include 1) differences between groups of normal comparison subjects and patients with higher and lower degrees of thought disorder on semantic measures; 2) associations between clinically rated symptoms of thought disorder, such as derailment, tangentiality, loss of goal, and poverty of content, and related semantic measures, such as semantic fluency, and the candidate mechanism’s measure, thus providing construct validity; 3) a theoretical account of normal semantic processing in which the candidate mechanism can be placed—in the present case it involves spreading semantic activation through a distributed network, and when aberrant it could logically be assumed to perturb the measure of the candidate mechanism; and 4) predictions about ways to perturb the mechanism and to ameliorate abnormalities in both the mechanism and the symptom (through the effects of neuroleptic medication). Ultimately, such a mechanism, with a single computational function, should be found to map to the brain in a reliable manner.
The present study was designed to determine the adequacy of one such candidate mechanism by examining the varying levels of association within a semantic category among schizophrenic patients and normal comparison subjects (given our previous findings of semantic organization deficits in patients) and their relationship to thought disorder through the use of a priming paradigm that assesses spreading semantic activation (to meet criteria 1, 2, and 3). Because of problematic aspects of prior work in this area (see above), we developed a novel semantic priming task that would use short stimulus onset asynchronies to maximize automatic processing, involve word pronunciation to minimize decision making, and use intracategorical word pairs to stress the semantic system, since we hypothesized that real time deficits in speech are most apparent when a given semantic dimension must be traversed. In fact, no study to date has examined the integrity of differing degrees of associations within a given semantic category (i.e., high, medium, and low associations). It is likely that such a study would be better suited for an examination of the overall integrity of the semantic network, because semantic disorganization is not thought to be based on the complete lack of association between words. Instead, semantic organization or disorganization is likely to exist on a continuum of association within well-delineated superordinate categories. In addition, by correlating results in priming with clinically rated thought disorder, on the one hand, and other semantic processing tasks, including verbal fluency, on the other hand, we might provide construct validity for a cognitive mechanism. We hypothesized that patients with low levels of thought disorder would exhibit normal priming, that patients with higher levels of thought disorder would show abnormal priming to within-category pairs, and that associations between priming and both other semantic processing measures and thought disorder would be observed.
METHOD
Twenty inpatients (15 male and five female) of the 23 from the National Institute of Mental Health neuropsychiatric research hospital described in part I of this report participated in this study. All of the patients met the DSM-IV criteria for schizophrenia. Patients in this study generally had had multiple hospital admissions and showed incomplete responses to conventional treatments. All of the patients were receiving neuroleptic medication at the time of the study (clozapine, N=9; risperidone, N=4; high-potency drugs, namely, haloperidol, fluphenazine, or loxapine, N=7, of whom six also received anticholinergic medication). Twelve of the patients met criteria for a prominent thought disorder (explained below), and eight were considered less thought-disordered.
Twenty-one normal comparison subjects (12 male and nine female) of the 23 described in part I were also recruited for this study. No comparison subject or patient with a history of traumatic brain injury, epilepsy, developmental disorder, diagnosable substance dependence, or other known neurologic condition was included in the study.
Tests and Measures
Semantic priming measure
Twenty-six word pairs were used for each of the three degrees of relatedness (high, medium, and low) within a given semantic category. Each word pair was judged to be composed of frequent members of the same category according to normative data on category exemplars that are commonly used in priming task development (16). In addition, the degree of association was judged as high, medium, or low with the use of word association norms from a study by Jenkins (17): a word was considered highly related to another word if subjects used it as a first response in a word association paradigm at least 50% of the time. A medium relationship occurred as a first response 25%–40% of the time, and low relationships occurred 8%–15% of the time.
After category exemplars were chosen from the Rosch list (16), they were found on the Jenkins list (17) to see what were high, medium, and low associates of these words. Among these levels of associates, same-category words were chosen for the pairings. Another reference of word association (18) was used to validate the association of the words on the three related lists. Pairs were eliminated if any particular word was repeated across word pairs or if there was little consistency between the two sets of norms. Thirty-four word pairs were eliminated for these reasons. Once the three related lists (high, medium, and low associates) were chosen, they were equated for the relative frequency of their occurrence in the English language with the use of the word frequency norms developed by Kucera and Francis (19). A fourth list of words from the Rosch list was developed and consisted of 45 unrelated word pairs. Average frequency was similar across all four lists.
The software program (and some of the hardware) used for controlling the presentation of the stimuli and for the initial analysis of data for the priming task was from Micro Experimental Laboratory (20). The hardware consisted of the following: a low-impedance, high-output unidirectional Electret remote microphone; an RB-100 response box to record responses from the remote microphone; and an IBM-compatible personal computer with a NEC MultiSync 3D Super VGA monitor for presentation of the stimuli and storage of the data.
The microphone was used so that the reaction time could be assessed from the point at which the subject first initiated a verbal response in the word pronunciation, semantic priming task. It had an impedance of 600 Ω and was designed to detect responses of 20,000 to 30,000 Hz. However, adjustments were made to the RB-100 response box as directed by the Micro Experimental Laboratory manual (20) so that extraneous noise detection would be minimized. The display of the stimuli and recording of the reaction times (in milliseconds) were controlled by Micro Experimental Laboratory software. Stimuli were presented in a fixed random order so that no stimulus was presented twice to any one subject.
Cognitive measures and ratings
Other tests and scales used in this study included the Wide Range Achievement Test—Revised (reading subtest), the Boston Naming Test, the difference between semantic fluency and phonologic fluency, the Peabody Picture Vocabulary Test, the Wisconsin Card Sorting Test, the Letter-Number Span test, the attention subtest of the Dementia Rating Scale, and the Scale for the Assessment of Thought, Language, and Communication, all of which are described in part I of this study (1).
Procedure
Administration and scoring of the tests listed above are described in greater detail in part I of this study. For the semantic priming task, the subject was seated in front of a CRT screen, holding the remote microphone, and read the following instructions: “You are getting ready to begin an experiment on the computer. First you will see a row of stars. Then a word will appear on the screen. Pronounce that word as quickly as possible. A second word will then appear and you are also to pronounce that word as quickly as possible.”
A practice block of 15 word pairs was administered first to prepare the subject for the task. The actual testing consisted of three experimental blocks, each of which included high-, medium-, and low-association word pairs and unrelated pairs. A total of 123 word pairs were presented to each subject (26 pairs for each of the three related conditions and 45 pairs of unrelated words). Responses below 100 msec and above 1000 msec were excluded from the analyses because they were thought to represent error rather than true responding; responses faster than 100 msec are physiologically unlikely, and those slower than 1000 msec suggest a failure of the system to detect responses accurately. Less than 10% of all responses were excluded for these reasons. Each trial proceeded along the framework illustrated in figure 1.
Median reaction times were calculated by block for each subject in each condition in order to reduce the impact of outliers. The means of these three medians (one for each block of trials) were then calculated, giving the investigators average medians for each subject for each condition (high-, medium-, and low-association pairs and unrelated pairs). We then used the following formula to calculate the percent change from baseline reaction time for each priming condition: (URT–RRT)/URT×100=prime, where URT is the average median reaction time to the second word of an unrelated pair, and RRT is the average median reaction time to the second word of a related pair. This computation enabled us to correct for slowed absolute reaction times in the schizophrenic group.
RESULTS
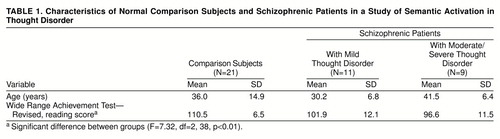
Demographic data for the three groups are presented in table 1. The groups were matched on age but not on putative premorbid intellectual level. This difference was accounted for by general differences between the patients and the normal comparison subjects as a whole and was not specific to differences between the two patient subgroups as assessed with Tukey’s honestly significant difference contrasts. In addition, premorbid intellectual level was not strongly related to semantic priming, since correlations between priming and reading scores on the Wide Range Achievement Test—Revised were rather low (r=0.02–0.22 for the three levels of priming, p>0.05). On the basis of the ratings on the Scale for the Assessment of Thought, Language, and Communication, nine patients with global scores greater than 2 were considered to exhibit relatively high amounts of thought disorder, while the remaining 11 patients were considered to exhibit little thought disorder. The rationale for this is described more fully in part I.
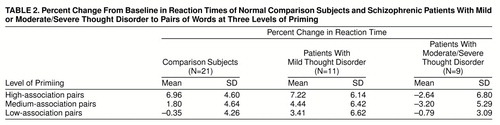
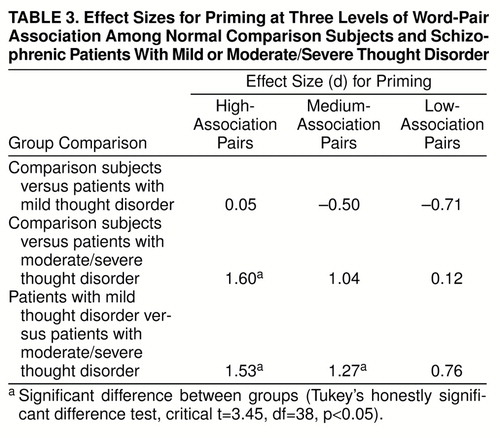
The means and standard deviations of each group for the three levels of priming are presented in table 2. A 3 (normal comparison subjects, high thought disorder patients, low thought disorder patients) ¥ 3 (high, medium, and low semantic associates) ANOVA was conducted on the priming data. There were main effects for group (F=6.72, df=2, 38, p<0.005) and degree of association (F=7.10, df=2, 38, p<0.005), as well as an interaction between the two (F=3.37, df=2, 38, p<0.05). Effect sizes (d) and post hoc t and p values are shown in table 3. Group comparisons revealed nonsignificant small or moderate differences in effect size between the normal comparison subjects and the patients with mild thought disorder. A comparison of the normal comparison subjects and the patients with higher levels of thought disorder revealed a large and significant effect in the high-association condition, with the normal subjects showing priming more than the patients (who actually displayed inhibition to related pairs). Finally, the group with lesser thought disorder showed priming significantly more than the group with greater thought disorder at the high- and medium-association levels.
The priming ability of each group at each level of semantic association was examined by means of t tests. The normal comparison subjects showed significant priming in both the high- and medium-association conditions (t=7.15, df=20, p<0.001, d=3.20, and t=2.11, df=20, p<0.05, d=0.94, respectively) but not in the low-association condition (t=–0.38, df=20, p>0.05, d=–0.17). The patients with mild thought disorder also showed significant priming in the high- and medium-association conditions (high: t=4.10, df=10, p<0.005, d=2.46; medium: t=2.45, df=10, p<0.05, d=1.48) but not the low-association condition (t=1.86, df=10, p=0.09, d=1.12). The patients with higher levels of thought disorder did not show priming in any association condition (high: t=–1.20, df=8, p>0.05, d=–0.85; medium: t=1.78, df=8, p>0.05, d=–1.34; low: t=0.83, df=8, p>0.05, d=–0.63).
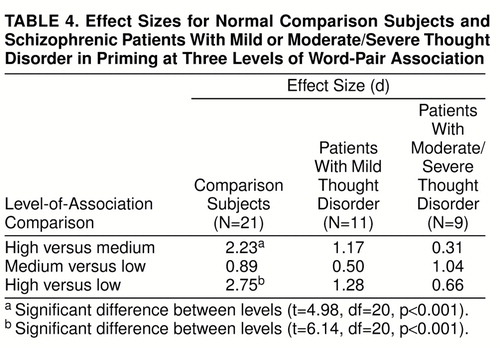
Table 4 shows effect sizes for the comparison of different levels of priming within each group. The normal comparison subjects appeared to prime “lawfully”: high associates were responded to significantly more quickly than medium associates, medium associates were responded to more quickly than low associates, although not significantly so, and high associates were responded to significantly more than low associates. The patients with low levels of thought disorder did not differ in reaction time in the high- versus medium-association contrast, the high- versus low-association contrast, and the medium- versus low-association contrast. The patients with moderate or severe thought disorder had no significant differences between high and medium associates, medium and low associates, and high and low associates; however, the effect size for the comparison between medium and low associates was large (d>0.80).
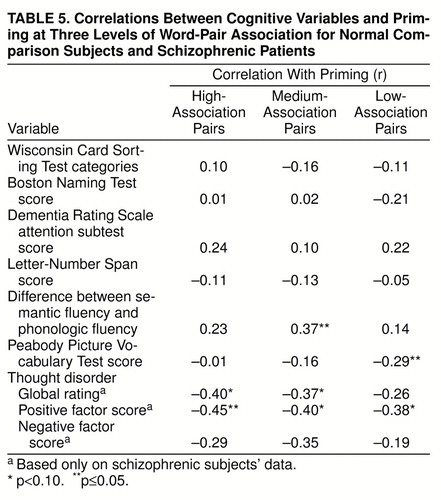
Correlations between scores on various cognitive tests and the three levels of priming are presented in table 5. Additionally, and perhaps most crucially, priming was negatively correlated with positive thought disorder. Thus, the less patients exhibited priming, the higher was their positive thought disorder (i.e., level of disorganized speech). This was especially true for the high and medium associations, conditions in which the more thought-disordered patients displayed inhibition. Second, only semantic measures correlated with priming measures; tests of attention and working memory did not. In particular, a key measure identified in part I of the study, the verbal fluency difference score, was associated with degree of priming, such that the greater ease with which subjects accessed semantic exemplars (controlling for retrieval and attentional factors), the more they showed priming to associates (at least in the medium-association condition). Thus, the subjects who exhibited minimal advantage in semantic fluency over phonologic fluency were also those who exhibited the least priming.
DISCUSSION
This study, designed as a part of a series of studies assessing the association between semantic organization and thought disorder, suggests that abnormalities in priming provide a tenable underpinning for impairments in the organization and, ultimately, the production of speech as manifested in ratings of thought disorder in patients with schizophrenia. In part I of the study we found that variables assessing semantic organization and knowledge predicted 43% of the variance in ratings of thought disorder. In addition, no executive function or traditional language variables added to the strength of the prediction.
In this part of the series, we focused on applying an experimental approach to the evaluation of semantic organization by means of a semantic priming paradigm. Correlations between semantic priming and thought disorder were consistently high. Correlations between priming and other cognitive variables were relatively low unless the cognitive variable involved semantic manipulation/knowledge (i.e., differences in verbal fluency and Peabody Picture Vocabulary Test scores). Therefore, the integration of the priming results with the results from the previous part of the study adds support to the association between semantic organization and thought disorder. The priming data themselves can be examined by asking a series of basic questions. Do the groups demonstrate priming, and if so, does priming occur “lawfully” across levels of association? Do the groups differ in their priming abilities?
It is clear that in normal comparison subjects, priming occurs most with high-association word pairs, significantly less with medium-association pairs, and not at all with low-association pairs. This differential priming validates the separation of these word pairs into their respective groupings. Low associations may not be environmentally relevant or frequent and therefore are not functionally useful.
Priming among the schizophrenic patients with low levels of thought disorder was similar to that among normal subjects, although at greater levels. This does not represent a qualitative abnormality, given that among these patients, priming occurred most with high associates, moderately with medium associates, and least with low associates. However, the lack of differentiation between medium and low associates is unique to this group. Less differentiation implies less organization and a less “complete” network, a finding implied in some previous studies with schizophrenic subjects (21, 22).
Finally, among the patients with greater thought disorder, priming did not occur at any level of association. They actually inhibited responses to high and medium associates. Consistent with these results, Ober et al. (23) recently observed that nonsignificant semantic priming occurs only in schizophrenia under automatic (e.g., short stimulus onset asynchrony) conditions in lexical decision tasks, and Passerieux et al. (24) found that thought-disordered patients failed to demonstrate priming, while normal subjects and non-thought-disordered subjects showed priming (although reaction times were unusually long for all groups in that study). This has the important implication that patients with thought disorder may have difficulty in automatically activating highly semantically related and relevant words in connected speech. As a result they may “select” or activate another word that is less semantically appropriate, that is removed in semantic distance, and hence is experienced by the listener as a “loose association.” Our results are also compatible with those of Gurd et al. (22), who, using a semantic search paradigm in which schizophrenic patients had to find a word that belonged to a specific semantic category, suggested that the patients had reduced connection strengths in their language processing systems, as evidenced by slower and less accurate responses.
The results of this study shed light on several aspects of semantic organization in patients with schizophrenia (with greater or lesser degrees of a formal thought disorder) and in normal comparison subjects. First, this study was the first to examine semantic priming across degrees of word relatedness within a superordinate category. In so doing, a lawful priming effect, often hypothesized in the literature, was demonstrated empirically in normal comparison subjects. In addition, hyperpriming and normal priming, both of which have been documented in patients with schizophrenia, were found to be a function of the interaction between thought disorder and the degree of association of the words (e.g., subtle hyperpriming in patients with mild thought disorder occurred only in the medium- and low-association conditions). Second, a marked distinction, both quantitative and qualitative, between the performance of schizophrenic patients with greater and lesser degrees of thought disorder was observed. It was based on findings that thought-disordered patients not only showed reduced priming but also demonstrated negative priming in response to the very pairs of related words that should have resulted in maximal priming. Third, we believe we have met criteria for a candidate cognitive mechanism for thought disorder. Not only were systematic differences in priming between the groups with greater and lesser thought disorder observed, but significant correlations between 1) the degree to which patients did not exhibit priming and severity of thought disorder and 2) the degree to which patients did not exhibit priming and abnormalities in semantic processing (e.g., differential semantic fluency impairments) were also observed.
It is important to recognize that although we divided our schizophrenic group into subgroups with greater and lesser degrees of clinically rated thought disorder, we are not suggesting that these represent dichotomous subtypes. Rather, we believe that thought disorder, like other cognitive pathologies, lies on a continuum based on severity. We divided the patients for illustrative purposes, so that we might more incisively determine the cognitive underpinnings of the symptom. The correlations between thought disorder and such semantic processing measures as semantic priming (found here) and semantic fluency (found in part I of this report) within the whole group of patients indicate that indeed the symptom is continuous and without hard-and-fast boundaries.
In summary, semantic organization in patients with thought disorder may be abnormal because of deviant spread of activation through a semantic network. In this population, thought disorder is seen to be a function of automatic priming of the semantic system and the relatedness of the word pairs. Moreover, we found additional evidence for associating thought disorder with speech and language and not with executive function. Thus, in parts I and II of this examination of thought disorder, measures of semantic production and organization have been closely related to, and even predictive of, thought disorder. Finally, we have identified a candidate cognitive mechanism for one of the hallmark symptoms of schizophrenia and now look forward to developing a better understanding of the effects of treatment on this mechanism.
Received Nov. 19, 1997; revision received May 22, 1998; accepted June 8, 1998. From the Clinical Brain Disorders Branch and the Experimental Therapeutics Branch, NIMH. Address reprint requests to Dr. Goldberg, Clinical Brain Disorders Branch, NIMH, Bldg. 10, Rm. 4S235, MSC 1379, Bethesda, MD 20892-1379.
 |
 |
 |
 |
 |
1. Goldberg TE, Aloia MS, Gourovitch ML, Missar D, Pickar D, Weinberger DR: Cognitive substrates of thought disorder, I: the semantic system. Am J Psychiatry 1998; 155:1671–1676Link, Google Scholar
2. Feinstein A, Nowlin B, Weinberger DR, Goldberg TE: Types and characteristics of remote memory impairment in schizophrenia. Schizophr Res (in press)Google Scholar
3. Gourovitch ML, Goldberg TE, Weinberger DR: Verbal fluency deficits in patients with schizophrenia: semantic fluency is differentially impaired as compared to phonologic fluency. Neuropsychology 1996; 6:573–577Crossref, Google Scholar
4. Aloia MS, Gourovitch ML, Weinberger DR, Goldberg TE: An investigation of semantic space in patients with schizophrenia. J Int Neuropsychol Society 1996; 2:267–273Crossref, Medline, Google Scholar
5. Collins AM, Loftus EF: A spreading activation theory of semantic processing. Psychol Rev 1975; 82:407–428Crossref, Google Scholar
6. Nebes RD, Brady BB, Huff FJ: Automatic and attentional mechanisms of semantic priming in Alzheimer disease. J Clin Exp Neuropsychol 1989; 11:219–230Crossref, Medline, Google Scholar
7. Vinogradov S, Ober BA, Shenaut GK: Semantic priming of word pronunciation and lexical decision in schizophrenia. Schizophr Res 1992; 8:171–181Crossref, Medline, Google Scholar
8. Chapin K, Vann LE, Lycaki H, Josef N, Meyendorff E: Investigation of the associative network in schizophrenia using the semantic priming paradigm. Schizophr Res 1989; 2:355–360Crossref, Medline, Google Scholar
9. Chapin K, McCown J, Vann L, Kenney D, Youssef I: Activation and facilitation in the lexicon of schizophrenics. Schizophr Res 1992; 6:251–255Crossref, Medline, Google Scholar
10. Henik A, Priel B, Umansky R: Attention and automaticity in semantic processing of schizophrenic patients. Neuropsychiatry Neuropsychol Behav Neurol 1992; 5:161–169Google Scholar
11. Manschreck TC, Maher BA, Milavetz JJ, Ames D, Weisstein CC, Schneyer ML: Semantic priming in thought disordered schizophrenic patients. Schizophr Res 1988; 1:61–66Crossref, Medline, Google Scholar
12. Spitzer M, Braun U, Hermle L, Maier S: Associative semantic network dysfunction in thought-disordered schizophrenic patients: direct evidence from indirect semantic priming. Biol Psychiatry 1993; 34:864–877Crossref, Medline, Google Scholar
13. Spitzer M, Weisker I, Winter M, Maier S, Hermle L, Maher BA: Semantic and phonological priming in schizophrenia. J Abnorm Psychol 1994; 103:485–494Crossref, Medline, Google Scholar
14. Ober BA, Vinogradov S, Shenaut GK: Semantic priming of category relations in schizophrenia. Neuropsychology 1995; 9:220–229Crossref, Google Scholar
15. Barch DM, Cohen JD, Servan-Schreiber D, Steingard S, Steinhauer SS, Van Kammen DP: Semantic priming in schizophrenia: an examination of spreading activation using word pronunciation and multiple SOAs. J Abnorm Psychol 1996; 105:592–601Crossref, Medline, Google Scholar
16. Rosch E: Cognitive representations of semantic categories. J Exp Psychol Gen 1975; 104:192–233Crossref, Google Scholar
17. Jenkins JJ: The 1952 Minnesota word association norms, in Norms of Word Association. Edited by Postman L, Keppel G. New York, Academic Press, 1970, pp 1–35Google Scholar
18. Palermo DS, Jenkins J: Word Association Norms. Minneapolis, University of Minnesota Press, 1964Google Scholar
19. Kucera H, Francis WN: Computational analysis of present-day American English. Providence, RI, Brown University Press, 1967Google Scholar
20. Schneider W: Micro Experimental Laboratory: an integrated system for IBM PC compatibles. Research Methods, Instruments, & Computers 1988; 20:206–217Crossref, Google Scholar
21. Chen EYH, Wilkins AJ, McKenna PJ: Semantic memory is both impaired and anomalous in schizophrenia. Psychol Med 1994; 24:193–202Crossref, Medline, Google Scholar
22. Gurd JM, Elvevaag B, Cortina-Borja M: Semantic category word search impairment in schizophrenia. Cognitive Neuropsychiatry 1997; 2:291–302Crossref, Medline, Google Scholar
23. Ober BA, Vinogradov S, Shenaut GK: Automatic versus controlled semantic priming in schizophrenia. Neuropsychology 1997; 11:506–513Crossref, Medline, Google Scholar
24. Passerieux C, Segui J, Besche C, Chevalier JF, Widlocher D, Hardy-Bayle MC: Heterogeneity in cognitive functioning of schizophrenic patients evaluated by a lexical decision task. Psychol Med 1997; 27:1295–1302Crossref, Medline, Google Scholar

