
In This Issue
Viewing Other-Race Faces in Schizophrenia
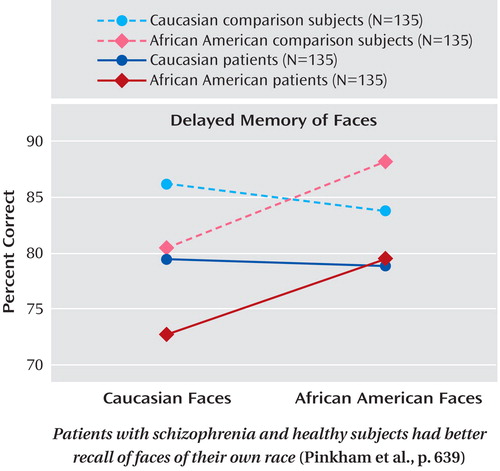
Demonstration that race influences facial processing by patients with schizophrenia challenges earlier findings of greater impairment in non-Caucasian patients viewing only Caucasian faces. Pinkham et al. (p. Original article: 639 ) report that 270 patients had poorer performance than healthy subjects on face recall and emotion recognition, but both groups showed less accuracy when the participant’s race differed from the race in the facial image being viewed. The similarity of the "other-race effect" in patients and healthy subjects suggests a normal aspect of development in individuals with schizophrenia and a need to recognize this influence in neurocognitive testing. Discussion is provided by Dr. Carl Bell in an editorial on p. Original article: 560 .
The Most Cost-Effective Treatment for Depressed Adolescents
The ratio of marginal cost to clinical improvement over 12 weeks was lower for fluoxetine than for cognitive-behavioral therapy (CBT), combined fluoxetine and CBT, or placebo among 369 adolescents with major depressive disorder. Earlier findings from the Treatment for Adolescents With Depression Study (TADS) showed significant symptom improvement with fluoxetine and even more with combination treatment. Domino et al. (CME, p. Original article: 588 ) related those results to monetary and time costs, including time and travel costs for adults providing transportation to treatment sessions. The total cost associated with fluoxetine treatment was only slightly more than for placebo. Combination treatment had the highest total cost but the greatest symptom reduction. Dr. Grayson Norquist examines treatment issues in an editorial on p. Original article: 549 .
ADHD Medication and Later Substance Abuse
Two long-term studies demonstrate that stimulant treatment of attention deficit hyperactivity disorder (ADHD) in young children does not increase the risk of substance abuse in early adulthood. Biederman et al. (p. Original article: 597 ) conducted a 10-year follow-up of boys with ADHD; 42 were treated with stimulants, and 39 were not. In early adulthood, the two groups showed no significant differences in the rates of alcohol use disorders, nicotine dependence, or other substance-related disorders. However, the duration of alcohol abuse was longer for those who had received stimulants for ADHD. Mannuzza et al. (p. Original article: 604 ) also performed a prospective follow-up, tracking 176 boys treated with methylphenidate for ADHD. The rates of nonalcohol substance use disorders in adulthood were similar in those who had begun taking methylphenidate at age 6 or 7 (27%) and in healthy comparison subjects (29%), but the rate was higher in those who started taking methylphenidate at ages 8–12 (44%). The association between age at first treatment and later substance abuse was accounted for by the development of antisocial personality disorder. Drs. Nora Volkow and James Swanson discuss ADHD and substance abuse in an editorial on p. Original article: 553 .
Mentalization Strategy Improves Outcome for Borderline Personality Disorder
Five years after the end of treatment, results were markedly better for 22 patients with borderline personality disorder in a multifaceted program focusing on the patient’s s mental state than for 19 who received standard treatment. The mentalization-based treatment included partial hospitalization, individualized medication, and psychoanalytically oriented psychotherapy. During follow-up, suicide was attempted by 23% of the patients in the experimental group but 74% of the control group. Bateman and Fonagy (p. Original article: 631 ) found numerous other differences favoring mentalization-based treatment in use of services and medication, global functioning, and vocational status. Although the 18-month partial hospitalization program was followed by 18 months of outpatient group treatment, service use was greater only during the first period, and it was significantly less throughout follow-up. Dr. Kenneth Levy considers these findings in an editorial on p. Original article: 556 .

