Integrating Clinical and Basic Research: Opioid Use Disorder, Psychotic Illnesses, and Prefrontal Microcircuits Relevant to Schizophrenia
Publication: American Journal of Psychiatry
This issue of the Journal brings together papers that have treatment implications with papers that also address basic mechanisms underlying psychopathology, with a specific focus on opioid use disorder, psychotic disorders, and schizophrenia. There are two papers on opiate use disorders: one that presents data linking opiate prescribing patterns to prescription-related opiate misuse, the other demonstrating that medication treatment for opioid use disorders is associated with reduced suicide rates. In relation to psychotic disorders, we include a paper that supports the importance of early intervention and detection strategies by providing valuable 20-year longitudinal follow-up data from individuals after their first psychotic episode.
At the basic research level, two papers focus on cortical microcircuits and cellular/molecular alterations that are associated with schizophrenia. An overview presents a cell type-specific, circuit-based understanding of normal and altered prefrontal cortical function. This is highly relevant for understanding maladaptive cognitive and emotional processes involved in psychopathology, particularly the cognitive deficits that occur in individuals with schizophrenia. In an accompanying original research paper, human postmortem data are used to identify molecular alterations at the level of the synapse in dorsolateral prefrontal cortex (dlPFC) neurons that are associated with schizophrenia and its neurophysiological correlates. Furthermore, by using computational modeling, the researchers plausibly link these synaptic alterations to features of prefrontal cortical dysfunction that are associated with schizophrenia, such as reduced gamma wave oscillatory power.
Understanding Prefrontal Cortical Microcircuitry in Relation to Psychopathology
Cognitive symptoms and cognitive impairments are common across various psychiatric illnesses, and this is particularly evident in schizophrenia in which impaired cognition is a substantial contributor to functional disability. An overview by Dr. Vikaas Sohal from the University of California at San Francisco focuses on cortical microcircuits in relation to schizophrenia-related cognitive deficits, explaining why it is important to understand how different neuronal cell types, and the microcircuits that they constitute, underlie prefrontal executive functions (1). This overview begins with a discussion of cortical gamma oscillations, which reflect high frequency coordinated neuronal activity, and are thought to be a neurophysiological intermediary between prefrontal cortical microcircuit activity and cognitive functioning. Evidence for reduced gamma oscillatory activity in schizophrenia is presented, as is the linkage between alterations in gamma rhythms and schizophrenia-related cognitive deficits. The overview further describes the current understanding of the neuronal cell types and microcircuits that generate gamma oscillations, with a specific focus on the mechanistic involvement of parvalbumin inhibitory interneurons. Finally, the review speculates about the possibility of using gamma oscillations, or components of the prefrontal microcircuit that mediate these oscillations, as novel treatment targets for schizophrenia-related cognitive deficits.
Postmortem Brain Studies Reveal Prefrontal Synaptic Alterations Relevant to Reduced Gamma Oscillation Power and Working Memory in Schizophrenia
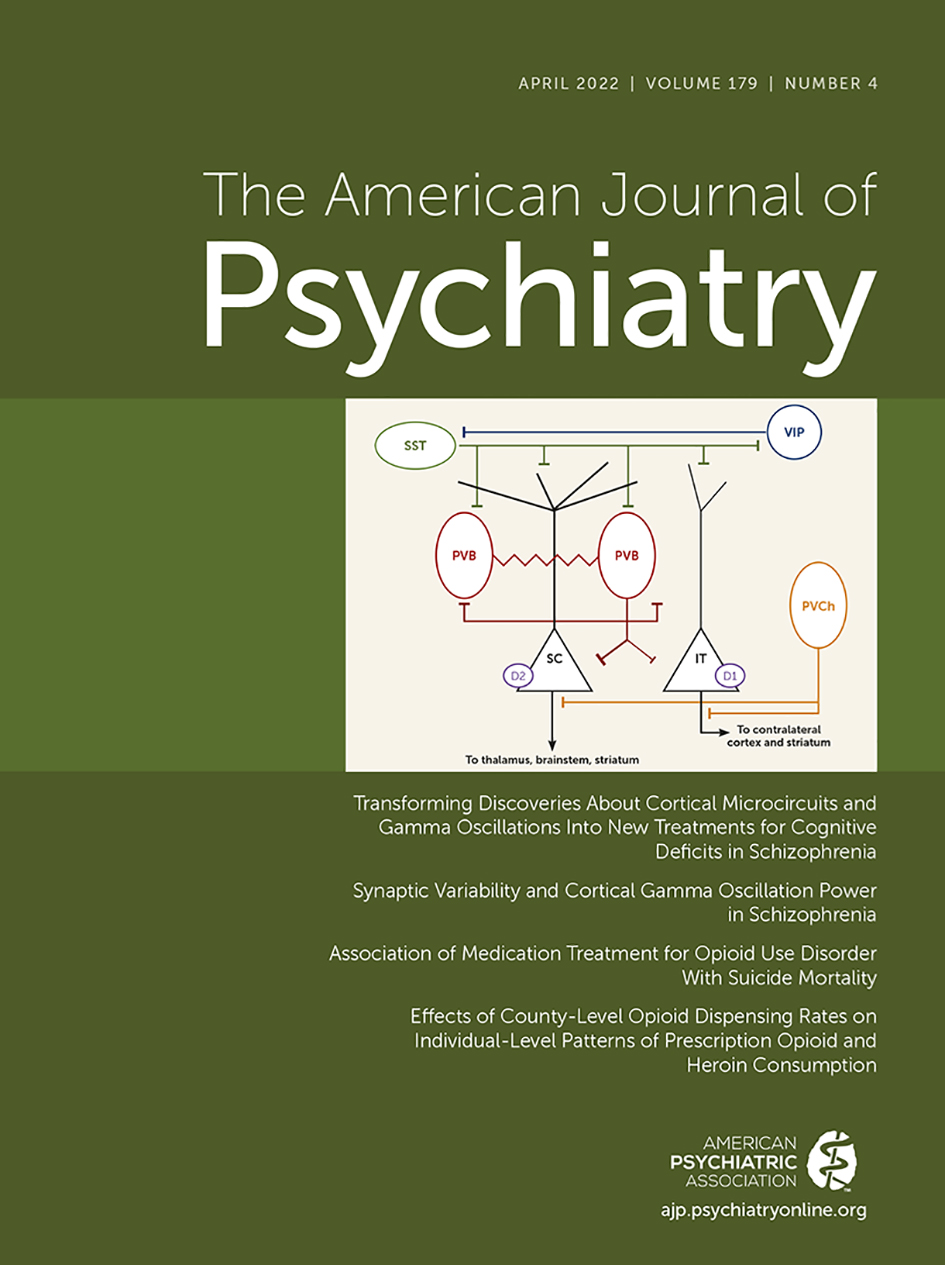
Considerable research has characterized numerous postmortem molecular alterations in brains from subjects with schizophrenia, providing a panoply of molecular findings that are associated with the long-term consequences of having this illness. A critical component of this line of research is to identify the extent to which the multitude of postmortem findings are related to the etiology or pathophysiology of schizophrenia versus being due to other nonspecific factors associated with having schizophrenia, such as chronic illness-related changes in lifestyle or effects of long-term medication exposure. Chung et al. (2) provide new insights into the synaptic alterations within the dlPFC that in individuals with schizophrenia are linked to neurophysiological processes relevant to impairments in working memory. It is well known that dlPFC function is altered in individuals with schizophrenia, and these alterations are thought, in part, to mediate the working memory impairments that contribute to functional disability. Within the dlPFC, gamma band electrical activity (30–80 Hz) constituting gamma oscillatory rhythms has been directly linked to working memory performance. And, like altered working memory, gamma oscillatory power is reduced in individuals with schizophrenia. Furthermore, evidence suggests that within the dlPFC, a specific microcircuit comprised of excitatory pyramidal neurons synapsing onto parvalbumin inhibitory interneurons is involved in mediating gamma oscillatory rhythms. By assessing markers of excitatory synaptic strength (i.e., vesicular glutamate transporter 1 and postsynaptic density 95) in dlPFC tissue from 20 subjects with schizophrenia and 20 control subjects, the authors demonstrate that individuals with schizophrenia have increased variability in the strength of excitatory inputs onto parvalbumin interneurons. With computational network modeling the authors further show that this increased variation in excitatory synaptic strength could, in part, account for the reduction in gamma oscillatory power observed in schizophrenia subjects. It is noteworthy that, on average, the markers of excitatory synaptic strength were not found to differ between schizophrenia brains and control brains but rather schizophrenia brains were characterized by increased variability of excitatory synaptic strength on dlPFC parvalbumin interneurons. Additionally, by using dlPFC tissue from nonhuman primates exposed to haloperidol or olanzapine, the researchers demonstrate that these findings are unlikely to be due to antipsychotic treatment. The data presented in this paper further support the strategy of therapeutically targeting specific components of prefrontal microcircuitry with the goal of developing novel therapeutics aimed at improving the cognitive impairments associated with schizophrenia and other psychiatric disorders.
Associations Between Duration of Untreated Psychosis and 20-Year Outcomes
Numerous studies have examined the impacts of the duration of untreated psychosis (DUP) on symptomatic and functional outcomes in individuals after their first psychotic episode. While, in general, the data confirm the finding that longer delays to engage in treatment are associated with poorer outcomes, the reasons underlying this relation have been attributed to various factors that are associated with prolonged DUPs. These include the possibility that severity of illness is associated with a longer time to treatment or that increased neurotoxicity occurs during a lengthy untreated period. Alternatively, a recent paper suggests the possibility that this association could be an artifact, or a confound in the analysis termed “lead time bias,” such that longer DUPs reflect earlier detection of the illness and that this is not accounted for when assessing treatment-related long-term outcomes (3, 4). O’Keeffe and colleagues (5) provide important insights into the long-term relation between DUP and outcomes by longitudinally following a cohort of patients for up to 20 years after presenting for treatment with their first psychotic episode. Starting with 171 participants, patients were assessed longitudinally at 6 months and 4, 8, 12, and 20 years, with 80 subjects completing assessments for the entire 20 years. Seventy-nine percent of the sample was determined to have a nonaffective psychosis, whereas 21% were categorized with an affective psychosis. Analyses were focused on the relation between DUP and longitudinal trajectories of symptom measures, functional outcomes, and quality of life. While different time-related trajectories were found for the relations between DUP and specific outcome parameters, overall the findings demonstrated that longer DUPs were associated with poorer outcomes (i.e., positive and negative symptoms, symptoms related to functional capacity, and quality of life). Although these findings cannot address issues of causality, they are important because they demonstrate the long-term, persistent relation between DUP and outcomes. The authors suggest in their conclusion that these findings, associating prolonged DUPs to deleterious outcomes, further support the value of early intervention treatment programs. In his editorial (6), Dr. Ashok Malla from McGill University discusses the efficacy of early intervention services, highlights the factors that contribute to prolonged DUPs, and emphasizes the potential therapeutic value of reducing DUPs in individuals with psychotic illnesses.
Decreased Suicide Risk Related to Medication Treatment for Opioid Use Disorder
Building on prior research, Watts et al. (7) present data that confirm and extend previous findings demonstrating that stable medication treatment for opioid use disorder reduces mortality risk. Using data from 2003 to 2017, from 61,633 VA patients that received medication treatment for opioid use disorder, the researchers sought to understand the impacts of treatment on deaths due to “external causes,” which include deaths due to intentional (i.e., suicide) and unintentional accidents or injury, as well as total deaths due to all-cause mortality. It is noteworthy that, while large, the sample was generally homogeneous with male subjects constituting 92.8% of the sample; 71% of the sample was White, 19.5% Black, and 5.5% Hispanic. Additionally, 66% of the participants had at least one mental health diagnosis and 35.4% had at least three mental health diagnoses. Data were analyzed for patients for up to 5 years after they initiated treatment, and the researchers also determined whether differences in mortality risk were associated with the different medication treatments (i.e., methadone, buprenorphine, or naltrexone). Over the follow-up period 6,608 deaths occurred, with 2,374 attributed to external causes, of which 298 were suicides. When receiving stable medication treatment, the hazard ratio for suicides decreased to 0.45 and for all-cause mortality to 0.33 relative to when individuals were stably off treatment. The hazard ratios for suicides associated with starting and ending treatment did not significantly differ when compared to being stably off treatment. However, the hazard ratio for all-cause mortality decreased to 0.59 when assessed during the first 14 days of treatment and increased to 1.14 when stopping treatment. In relation to the use of specific agents, 50.2% percent of treated individuals received buprenorphine, 25.1% methadone, and 24.7% naltrexone. Interestingly, buprenorphine treatment was associated with a significantly reduced hazard ratio of 0.34, whereas this effect was equivocal for methadone treatment and not significant for naltrexone treatment. In her editorial, Dr. Larissa Mooney from UCLA points out the importance of extending this work to more diverse samples, discusses the reasons why buprenorphine may be more effective in reducing suicides, and underscores the need to implement suicide detection and prevention strategies in individuals with substance use disorders (8).
Relations Between Opiate Prescription Dispensing Rates With Prescription-Related Opiate Misuse and Heroin Use
Vuolo and Kelly (9) draw attention to the impact of opiate prescription rates on prescription-related opiate misuse and the development of prescription-related opiate dependence. The authors also examine the extent to which changes in opiate prescription rates are reflected by reciprocal changes in the use of heroin as there is some concern that a reduction in the availability of prescribed opiates could result in a shift to the use of illicit opiates. A unique aspect of this study is that the analyses are performed with county-level prescription data allowing the researchers to uncover, at the local level, how opiate prescriptions impact individuals. Opiate usage data from the National Survey on Drug Use from 2006 to 2016 from 748,800 participants were used along with opiate prescription data acquired from the Centers for Disease Control and Prevention covering the same time period. For the drug use survey, 70,000 participants are randomly selected each year and over the time period assessed the average county-level opiate dispensing rate endorsed by the participants across all years was 78.4%. Results from this data set revealed that 4.6% of surveyed individuals reported opiate misuse and 0.5% reported opiate dependence. Of those individuals reporting misuse, 0.5% endorsed regular but not daily misuse, whereas 0.3% reported daily misuse. When performing mathematical modeling and accounting for numerous relevant covariates, the researchers found significant relations between county-level opioid prescription rates and the odds of the occurrence of negative outcomes. Specifically, a one standard deviation increase in a county’s opiate prescribing level was estimated to be associated with a 7.2% increase in the odds of opioid misuse, a 3.5% increase in the odds of increased frequency of misuse, and a 10.4% increase in the odds of opiate dependence. No significant relation was found between changes in opiate prescription rates and changes in heroin use. Taken together, these findings provide additional data to support the value of reducing opiate prescription rates with the goal of reducing the misuse of prescribed opiates. The data also suggest that, at least in populations similar to that surveyed in this study, that a reduction in opiate prescribing will not be associated with an increase heroin use. In her editorial, Dr. Maree Teeson from the University of Sydney in Australia reminds us of the huge human toll that results from opiate abuse (10). She further discusses the need for taking measures that not only reduce the risk to misuse opiates but that also increase the ability to effectively treat individuals with opiate use disorders.
Conclusions
Taken together, the papers in this issue of the Journal illustrate the fundamental importance of integrating clinical and basic research approaches in the pursuit of a deeper understanding of psychiatric disorders. The clinical papers in this issue are focused on opiate misuse as well as on long-term outcomes in individuals with psychotic disorders. In relation to opiates, data are presented supporting an association between increased opiate prescribing patterns with an increased risk to engage in opiate misuse and to develop opiate use disorder. Notably, the data from this study also demonstrated that reductions in opiate prescribing were not accompanied by increases in the use of illicit opiates such as heroin. The other paper in this issue that is relevant to opiate use disorder demonstrates that stable medication treatment for opiate use disorder, especially with buprenorphine, is associated with a reduction in suicide risk. The findings from both of these papers are of obvious clinical importance and should reinforce providers to be mindful of the judicious use of opiates for pain control, the need to regularly assess suicidality in opioid use disorder patients, and the added value afforded by medication treatment for opioid use disorder in reducing suicidality.
Regarding psychotic disorders, the paper by O’Keefe et al. (5) demonstrates that prolonged durations of untreated psychosis are associated with poorer functional outcomes that are evident for up to 20 years after treatment of a first psychotic episode. These data reinforce the importance of early detection and intervention programs for individuals with psychotic illnesses, as well as the need to reduce barriers and enable access to treatment.
The basic research papers included in this issue take us to a deeper mechanistic level, providing insights into prefrontal cortical dysfunction that is relevant to patients with schizophrenia and other illnesses associated with cognitive impairments. The overview by Sohal (1) on prefrontal microcircuits is highly informative, presenting an in-depth discussion of the importance of cortical microcircuits in mediating neurophysiological processes that are critical to adaptive prefrontal executive and cognitive functions. The original research paper by Chung et al. (2) extends these concepts by demonstrating specific synaptic alterations in dlPFC neurons from individuals with schizophrenia that are characterized by increased variability in the strength of excitatory inputs onto parvalbumin interneurons. These papers are exemplars of the critical value that basic neuroscience research brings to, and is translatable to, psychiatry. Taken together, the clinical and basic research papers included in this issue highlight opportunities for future research aimed at developing new treatments and improving clinical care.
References
1.
Sohal VS: Transforming discoveries about cortical microcircuits and gamma oscillations into new treatments for cognitive deficits in schizophrenia. Am J Psychiatry 2022; 179:267–276
2.
Chung DW, Geramita MA, Lewis DA: Synaptic variability and cortical gamma oscillation power in schizophrenia. Am J Psychiatry 2022; 179:277–287
3.
Jonas KG, Fochtmann LJ, Perlman G, et al: Lead-time bias confounds association between duration of untreated psychosis and illness course in schizophrenia. Am J Psychiatry 2020; 177:327–334
4.
Goff DC, Li C, Thorpe L: Does early intervention improve the long-term course of schizophrenia? Am J Psychiatry 2020; 177:288–290
5.
O’Keeffe D, Kinsella A, Waddington JL, et al: 20-year prospective, sequential follow-up study of heterogeneity in associations of duration of untreated psychosis with symptoms, functioning, and quality of life following first-episode psychosis. Am J Psychiatry 2022; 179:288–297
6.
Malla A: Reducing duration of untreated psychosis: the neglected dimension of early intervention services. Am J Psychiatry 2022; 179:259–261
7.
Watts BV, Gottlieb DJ, Riblet NB, et al: Association of medication treatment for opioid use disorder with suicide mortality. Am J Psychiatry 2022; 179:298–304
8.
Mooney LJ: Medication treatment for opioid use disorder reduces suicide risk. Am J Psychiatry 2022; 179:262–263
9.
Vuolo M, Kelly BC: Effects of county-level opioid dispensing rates on individual-level patterns of prescription opioid and heroin consumption: evidence from national US data. Am J Psychiatry 2022; 179:305–311
10.
Teesson M: Opioid prescribing and the very human toll of drug harms. Am J Psychiatry 2022; 179:264–266
Information & Authors
Information
Published In

History
Received: 17 February 2022
Accepted: 22 February 2022
Published online: 1 April 2022
Published in print: April 2022
Keywords
Authors
Funding Information
Disclosures of Editors’ financial relationships appear in the April 2022 issue of the Journal.
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBFigures
Tables
Media
References
References
1.
Sohal VS: Transforming discoveries about cortical microcircuits and gamma oscillations into new treatments for cognitive deficits in schizophrenia. Am J Psychiatry 2022; 179:267–276
2.
Chung DW, Geramita MA, Lewis DA: Synaptic variability and cortical gamma oscillation power in schizophrenia. Am J Psychiatry 2022; 179:277–287
3.
Jonas KG, Fochtmann LJ, Perlman G, et al: Lead-time bias confounds association between duration of untreated psychosis and illness course in schizophrenia. Am J Psychiatry 2020; 177:327–334
4.
Goff DC, Li C, Thorpe L: Does early intervention improve the long-term course of schizophrenia? Am J Psychiatry 2020; 177:288–290
5.
O’Keeffe D, Kinsella A, Waddington JL, et al: 20-year prospective, sequential follow-up study of heterogeneity in associations of duration of untreated psychosis with symptoms, functioning, and quality of life following first-episode psychosis. Am J Psychiatry 2022; 179:288–297
6.
Malla A: Reducing duration of untreated psychosis: the neglected dimension of early intervention services. Am J Psychiatry 2022; 179:259–261
7.
Watts BV, Gottlieb DJ, Riblet NB, et al: Association of medication treatment for opioid use disorder with suicide mortality. Am J Psychiatry 2022; 179:298–304
8.
Mooney LJ: Medication treatment for opioid use disorder reduces suicide risk. Am J Psychiatry 2022; 179:262–263
9.
Vuolo M, Kelly BC: Effects of county-level opioid dispensing rates on individual-level patterns of prescription opioid and heroin consumption: evidence from national US data. Am J Psychiatry 2022; 179:305–311
10.
Teesson M: Opioid prescribing and the very human toll of drug harms. Am J Psychiatry 2022; 179:264–266