
Dispositional Predictors of Problem Gambling in Male Adolescents
Abstract
OBJECTIVE: This study investigated the possible relationship between impulsivity in early adolescence and gambler status in late adolescence. METHOD: Impulsivity measures consisting of self-reports and teacher ratings were gathered from 754 boys in early adolescence, and their gambling status in late adolescence was assessed with a self-report measure. RESULTS: On both measures of impulsivity, nongamblers had the lowest scores, recreational gamblers had the next higher scores, low problem gamblers had still higher scores, and high problem gamblers had the highest scores. CONCLUSIONS: These findings support the DSM-IV classification of problem gambling as a deficit in impulse control. (Am J Psychiatry 1997; 154:1769–1770)
Pathological gambling has been classified as a disorder of impulse control by the American Psychiatric Association (DSM-IV). In support of this classification, some studies have found that pathological gamblers are highly distractible and have poor impulse control (1–3). These results suggest that impulsivity is a dispositional attribute of gamblers. However, most studies have used gamblers who were entering or were already in treatment. These individuals may represent only a subset of problem gamblers in the community. In addition, almost all of these studies have used cross-sectional designs, which cannot establish the direction of the relationship between personal dispositions and gambling, or retrospective reports, which are subject to distortion and memory problems. Finally, all of the previous studies used adult study groups, even though adolescent subjects might better reveal predisposing personality factors—those that existed before pathological gambling developed. In sum, we do not yet know whether pathological gamblers have poor impulse control before they start gambling. If we find that they do, we will have a clearer picture of the personality precursors of gambling.
The objective of the present study was to establish a link between gambling status (i.e., high problem gambler, low problem gambler, recreational gambler, or nongambler) and impulsivity. Impulsivity was assessed during early adolescence, and gambling status was established during late adolescence. Because pathological gambling is more prevalent in males than females, especially during adolescence (4), only male subjects were studied.
METHOD
The 754 boys who participated in the study were part of an ongoing longitudinal study group. They were French-speaking Caucasians living in disadvantaged neighborhoods in Montreal, Canada. The original group of 1,034 was a nonselected community sample that represented 87% of all boys in 53 schools. Written consent was obtained from both the boys and their parents.
A French translation of the South Oaks Gambling Screen for Adolescents (5) was administered when the boys were 17 years old. This instrument assesses problem severity over the past 12 months by means of 12 items, which are answered either yes or no. The frequency over the past 12 months of 11 different gambling activities was also assessed, and a total frequency-by-diversity score was computed by adding the frequency scores. Cronbach's alpha for internal consistency was 0.78 for the problem severity scale and 0.77 for the frequency-by-diversity scale.
Self-reported impulsivity had been assessed when the boys were 13 years of age with the use of the following five impulsiveness items, which had the highest factor loadings on the Eysenck Impulsiveness Scale (6). 1) Do you generally do and say things without stopping to think? 2) Do you often get into trouble because you do things without thinking? 3) Are you an impulsive person? 4) Do you usually think carefully before doing anything? 5) Do you mostly speak before thinking things out? Items could be answered yes (scored 1) or no (scored 0) (alpha for internal consistency=0.69).
Teachers had also rated the boys' impulsive behaviors at age 13 years using the following three items. 1) Jumps from one activity to another without finishing. 2) Attracts attention by shouting. 3) Acts without reasoning. Items were scored 0, 1, or 2, depending on the frequency of each behavior (alpha for internal consistency=0.71).
Boys who scored 3 or more on the problem severity scale of the South Oaks Gambling Screen for Adolescents were included in the high problem gambler group (N=38). A cutoff score of 3 was selected on the basis of previous research (5). Those who scored 1 or 2 were considered low problem gamblers (N=109). The remaining boys who had scores of 0 on the problem severity scale but scores of 1 or more on the frequency/diversity scale were classified as recreational gamblers (N=381). The others with scores of 0 on both scales were considered nongamblers (N=226).
RESULTS
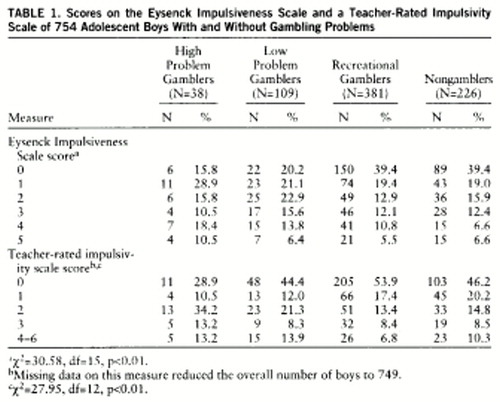
A chi-square analysis was performed to test the relationship between gambling group membership and scores on the Eysenck scale (scores=0–5). The analysis revealed a significant relationship (table 1). As can be seen in table 1, there was a linear trend for scores on impulsiveness to increase across the groups, from nongamblers to recreational gamblers to low problem gamblers to high problem gamblers.
A similar analysis was performed with teacher-rated impulsivity. Scores on this measure could vary from 0 through 6, but because of the small number of participants in some cells, scores of 4, 5, and 6 were collapsed. As in the analysis of Eysenck scale scores, across groups (nongamblers and recreational, low problem, and high problem gamblers) teachers' ratings of impulsivity increased (table 1).
Finally, the four groups were compared on their gambling behavior at age 13 to test whether between-group differences already existed when impulsivity measures were collected. Subjects had answered the question, Over the past 12 months, how often did you gamble for money with people who are not family members? Possible answers were never, a few times, often, or very often. No interaction between group membership and response category was found (p>0.25).
DISCUSSION
The purpose of this study was to test the relationship between gambling status during late adolescence and impulsivity measures collected during early adolescence. The results indicated that on both measures of impulsivity, nongamblers scored lowest, followed by recreational gamblers, low problem gamblers, and high problem gamblers.
These results support earlier findings that adult pathological gamblers have concurrent impulse control deficits or have had such deficits during childhood (1–3, 7). Altogether, these results are consistent with the DSM-IV classification of pathological gambling as an impulse control deficit. But these results go a step further: they show that for problem gamblers, impulse control deficits precede later gambling problems.
 |
Received Sept. 12, 1996; revisions received March 17 and June 2, 1997; accepted July 10, 1997. From the Research Unit on Children's Psycho-Social Maladjustment, University of Montreal. Address reprint requests to Dr. Vitaro, Research Unit on Children's Psycho-Social Maladjustment, University of Montreal, 750 Gouin Boulevard East, Montreal, Que., Canada H2C 1A6.
1. Carlton PL, Manowitz P: Physiological factors as determinants of pathological gambling. J Gambling Behavior 1987; 3:274–285Crossref, Google Scholar
2. Castellani B, Rugle L: A comparison of pathological gamblers to alcoholics and cocaine misusers on impulsivity, sensation seeking, and craving. Int J Addict 1995; 30:275–289Crossref, Medline, Google Scholar
3. Rugle L, Melamed L: Neuropsychological assessment of attention problems in pathological gamblers. J Nerv Ment Dis 1993; 181:107–112Crossref, Medline, Google Scholar
4. Lesieur HR, Klein R: Pathological gambling among high school students. Addict Behav 1987; 12:129–135Crossref, Medline, Google Scholar
5. Winters KC, Stinchfield RD, Fulkerson J: Toward the development of an adolescent gambling problem severity scale. J Gambling Studies 1993; 9:63–82Crossref, Google Scholar
6. Eysenck SBG, Eysenck HJ: Impulsiveness and venturesomeness: their position in a dimensional system of personality description. Psychol Rep 1978; 43:1247–1255Google Scholar
7. Carlton PL, Manowitz P: Behavioral restraint and symptoms of attention deficit disorder in alcoholics and pathological gamblers. Neuropsychobiology 1992; 25:44–48Crossref, Medline, Google Scholar

