
The Incidence and Course of Depression in Bereaved Youth 21 Months After the Loss of a Parent to Suicide, Accident, or Sudden Natural Death
Abstract
Objective: This study examined effects of bereavement 21 months after a parent’s death, particularly death by suicide. Method: The participants were 176 offspring, ages 7–25, of parents who died by suicide, accident, or sudden natural death. They were assessed 9 and 21 months after the death, along with 168 nonbereaved subjects. Results: Major depression and alcohol or substance abuse 21 months after the parent’s death were more common among bereaved youth than among comparison subjects. Offspring with parental suicide or accidental death had higher rates of depression than comparison subjects; those with parental suicide had higher rates of alcohol or substance abuse. Youth with parental suicide had a higher incidence of depression than those bereaved by sudden natural death. Bereavement and a past history of depression increased depression risk in the 9 months following the death, which increased depression risk between 9 and 21 months. Losing a mother, blaming others, low self-esteem, negative coping, and complicated grief were associated with depression in the second year. Conclusions: Youth who lose a parent, especially through suicide, are vulnerable to depression and alcohol or substance abuse during the second year after the loss. Depression risk in the second year is mediated by the increased incidence of depression within the first 9 months. The most propitious time to prevent or attenuate depressive episodes in bereaved youth may be shortly after the parent’s death. Interventions that target complicated grief and blaming of others may also improve outcomes in symptomatic youth with parental bereavement.
Enduring psychiatric sequelae in children who have lost a parent have been demonstrated by retrospective, record-linkage, and prospective studies (1 – 3) . However, relatively little is known about the time, course, and causal pathways leading to disorders in parentally bereaved children. The delineation of predictors and temporal pathways to disorders and recovery could help to clarify the boundaries of normal versus pathological bereavement and to frame targets for effective intervention.
We have previously reported that children of parents who died of suicide, accidental death, or sudden natural death had higher rates of new-onset depression and posttraumatic stress disorder (PTSD) than nonbereaved comparison subjects during the first 9 months after the death, with no within-group differences attributable to cause of parental death (4) . Significant correlates of depression, the most common new-onset condition, were degree of impairment in the surviving parent, intercurrent life events, negative child coping, and child history of a psychiatric disorder before the death.
We now report on a 21-month follow-up of this cohort in order to describe the ongoing trajectory of disorders and symptoms in the bereaved youth relative to nonbereaved comparison subjects. We hypothesized that 1) at 21 months after the death, bereaved youth would continue to show a higher prevalence and symptom severity of depression and PTSD than nonbereaved comparison subjects, 2) during the second year of follow-up, youth whose parents died by suicide would show the highest prevalence and incidence of depression, 3) predictors of depression during follow-up would include worse caregiver functioning, stressful life events, negative coping, low social support, and prior history of depression, and 4) within the bereaved group, depression would be predicted by the preceding variables, in addition to parental suicide and high baseline levels of complicated grief.
Method
Study Group and Recruitment
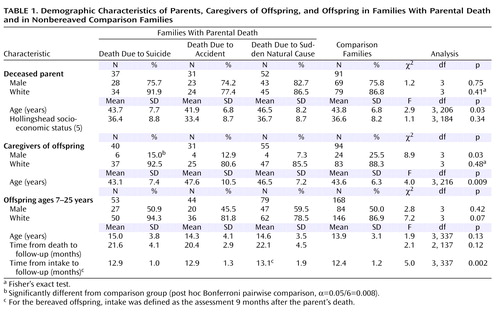
The participants were from 120 parentally bereaved families and 91 nonbereaved families, which comprised 83.1% of the 239 families described previously and an additional 15 families recruited subsequently (4) . The deceased probands were between the ages of 30 and 60 years, had biological offspring between the ages of 7 and 25, and had died within 24 hours of the precipitating event from suicide, an accident, or sudden natural cause. Families in which there were multiple deaths or injuries were excluded. The accidental deaths consisted of 12 motor vehicle accidents, 11 drug overdoses, three falls, and five other causes (e.g., drowning, exposure to cold). At intake the drug overdoses were carefully reviewed to rule out subjects with possible suicidal intent, and those probands had a much lower rate of previous suicide attempt (none of 11, or 0.0%) than did suicide victims (11 of 37, or 29.7%) (p=0.03, Fisher’s exact test). The sudden natural deaths were due to myocardial infarction (N=37), infections (N=5), and 10 less frequent causes (e.g., diabetes, stroke, aneurysm, gastric bypass surgery). In the bereaved families, the caretaking parent was almost always female (112 of 120, or 93.3%) and offspring in bereaved families were almost always the biological offspring of the caretaking parent (151 of 176, or 85.8%). The nonbereaved offspring had two living biological parents, lived in the home of at least one of them, and had no first-degree relatives who had died within the previous 2 years. Four offspring from two comparison families who experienced the loss of a parent during the follow-up period were excluded from these analyses.
Bereaved families were recruited through coroner’s reports and newspaper advertisements, and 71% of the potential subjects participated (4) . The demographic characteristics of the enrolled probands were similar to those for all people who had died by suicide or accident. The accident and suicide probands in the families recruited by advertisement and those recruited from the coroner’s office were similar with respect to method of death and demographic variables. Because people who die from sudden natural causes are not under the coroner’s jurisdiction, the representativeness of this proband group cannot be assessed. The comparison probands were frequency matched to the deceased parents by neighborhood, age, and gender, and they were recruited either by random-digit dialing or by newspaper advertisement, with an overall acceptance rate of 55% (4) . This study was approved by the University of Pittsburgh institutional review board, and all participants gave written consent or assent.
A total of 401 bereaved and nonbereaved youth were available for follow-up, of whom 344 (85.8%) were interviewed ( Table 1 ). Those retained in the study were similar to those who were lost, except that the caregivers who were retained had higher levels of functioning at baseline according to the Global Assessment Scale (GAS) (6) (mean=78.4, SD=11.0, versus mean=71.1, SD=14.4; t=3.8, df=35.9, p=0.008) and were more likely to be Caucasian (85.1% versus 70.3%; χ 2 =5.34, df=1, p=0.02). Group comparisons showed similarities among probands, caregivers, and offspring, except that the caregivers of children whose parent committed suicide were more likely to be female than were the caregivers of the comparison children and that the length of follow-up was about 3 weeks longer in the group with sudden natural parental death than in the comparison group.
Assessment
The participants were interviewed at two points in time, first around 9 months after the death, as previously reported, and then around 1 year later, i.e., 21 months after the death (4) . The latter assessments were timed to avoid conducting an interview on the second-year anniversary of the parent’s death. Socioeconomic status and household income were rated by using Hollingshead’s scale (5) . Psychiatric disorders in offspring younger than 18 were assessed by using the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (7) , and for adult offspring and caregivers, the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) was used (8) . Psychiatric assessment of the proband was conducted by using a psychological autopsy procedure (9) and the SCID-I (8) . The course of disorders in offspring was documented by using the Longitudinal Interview for Follow-Up Evaluations (10) or the adolescent version. Functional status was determined by using the Children’s Global Assessment Scale (11) or the GAS for adults (6) . High interrater reliability was maintained on psychiatric diagnoses and global impairment, as indicated by kappa values of 0.74–0.85 and an intraclass correlation coefficient of 0.88.
The Circumstances of Exposure to Death, a semistructured interview, was used to assess the offspring’s experience surrounding and following the death of the parent (12) . A 28-item version of the Inventory of Complicated Grief modified for children and adolescents was used to assess complicated grief (13) , and the adult version was used for adult offspring (14) .
Severity of depression, anxiety, PTSD, and suicidal ideation was assessed in the offspring by using the Mood and Feelings Questionnaire (15) , the Screen for Child Anxiety-Related Emotional Disorders (16) , the Child PTSD Symptom Scale Interview (17) , and the Suicidal Ideation Questionnaire-JR (18) . Parallel measures in adults were obtained by using the Beck Depression Inventory (19) , the Beck Anxiety Inventory (20) , the PTSD Symptom Scale Interview (21) , and the Suicidal Ideation Questionnaire (22) . Intercurrent life events were assessed by using the Life Events Checklist (23) and a shortened version of the Holmes-Rahe Social Readjustment Rating Scale (24) , in offspring under and over 18, respectively.
Family cohesion, social support, coping, and self-esteem in youth were assessed by means of the Family Adaptability and Cohesion Evaluation Scales-II (25) , the Survey of Children’s Social Support (26) , the Kidcope (27) , and the self-esteem subscale of the Weinberger Adjustment Inventory (unpublished 1987 work of Weinberger et al.), respectively. Social support and coping were assessed in adult offspring by using the Multidimensional Scale of Perceived Social Support (28) and the Ways of Coping questionnaire (29) , respectively.
Data Analyses
We compared the bereaved and comparison groups on rates of current disorders by using either the chi-square statistic or Fisher’s exact test. Difference in the severity of a disorder was examined with analysis of variance. When different measures for the same domains were used for adults and children, the data were z-transformed. Unless stated otherwise, df=1. Bonferroni’s correction for multiple contrasts was used as follows: for current psychiatric disorders, with seven categories, α=0.05/7=0.007; for current symptoms, with six measures each, α=0.05/6=0.008. Post hoc pairwise contrasts among the four groups overall and among the three bereaved groups were also protected for the number of contrasts (α=0.05/6=0.008 and α=0.05/3=0.017, respectively).
The cumulative incidence of depression was compared in the four groups by using Kaplan-Meier survival analysis. The correlates of depression occurring between 9 and 21 months were examined by means of standard parametric univariate statistics. Logistic regression, after application of appropriate data imputations, was used to identify the most parsimonious set of variables that predicted depression occurring during the 9–21-month follow-up period. We included a clustering term since multiple offspring from the same family often participated. In this study group, only 10% of the participants had missing data for more than four variables that were significantly associated with follow-up depression; thus, the missing-at-random assumption is reasonable. For statistical analyses with missing data, we used the general approach of Little and Rubin (30) , applying multiple imputation by chained equations (MICE), implemented in STATA version 10.0 (Stata Corp, College Station, Tex.), which makes use of auxiliary variables that are correlates of being missing and/or the variables of interest (31) . Finally, path analyses were conducted by using MPlus version 4.1 (Muthén & Muthén, Los Angeles), beginning with the variables selected by logistic regression to identify possible causal pathways between bereavement and subsequent depression in offspring (32) .
Results
Diagnoses and Symptoms 21 Months After Parent’s Death
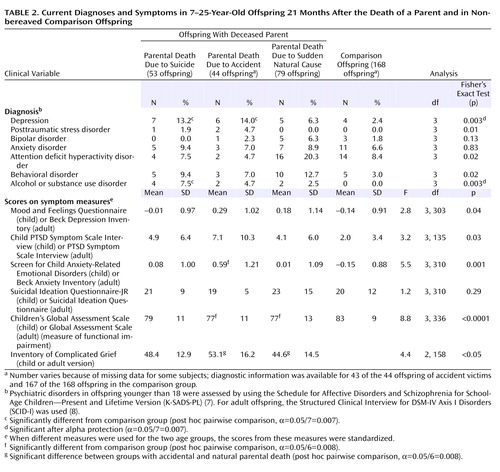
In relation to the nonbereaved comparison group, the total group of bereaved offspring had higher rates of major depression (10.2% versus 2.4%; p<0.007, Fisher’s exact test) and alcohol or substance abuse (4.5% versus 0.0%; p=0.008, Fisher’s exact test). As shown in Table 2 , post hoc contrasts showed that the offspring of parents who died by suicide and offspring of those who died in accidents showed higher rates of major depression than did the comparison subjects, and the children of suicide victims showed a higher rate of alcohol or substance abuse disorders than did the comparison subjects. Overall differences were found for severity of anxiety symptoms and level of functioning ( Table 2 ). Post hoc comparisons showed that anxiety was higher in youth whose parents died through accidents than in the comparison subjects and functional impairment was greater in the offspring of parents who died by accidents or by sudden natural death than in the comparison subjects. There were also group differences with respect to scores for complicated grief; the post hoc contrasts indicated that the level of complicated grief was higher in youth whose parents died through accidents than in those whose parents died by sudden natural death.
Cumulative Incidence and Course of Depression
The incidence rate ratio for depression was greater in the bereaved than in the comparison offspring; the incidence rate ratio was 2.7, with a 95% confidence interval (CI) of 1.6 to 4.8. There were significant differences between each of the three bereaved groups and the comparison subjects (incidence rate ratios, 2.1–3.4) but with no significant differences among the three bereaved groups ( Figure 1 ). Bereavement had a strong effect on the incidence of depression in the 9 months following the parent’s death (23.9% versus 5.4%; χ 2 =23.3, df=1, p<0.0001) but not during the subsequent year (8.5% versus 7.1%; p=0.69, Fisher’s exact test). The post hoc contrasts showed that the rate of incident depression between the 9- and 21-month assessments was higher in the offspring who lost a parent to suicide (nine of 53, 17.0%) than in those whose parents died by sudden natural death (two of 79, 2.5%) (p=0.007, Fisher’s exact test). The rates of depression remission observed in those who became depressed during the first 9 months after the death were similar in the bereaved (30 of 42, 71.4%) and comparison (six of nine, 66.7%) groups (p=1.00, Fisher’s exact test).

a Significant differences among groups (Wilcoxon and log-rank tests for equality of survivor functions: χ 2 =17.4, df=3, p=0.0006).
Cumulative Incidence and Course of PTSD
The incidence of PTSD was higher in the bereaved group than in the comparison group during the first 9 months after the death (8.5% versus 0.0%; p<0.0001, Fisher’s exact test) but not during the second year of follow-up (2.8% versus 0.0%; p=0.06, Fisher’s exact test). Of the 15 individuals with incident PTSD within 9 months of the death, all but one experienced a remission. During the second year, two of the five who experienced incident PTSD had remissions.
Correlates of Depressive Episode During Second Follow-Up Year
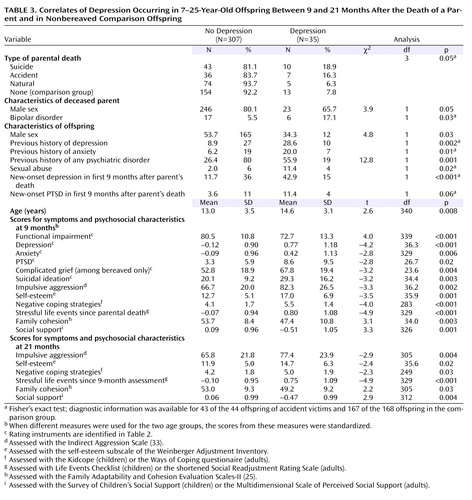
At some point during the second year of observation (from 9 to 21 months after the death), 35 offspring had a depressive episode, 22 bereaved youth and 13 comparison subjects. These depressive episodes (“follow-up depression”) included both those that were ongoing from the time of the 9-month assessment (N=8) as well as those that were incident during this time interval (N=27). Correlates of follow-up depression were female gender, older age, a previous history of anxiety or depression, and a history of sexual abuse ( Table 3 ). Characteristics assessed at the 9-month assessment that were associated with follow-up depression were greater functional impairment; higher levels of self-reported depression, anxiety, PTSD, suicidal ideation, and impulsive aggression; negative coping; greater number of stressful life events; lower family cohesion; and lower perceived social support. Many of these same variables assessed at the 21-month follow-up were also associated with a depressive episode during the follow-up period. Having had an episode of depression during the first 9 months was predictive of depression in the following year. Depression at 21 months was more likely to be a persistence or recurrence from the first observation period in the bereaved group (12 of 176, 6.8%) than in the nonbereaved offspring (three of 168, 1.8%) (p=0.03, Fisher’s exact test).
The best-fitting, most parsimonious model that predicted the occurrence of depression between 9 and 21 months included previous history of a depressive episode (odds ratio=8.6, 95% CI=1.7 to 43.8), self-reported anxiety at 9 months (odds ratio=1.6, 95% CI=1.1 to 2.4), and negative life events at 9 months (odds ratio=1.9, 95% CI=1.2 to 2.9) and 21 months (odds ratio=1.7, 95% CI=1.2 to 2.5). Compared to the other bereaved and nonbereaved groups, the offspring of parents who died sudden natural deaths had a lower risk of depression (odds ratio=0.01, 95% CI=6×10 –5 to 0.99). There was an interaction between bereavement and previous history of depression, meaning that a previous history of depression conveyed an even greater risk for subsequent depression in the nonbereaved group (odds ratio=23.5, 95% CI=1.6 to 350.7). In this regression, the diagnosis of bipolar disorder in the proband, which was an important correlate of incident depression within the first 9 months after parental loss, was associated with a threefold (odds ration=3.15, 95% CI=0.98 to 10.2) increased risk of depression, although it was not statistically significant (p=0.06).
Within the bereaved group, depression between 9 and 21 months was associated with the loss of a mother rather than a father (41.9% versus 13.7%; p=0.004, Fisher’s exact test) and a previous history of any psychiatric disorder (57.1% versus 32.9%; χ 2 =4.7, df=1, p=0.03). The risk of follow-up depression tended to be higher in those whose parent died by suicide than in those with parental bereavement due to natural death (18.9% versus 1.3%) (p=0.05, Fisher’s exact test). Higher scores for complicated grief at 9 months and lower self-esteem scores (mean=13.0, SD=5.1, versus mean=18.6, SD=7.0; t=–3.5, df=21.8, p=0.002) were associated with subsequent depression, as were a similar set of measures of self-reported symptoms and psychosocial characteristics at both 9 and 21 months, as noted already. Those who developed depression in the first 9 months after the death were more likely to have an incident depressive episode between 9 and 21 months (54.5%) than were those without depression in the first 9 months (19.6%) (χ 2 =12.9, df=1, p<0.001). Those with PTSD during the first 9 months were also more likely to develop depression during the next assessment period (18.2% versus 5.2%; p=0.05, Fisher’s exact test). Risk for depression during the second year of follow-up was also higher among bereaved offspring whose last conversation with the deceased was discordant (26.3% versus 6.1%; p=0.02, Fisher’s exact test) or who felt that others were accountable for the death (47.6% versus 21.6%; χ 2 =6.6, df=1, p=0.01).
Logistic regression identified the following as the most parsimonious, best-fitting set of predictors of depression among bereaved offspring between 9 and 21 months: baseline low self-esteem (odds ratio=1.16, 95% CI=1.05 to 1.28) and high negative coping (odds ratio=1.34, 95% CI=1.03 to 1.75) at 9 months. With the two variables in the model, parental bereavement through suicide was, as predicted, associated with a higher risk for depression between the two assessments, relative to accidents (odds ratio=2.9, 95% CI=0.83 to 10.0) and sudden natural death (odds ratio=3.5, 95% CI=0.95 to 12.8), but these findings escaped statistical significance.
Path Analysis
A good-fitting path model predicting depression between 9 and 21 months was developed by using variables selected by logistic regression (chi-square test of model fit=10.4, df=8, p=0.24; comparative fit index=0.98; Tucker-Lewis index=0.96; root mean square residual=0.03; weighted root mean square residual=0.58). In this model, bereavement had an indirect effect on depression at 21 months, mediated by the relationship between bereavement and incident depression within the first 9 months of depression ( Figure 2 ). A previous history of depression, antedating the period of observation, was related to depression at 21 months through two pathways: 1) history of depression was related to negative life events, which in turn increased the risk of depression between 9 and 21 months, and 2) history of depression was related to a higher score for self-reported anxiety symptoms at 9 months, which was associated with incident depression at 9 months, which then increased the risk for depression during the subsequent year.
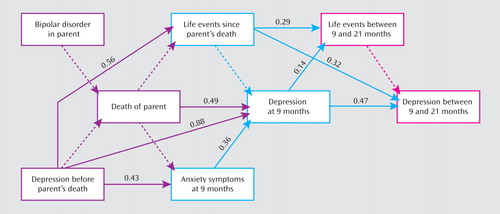
a Numbers are standardized path coefficients. Solid lines indicate statistically significant paths. Dotted lines indicate pathways that are not significant.
Discussion
In this longitudinal study, there were enduring effects of parental bereavement on the offspring, with higher rates of depression and alcohol or substance abuse, greater functional impairment, and higher self-reported anxiety nearly 2 years after the loss. Bereavement by accident and by suicide were associated with higher risks of depression than seen in nonbereaved comparison subjects; suicide-related bereavement was also associated with alcohol or substance abuse, and accident-related bereavement was also related to higher symptom levels. The direct effect of bereavement on incident depression and PTSD was limited to the first 9 months after the loss, except in the offspring of parents who died by suicide, who continued to have a higher incidence of depression than offspring whose parents had sudden natural deaths. During the second year of follow-up, the effect of bereavement on depression was mediated by the occurrence of new-onset depression during the first 9 months postbereavement. Within the bereaved group, depression at 21-month follow-up was predicted by parental suicide, loss of a mother, postbereavement depression, complicated grief, negative coping, low self-esteem, and blaming others for the death.
These results should be considered within the context of the strengths and limitations of this study. This is one of the largest population-based longitudinal studies of the impact of parental bereavement on children, and it is one of the few to examine the specific effects on offspring of parental death by suicide. Despite the study’s relative size, contrasts among the different causes of death can detect only relatively large effects. Also, the study group is mostly Caucasian and does not include parental homicide, thereby limiting the generalizability of these findings.
Nearly 2 years after the death, bereaved youth showed higher rates of depression and alcohol or substance abuse than comparison subjects, higher self-rated anxiety, and greater functional impairment. The main effect of bereavement on both incident depression and PTSD occurred shortly after the death, as has been reported in other studies of adolescent bereavement (12 , 34) . However, bereavement had an indirect effect on depression during the second year of follow-up, by increasing the risk of incident depression within 9 months of the loss, which increased the likelihood of depression during the next year. This pathway is attributable in part to the persistence and recurrence of these incident episodes of depression occurring shortly after the loss in the bereaved group.
Prior history of depression was related to depressive outcome at 21-month follow-up through two pathways. First, a history of depression was associated with an increased risk of negative life events, which then increased the risk of subsequent depression. Second, a history of depression was related to anxiety at 9 months, which was associated with incident depression during the first 9 months; depression in the first 9 months increased the risk of incident depression between 9 and 21 months. While a prior history of depression predicted depression at 21 months among the bereaved, it was an even stronger predictor of subsequent depression in the nonbereaved comparison subjects, which contrasts with findings in some other studies of adolescent bereavement (12) .
As hypothesized, offspring of parents who died by suicide showed higher rates of current and incident depression from 9 to 21 months after the death, in relation to the comparison subjects and the offspring of parents who died by sudden natural death, respectively. Offspring of the suicide group also showed a higher rate of alcohol or substance abuse. However, all deleterious effects of bereavement were not attributable to suicide. Offspring of parents who died through accidents also showed higher rates of depression than comparison subjects at 21 months, had the highest scores on self-reported anxiety and complicated grief, and were more functionally impaired. Other studies have shown either no difference between youth whose parents died by suicide and those whose parents died of other causes (35) or more behavioral or anxiety symptoms, but not depression (36) .
The pathways and predictors of depression in this study group suggest that there may be a window of opportunity shortly after a parent’s death in which to prevent or attenuate further depressive episodes in bereaved youth. This is because the effect of bereavement on depression 21 months after the death is mediated by the occurrence of depression in the 9 months after the death. Previous intervention studies have not found a critical period during which the intervention is more effective, but these studies did not have data about prior course for participants enrolled longer after the death (37) . However, our previous (4) and current findings are convergent with the prevention studies of Sandler and colleagues, who have identified the critical roles of coping, self-esteem, negative life events, family cohesion, and social support in mediating long-term outcome for parentally bereaved youth (37) .
Within the bereaved group, we found that the loss of a mother was more deleterious than the loss of a father. Although this finding did not survive multivariate analyses, it is consistent with other reports (38 , 39) . Bereaved youth who had high levels of complicated grief and those who blamed others for the death were at particularly high risk for depression at the 21-month follow-up. This finding is consistent with studies in adults showing prolonged time to recovery from depression in those with complicated grief, and it provides additional support for the existence of complicated grief in children and adolescents (14 , 40) . Interventions that target complicated grief and the placement of blame for the death on others may be useful in managing symptomatic and impaired parentally bereaved youth.
In conclusion, we have shown that there are enduring effects of parental bereavement, especially with regard to the occurrence of depression during the second year of follow-up. The offspring of parents who died by suicide showed the highest risk for subsequent depression. Since the effects of bereavement on depression in the second year were mediated by the increased risk of depression occurring shortly after the death, the best time to intervene to prevent further depression episodes may be shortly after the loss. Further follow-up of this cohort should help to address the validity and impact of complicated grief and whether individuals with a parent who dies by suicide do indeed suffer more long-term sequelae, compared to other bereaved youth.
1. Tremblay GC, Israel AC: Children’s adjustment to parental death. Clin Psychol Sci Prac 1998; 5:424–438Google Scholar
2. Dowdney L: Childhood bereavement following parental death. J Child Psychol Psychiatry 2000; 41:819–830Google Scholar
3. Kendler KS, Sheth K, Gardner CO, Prescott CA: Childhood parental loss and risk for first-onset of major depression and alcohol dependence: the time-decay of risk and sex differences. Psychol Med 2002; 32:1187–1194Google Scholar
4. Melhem N, Walker M, Moritz G, Brent DA: Antecedents and sequelae of sudden parental death in offspring and surviving caregivers. Arch Pediatr Adolesc Med 2008; 162:403–410Google Scholar
5. Hollingshead AB: Four-Factor Index of Social Status. New Haven, Conn, Yale University, Department of Sociology, 1975Google Scholar
6. Endicott J, Spitzer RL, Fleiss JL, Cohen J: The Global Assessment Scale: a procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry 1976; 33:766–771Google Scholar
7. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N: Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 1997; 36:980–988Google Scholar
8. First MB, Spitzer RL, Gibbon M, Williams JBW: Structured Clinical Interview for DSM-IV Axis I Disorders (SCID). New York, New York State Psychiatric Institute, Biometrics Research, 1996Google Scholar
9. Hawton K, Appleby L, Platt S, Foster T, Cooper J, Malmberg A, Simkin S: The psychological autopsy approach to studying suicide: a review of methodological issues. J Affect Disord 1998; 50:269–276Google Scholar
10. Keller MB, Lavori PW, Friedman B, Nielsen E, Endicott J, McDonald-Scott P, Andreasen NC: The Longitudinal Interval Follow-Up Evaluation: a comprehensive method for outcome in prospective longitudinal studies. Arch Gen Psychiatry 1987; 44:540–548Google Scholar
11. Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H: A Children’s Global Assessment Scale (C-GAS). Arch Gen Psychiatry 1983; 40:1228–1231Google Scholar
12. Brent DA, Perper JA, Moritz G, Allman C, Schweers J, Roth C, Balach L, Conobbio R, Liotus L: Psychiatric sequelae to the loss of an adolescent to suicide. J Am Acad Child Adolesc Psychiatry 1993; 32:509–517Google Scholar
13. Melhem NM, Moritz G, Walker M, Shear MK, Brent D: Phenomenology and correlates of complicated grief in children and adolescents. J Am Acad Child Adolesc Psychiatry 2007; 46:493–499Google Scholar
14. Prigerson HG, Jacobs SC: Traumatic grief as a distinct disorder: a rationale, consensus criteria, and a preliminary empirical test, in Handbook of Bereavement Research: Consequences, Coping, and Care. Edited by Stroebe MS, Hansson RO, Stroebe W, Schut HAW. Washington, DC, American Psychological Association, 2001, pp 613–647Google Scholar
15. Messer SC, Angold A, Costello EJ, Loeber R, van Kammen W, Stouthamer-Loeber M: Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents: factor composition and structure across development. Int J Methods Psychiatr Res 1995; 5:251–262Google Scholar
16. Khetarpal-Monga S, Birmaher B, Chiappetta L, Brent DA, Kaufman J, Bridge J, Cully M: The Screen for Child Anxiety-Related Emotional Disorders (SCARED): convergent and divergent validity. Depress Anxiety 2000; 12:85–91Google Scholar
17. Foa EB, Johnson KM, Feeny N, Treadwell KR: The Child PTSD Symptom Scale: a preliminary examination of its psychometric properties. J Clin Child Psychol 2001; 30:376–384Google Scholar
18. Reynolds WM, Mazza JJ: Assessment of suicidal ideation in inner-city children and young adolescents: reliability and validity of the Suicidal Ideation Questionnaire-JR. School Psych Rev 1999; 28:17–30Google Scholar
19. Beck AT, Steer RA, Garbin MG: Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin Psychol Rev 1988; 8:77–100Google Scholar
20. Beck AT, Brown G, Epstein N, Steer RA: An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 1988; 56:893–897Google Scholar
21. Foa E, Johnson KM, Feeny NC: Reliability and validity of a brief instrument for assessing post traumatic stress disorder. J Trauma Stress 1993; 6:459–473Google Scholar
22. Reynolds WM: Suicidal Ideation Questionnaire: Professional Manual. Odessa, Fla, Psychological Assessment Resources, 1988Google Scholar
23. Brand AH, Johnson JH: Note on reliability of the Life Events Checklist. Psychol Rep 1982; 50:1274Google Scholar
24. Lewinsohn PM, Rohde P, Seeley JR, Fischer SA: Age and depression: unique and shared effects. Psychol Aging 1991; 6:247–260Google Scholar
25. Olsen DH, Portner J, Lavee Y: Family Adaptability and Cohesion Evaluation Scales (FACES-II). Minneapolis, University of Minnesota Press, 1985Google Scholar
26. Dubow EF, Ullman DG: Assessing social support in elementary school children: the Survey of Children’s Social Support. J Clin Child Psychol 1989; 18:52–64Google Scholar
27. Spirito A, Stark LJ, Williams C: Development of a brief coping checklist for use with pediatric populations. J Pediatr Psychol 1988; 13:555–574Google Scholar
28. Zimet GD, Dahlem NW, Zimet SG, Farley GK: The Multidimensional Scale of Perceived Social Support. J Pers Assess 1988; 52:30–41Google Scholar
29. Lazarus RS: Coping theory and research: past, present, and future. Psychosom Med 1993; 55:234–247Google Scholar
30. Little RJA, Rubin DB: Statistical Analysis With Missing Data. New York, Wiley, 1987Google Scholar
31. Collins L, Schafer JL, Kam CM: A comparison of inclusive and restrictive strategies in modern missing data procedures. Psychol Methods 2001; 6:330–351Google Scholar
32. Muthén B, Shedden K: Finite mixture modeling with mixture outcomes using the EM algorithm. Biometrics 1999; 55:463–469Google Scholar
33. Buss AH, Perry M: The Aggression Questionaire. J Pers Soc Psychol 1992; 63:452–459Google Scholar
34. Bridge J, Day NL, Day RM, Richardson GA, Birmaher B, Brent DA: Major depressive disorder in adolescents exposed to a friend’s suicide. J Am Acad Child Adolesc Psychiatry 2003; 42:1294–1300Google Scholar
35. Brown AC, Sandler IN, Tein JY, Liu X, Haine RA: Implications of parental suicide and violent death for promotion of resilience of parentally bereaved children. Death Studies 2007; 31:301–305Google Scholar
36. Cerel J, Fristad MA, Weller EB, Weller RA: Suicide-bereaved children and adolescents: a controlled longitudinal examination. J Am Acad Child Adolesc Psychiatry 1999; 38:672–679Google Scholar
37. Sandler IN, Ayers TS, Wolchik SA, Tein J-Y, Kwok O-M, Haine RA, Twohey-Jacobs J, Suter J, Lin K, Padgett-Jones S, Weyer JL, Cole E, Kriege G, Griffin W: The Family Bereavement Program: efficacy evaluation of a theory-based prevention program for parentally bereaved children and adolescents. J Consult Clin Psychol 2003; 71:587–600Google Scholar
38. Agerbo E, Nordentoft M, Mortensen PB: Familial, psychiatric, and socioeconomic risk factors for suicide in young people: nested case-controlled study. Br Med J 2002; 32:574–577Google Scholar
39. Reinherz HZ, Giaconia RM, Carmola Hauf AM, Wasserman MS, Silverman AB: Major depression in the transition to adulthood: risks and impairments. J Abnorm Psychol 1999; 108:500–510Google Scholar
40. Melhem NM, Day N, Shear MK, Day R, Reynolds III CF, Brent DA: Predictors of complicated grief among adolescents exposed to a peer’s suicide. Journal of Loss and Trauma 2004; 9:21–33Google Scholar

