
A Multidimensional Meta-Analysis of Psychotherapy for PTSD
Abstract
OBJECTIVE: The authors present a multidimensional meta-analysis of studies published between 1980 and 2003 on psychotherapy for PTSD. METHOD: Data on variables not previously meta-analyzed such as inclusion and exclusion criteria and rates, recovery and improvement rates, and follow-up data were examined. RESULTS: Results suggest that psychotherapy for PTSD leads to a large initial improvement from baseline. More than half of patients who complete treatment with various forms of cognitive behavior therapy or eye movement desensitization and reprocessing improve. Reporting of metrics other than effect size provides a somewhat more nuanced account of outcome and generalizability. CONCLUSIONS: The majority of patients treated with psychotherapy for PTSD in randomized trials recover or improve, rendering these approaches some of the most effective psychosocial treatments devised to date. Several caveats, however, are important in applying these findings to patients treated in the community. Exclusion criteria and failure to address polysymptomatic presentations render generalizability to the population of PTSD patients indeterminate. The majority of patients posttreatment continue to have substantial residual symptoms, and follow-up data beyond very brief intervals have been largely absent. Future research intended to generalize to patients in practice should avoid exclusion criteria other than those a sensible clinician would impose in practice (e.g., schizophrenia), should avoid wait-list and other relatively inert control conditions, and should follow patients through at least 2 years.
Posttraumatic stress disorder (PTSD) is one of the most prevalent axis I disorders (1) for which psychotherapy is widely practiced. The psychotherapy research literature has focused primarily on cognitive behavior therapy approaches (particularly exposure and cognitive restructuring) and eye movement desensitization and reprocessing. Exposure therapy includes confrontation of memories of the trauma or cues (“triggers”) related to the traumatic event. Other cognitive behavior therapy approaches focus on developing skills for anxiety management or challenging distorted cognitions. Another treatment approach is eye movement desensitization and reprocessing (2), in which the patient is asked to develop a mental image of a traumatic event and related negative cognitions while tracking a bilateral stimulus. The mechanisms of action are largely unknown, although likely possibilities include exposure, other cognitive behavior therapy-like interventions (e.g., choosing and altering a negative belief about the self), and accessing of associative networks as in psychodynamic psychotherapy (3, 4). Reviews and meta-analyses have supported the efficacy of psychotherapy for PTSD, particularly cognitive behavior therapy and, more recently, eye movement desensitization and reprocessing (5–9). Although case studies have suggested the potential utility of other therapeutic approaches, such as psychodynamic and humanistic/experiential psychotherapy, research is not available to draw strong conclusions.
Although the short-term treatments tested in clinical trials (primarily cognitive behavior therapy) are clearly effective in reducing PTSD symptoms, research has yet to delineate clearly which patients are most likely to respond. Research on prognostic factors is limited, with different studies often finding different predictors (10–14). Of particular interest from a clinical standpoint is comorbidity, which is the rule rather than the exception in PTSD. Studying PTSD in an urban population, Breslau and colleagues (15) reported that 83% of individuals with PTSD met criteria for one or more other disorders. The most common comorbid conditions include depression, substance abuse, and other anxiety disorders (1, 15). Patients with PTSD are also frequently comorbid for axis II disorders and vice versa. For example, Yen et al. (16) found a 35% lifetime prevalence of PTSD among patients with personality disorders who reported any traumatic event and also found an association between severity of traumatic exposure and severity of personality disorder. Despite these high rates of comorbidity, empirical research addressing treatment effectiveness for patients presenting with specific patterns of comorbidity is sparse.
Goal of This Study
In this study we present a multidimensional meta-analysis (17, 18) of data from controlled trials of psychotherapy for PTSD, with the goal of describing a range of indices that bear on efficacy and generalizability, many of which have not previously been subjected to meta-analytic aggregation. A multidimensional meta-analysis presents, in addition to effect size, a range of statistics bearing on clinical utility and external validity that can be important in assessing the strengths and limitations of treatments of psychiatric disorders but are generally omitted from meta-analytic assessments of treatments. First, although most treatment studies attempt to maximize internal validity through their screening processes and inclusion/exclusion criteria, these decisions can affect external validity or generalizability. Thus, we aggregated data on both inclusion/exclusion criteria and patient exclusion rates. Second, no single index of outcome provides a comprehensive description of the effects of a treatment; a more nuanced portrait may require presentation of multiple metrics. Although effect size provides a crucial index of the effect an average patient can expect to achieve, it does not yield information on response variability, notably the proportion of patients who recover or experience clinically significant improvement. Thus, in addition to effect size, two additional indices are included in this meta-analysis: recovery rate and improvement rate. In calculating improvement and recovery rates, however, of particular importance is the denominator one chooses, i.e., the proportion improved or recovered out of what group of patients? The most liberal estimate uses as the denominator the number of study completers, eliminating patients who dropped out of treatment. A more conservative estimate uses the number of patients who actually began treatment (i.e., the intent-to-treat study group). Neither metric is more definitive than the other; consumers of research can draw the most accurate conclusions if researchers report both completer and intent-to-treat analyses (19). Because the completer/intent-to-treat distinction is orthogonal to the distinction between recovery and clinically significant improvement, we present four metrics: recovery rate among study completers, recovery rate for the intent-to-treat study group, improvement rate among study completers, and improvement rate for the intent-to-treat study group. Another variable that bears on efficacy is mean posttreatment symptom level. A treatment could lead to substantial improvement in most patients but nevertheless leave most patients highly symptomatic. A final variable of crucial importance is sustained efficacy over time. A treatment that produces an initial response, or a response that holds for 3 to 6 months after termination, may or may not be an efficacious treatment for a disorder such as PTSD, which tends to be longstanding.
Method
Selection of Studies
To maximize the likelihood of obtaining all relevant published research, we used a three-phase search process. First, we identified studies using a manual search of 19 high-quality, high-impact journals that routinely publish efficacy research, including research on PTSD (e.g., The American Journal of Psychiatry,Journal of Consulting and Clinical Psychology). Next, we conducted an exhaustive computer search of PsychInfo and Medline, using the key words “PTSD” and “Posttraumatic.” Last, we manually reviewed prior meta-analyses and reviews for studies not obtained using the first two procedures.
We included studies published in the years 1980–2003. Inclusion of only published studies (rather than unpublished, “file-drawer” studies [20]) in this study as in past reviews and meta-analyses means that the findings can only be generalized to published research and therefore could potentially inflate estimates of efficacy. We did this because our prior research using this method with other disorders has identified a number of limitations of the treatment literature we have meta-analyzed, leading to conclusions somewhat at odds with prior reviews. We thus wanted to reexamine data similar to those examined in prior reviews and meta-analyses, from which conclusions about efficacy and treatment of choice have been drawn, without the possibility that any findings reflect sample differences or biases on our part.
To be included, we required studies to meet the following criteria. 1) The study had to test a specific psychotherapeutic treatment for PTSD for efficacy against a control condition, an alternative credible psychotherapeutic treatment, or a combination of two or more of the above (relaxation and biofeedback were included as control conditions, not as primary treatments tested, in accordance with the stated goals and theoretical descriptions of the treatments in the primary articles reviewed). 2) The study had to use a validated self-report measure of PTSD symptoms or a validated structured interview administered and scored by an evaluator blind to treatment condition. In studies reporting both a valid self-report measure and an interview assessment for which the evaluator was not blind, we used only the self-report data in our analyses. 3) The study had to be experimental in design, including random assignment of patients to condition and standardized treatment. 4) Enough patients had to be included to randomly assign 10 patients to each experimental group. We chose a priori to exclude studies with fewer than 10 patients per condition because of methodological concerns about studies that build in too little power to detect effects and because of concerns about maintaining the blind with such small Ns. 5) The study had to be reported in English. We excluded studies that reanalyzed data already included in the meta-analysis unless they provided new data. We included only studies that used adult patients and that examined treatment of PTSD proper (rather than acute stress disorder, preventive programs such as debriefing in the wake of a traumatic event, etc.). All decisions of this sort were made a priori, before examining any individual studies.
Procedure
We assessed the following variables: number of participants, participant inclusion rate (out of those screened for participation), number of exclusion criteria, study completion rate, effect size (for both treatment versus control conditions and pre- versus posttreatment), rate of diagnostic change (i.e., patients no longer meeting criteria for PTSD), improvement rate (for study completers as well as the intent-to-treat study group), and mean posttreatment symptom level. We assessed the same variables at follow-up intervals of 6 months and beyond.
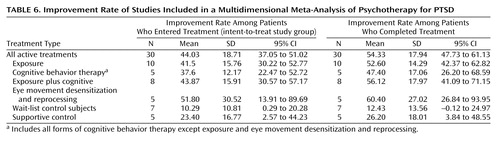
Table 1 lists each study, each active and control condition, and the data we extracted and analyzed so that researchers can directly assess our decisions and results. Decisions about how to code or define variables reflected our consistent efforts to 1) make methodological decisions prior to examining the data where possible, and 2) give the treatments under consideration the “benefit of the doubt” (18). For example, when researchers reported alternative values for the same analyses in the text and tables, we used the values that had the best results for the treatment. Two raters (each blind to the other’s ratings) coded each of the variables to ensure accuracy.
Definition of Primary Variables
Number of participants refers to the number of people who actually began treatment (i.e., the number randomly assigned to any treatment condition who attended at least one session).
Number screened refers to the number of patients researchers reported screening for inclusion in the study (e.g., in initial interviews). In some cases, researchers first prescreened participants via phone and then in person. In these cases, we used the number screened rather than prescreened to maximize comparability to data from studies that did not report prescreening numbers. This produced a conservative estimate of number screened and exclusion rate because it does not include those initially screened out after a prescreening call (or those prescreened by referral sources, who are often aware of the kinds of patients researchers do and do not want included in a treatment study).
Number of exclusion criteria refers to the number of separate criteria used to exclude patients from a study. We did not count presence of psychosis, organic impairment, involvement in the legal system, or failure to meet criteria for PTSD in this number, given that these are criteria that would likely lead a clinician in everyday practice to refer the patient or apply a different treatment. Since researchers enumerated multiple exclusion criteria related to alcohol or drugs (e.g., drug abuse or dependence), we counted this as one exclusionary criterion to maximize comparability across studies. Determining the exact nature of the screening criteria was sometimes difficult because these criteria often included many unstated assumptions. Many studies offered broad exclusion criteria such as “major mental illness,” whereas others presented more precise lists. Thus, simply counting the number of screening criteria might not provide an accurate picture. As in prior meta-analyses (17, 18), we assigned highly generalized criteria (e.g., severe chronic preinjury mental health difficulties) a score equal to the highest number of specific exclusionary criteria in the sample plus one.
Inclusion rate refers to the proportion of patients who were randomly assigned after surviving inclusion and exclusion criteria and attrition before the first treatment session.
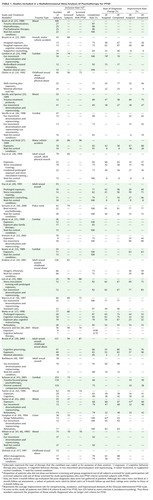
Effect size was calculated by using Cohen’s d with the following formula: ([mean1–mean2]/[SD12+SD22])/2. When means or standard deviations were not reported, where possible we calculated effect size from other data provided (20). For articles reporting effect sizes without reporting raw data, we relied on the effect sizes provided in the published report. Where data were provided only in graphic form, we interpolated. We calculated effect sizes for both pre- versus posttreatment and treatment versus control condition. In cases where both full-scale and subscale scores for a PTSD measure were reported, we used the full-scale score. If subscale data only were reported, we aggregated the scales. Where the investigators reported data on multiple measures of PTSD symptoms, we aggregated the effect sizes across measures. We present these effect sizes in Table 2.
Posttreatment scores were analyzed by using the two most commonly used PTSD assessment instruments, the PTSD Symptom Scale (either the interview or self-report version) and the Impact of Event Scale.
Rate of diagnostic change is the proportion of patients who met diagnostic criteria for PTSD pretreatment but no longer met these criteria posttreatment. We calculated this variable for both study completers and the intent-to-treat study group.
In the absence of agreed-upon standards for clinically meaningful improvement, as in prior studies, we calculated improvement rates (of patients entering as well as completing treatment) by relying on definitions for improvement used by the authors. Typical examples of criteria for improvement were PTSD Symptom Scale score <20 or a decrease of two or more standard deviations in PTSD Symptom Scale score.
Results
The sample included data from 26 studies (21–47) that included 44 treatment conditions. The treatment conditions included 13 exposure-based therapies, five cognitive behavior therapy treatments other than exposure, nine combined cognitive behavior therapy and exposure, 10 eye movement desensitization and reprocessing, and seven other. Twenty-three studies included control conditions: wait-list (we included minimal contact and no contact control conditions in this category [N=15]) and supportive control (patients received some form of professional attention, including process-oriented therapy, supportive therapy, and relaxation/biofeedback [N=8]). Length of treatment ranged from 3 to 52 hours (number of hours per session varied across studies); the average length was 15.64 hours (SD=10.52). The total number of patients reported across all studies, including both treatment and control conditions, was 1,535, with 966 receiving active treatment, 317 assigned to wait-list control conditions, and 252 receiving placebo treatment.
Inclusion/Exclusion Criteria and Completion Rates
Table 3 summarizes inclusion and completion rates. Although such data are crucial for generalizing from any study, they were missing from roughly 40% of published reports. Of those reporting inclusion rates, the mean was 70% inclusion (30% exclusion). Although most of the 26 studies appropriately excluded patients with psychosis (N=22, 85%) or organic disorders (N=20, 77%), most imposed additional criteria limiting generalizability to the population of treatment-seeking patients with PTSD. Twelve studies (46%) excluded potential participants for suicide risk. Sixteen (62%) excluded those with drug or alcohol abuse/dependence, and another 16 (62%) used some version of “serious comorbidity” as an exclusion criterion. Precisely what the comorbidity was could often not be ascertained. Several studies excluded participants because PTSD was not the “primary” diagnosis but did not specify how that decision was made (and how reliably).
An important distinction in evaluating the meaning of exclusion rates is between patients excluded because they did not meet PTSD criteria and those excluded for some other reason (e.g., comorbidity or suicidality). Unfortunately, the majority of studies did not provide data to allow us to make this determination. The studies reviewed also generally did not provide systematic data on comorbidity in patients included in the study. Only 11 (42%) reported any axis I comorbidity data, and three (12%) reported axis II comorbidity.
Most patients who entered a study completed treatment (78.9%). Overall, only small differences emerged between treatments in completion rates (Table 3).
Effect Size
Table 4 reports effect sizes for each type of treatment relative to wait-list control and supportive control conditions as well as for pre- versus postreatment. Across all treatments, the average effect size for pre- versus posttreatment comparisons was 1.43. The average effect size for active versus control treatment comparisons was 1.11 for treatment versus wait-list control and 0.83 for treatment versus supportive control. These figures suggest that psychotherapy for PTSD produces substantial effects. Effect size estimates were predictably highest for pre- versus posttreatment comparisons, which confound treatment effects with passage of time and other variables unrelated to the specific treatment. Effect size estimates were lowest (but nonetheless substantial) for comparisons between active treatment and the supportive therapy control condition. To assess the homogeneity of these effect sizes we used a Q statistic (48, p. 123). A significant Q indicates heterogeneity across studies deserving further exploration (49). The Q was significant (p<0.001) for all three effect size estimates (pre- versus posttreatment and active treatment versus both wait-list control and supportive control conditions). Thus, we followed these data up with moderator analyses.
Given the relatively small number of studies, we lacked adequate power to compare different types of treatment. However, the descriptive data suggest relatively small differences (Table 4). Researchers directly compared exposure to cognitive behavior therapy, combined exposure plus cognitive behavior therapy, or eye movement desensitization and reprocessing in 12 cases. Given the suggestion in the literature of the particular efficacy of exposure, we calculated effect sizes for these studies by subtracting the exposure posttreatment score from the posttreatment scores of the other therapy approaches; thus, a positive effect size resulted when exposure yielded lower symptom levels. Across studies, we found an average effect size of –0.11 (SD=0.44). In seven cases, researchers compared cognitive behavior therapy to other specific treatments; here we similarly subtracted cognitive behavior therapy posttreatment means from those of the other therapies. The average effect size was 0.05 (SD=0.40). Researchers compared exposure plus cognitive behavior therapy to other forms of therapy in nine cases, yielding a mean effect size of 0.16 (SD=0.40). Finally, in the five cases that compared eye movement desensitization and reprocessing to other forms of therapy, the average effect size was 0.11 (SD=0.60). It should be noted that these analyses are not independent, since they each included some percent of overlapping cases. At least within the range of treatments studied, the data thus do not support differential efficacy.
Diagnostic Change and Improvement Rates
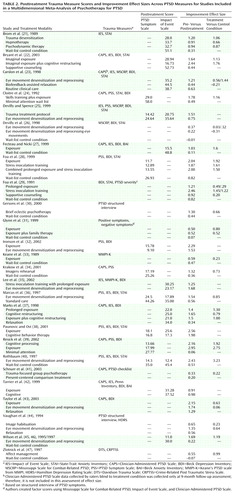
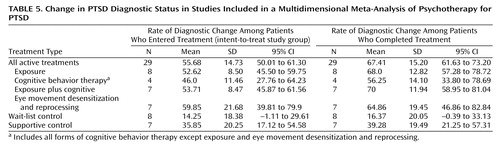
Approximately 62% of studies reported the proportion of patients no longer meeting criteria for PTSD, and 65% reported on the proportion classified as improved. Across all treatments, 56% of all those who entered treatment, including those who did not complete the study (i.e., the intent-to-treat group), and 67% of the patients who completed treatment no longer met criteria for PTSD posttreatment (Table 5). Using author-defined criteria for clinically meaningful improvement, 44% of all those who entered treatment and 54% of those who completed treatment were classified as improved at the end of the study (Table 6). As can be seen from the tables, the confidence intervals overlapped for all treatments and sometimes, although marginally, with supportive therapy control conditions.
Posttreatment Symptom Level
An index of outcome that has received little attention in prior reviews is mean posttreatment symptom level. At termination, across treatments, the average patient had a PTSD Symptom Scale score of 17.28 (SD=5.34, N=14) and an Impact of Event Scale score of 23.96 (SD=7.96, N=7.97) Thus, the average patient showed clinically meaningful improvement, particularly relative to wait-list control condition patients, although these posttreatment means suggest considerable residual symptoms.
Follow-Up Studies
We next examined follow-up data, including studies with follow-up points of at least 6 months. As in our prior research, we intended to focus only on extended follow-up studies (1 year or more after treatment) given the relative durability of PTSD symptoms over time, but the low number of such studies rendered this impossible. Ten studies included follow-up evaluations at ≥6 months (assessing 21 conditions, total N=308); however, the majority of follow-up studies assessed outcome only at 6 months, with only two assessing outcome as far as 12 months posttreatment.
Effect sizes for comparison of pretreatment and follow-up data were large (mean=1.52, SD=0.95), with 62% of patients falling below diagnostic thresholds for PTSD (SD=17.60, N=7) and 32% meeting the investigators’ criteria for improvement (SD=26.28, N=10). Only one study (42), however, reported the proportion of patients recovered at follow-up who remained improved, rendering unknown the extent to which patients described as improved or recovered at follow-up were the same as those who benefited initially from the treatment. Too few follow-up studies exist to compare specific treatments in outcome over time; however, as above, the descriptive statistics suggest little difference, with the confidence intervals for the only follow-up variable that could be meta-analyzed (effect size for pre- versus postreatment comparison) overlapping for exposure (95% CI=0.92 to 2.57 [N=9]), cognitive behavior therapy (95% CI=–0.11 to 3.01 [N=3]), and combined exposure plus cognitive behavior therapy (95% CI=1.58 to 2.55 [N=5]).
Moderator Variables
On the basis of findings from prior meta-analyses, we examined several potential moderator variables, including 1) year the report was published, 2) sample size, 3) quality of diagnosis, 4) number of exclusion criteria, 5) exclusion rate, and 6) completion rate. We also looked at type of trauma. We used pre- versus posttreatment effect size, treatment versus wait-list control effect size, rate of diagnostic change, and improvement rate as measures of treatment outcome because these were the measures for which we had a high enough number of treatment conditions to begin examining moderators. We consider these findings preliminary, as many are underpowered.
Sample size was unrelated to outcome; hence we report in this study only unweighted means. None of the other moderator variables was associated significantly with change in diagnosis or percent improved. Year of publication, however, was positively associated with pre- versus posttreatment effect sizes (r=0.36, df=48, p=0.01) and treatment versus wait-list control effect sizes (r=0.42, df=23, p=0.04), indicating that more recent treatments had larger initial effects than earlier treatments. The number of exclusion criteria was significantly related to pre- versus posttreatment effect size (r=0.42, df=23, p=0.03), such that studies with more exclusion criteria reported higher effect sizes. Completion rate was negatively related to pre- versus posttreatment effect size (r=–0.32, df=50, p=0.02), indicating that the fewer patients who completed the study, the higher the effect size. Finally, we examined type of trauma, which we coded into three categories: combat, sexual or physical assault, and mixed/other. Type of trauma was a significant predictor of pre- versus posttreatment effect size (F=8.62, df=2, 49, p=0.001). The combat group showed the least change (mean=0.81, SD=0.78), followed by the mixed group (mean=1.24, SD=0.52), and then the assault group (mean=1.82, SD=0.66). Because of the relatively small number of studies, we could not enter more than one moderator into a regression equation.
Discussion
On average, the brief psychotherapy approaches tested in the laboratory produce substantial improvements for patients with PTSD. Of patients who complete treatment, 67% no longer meet criteria for PTSD, and of those who enter treatment (whether or not they complete), the recovery rate is 56%. These findings are particularly impressive given that PTSD is often a chronic disorder. Most patients complete treatment, which is also impressive given the aversive nature of some of the treatments. Preliminary analyses indicated that the completion rate is, however, negatively associated with at least one measure of outcome (pre- versus posttreatment effect size), raising the possibility that patients who do not get better tend to drop out and highlighting the importance of presenting and meta-analyzing both completer and intent-to-treat data.
A multidimensional meta-analytic approach has the advantage of calling attention to a number of nuances that may qualify conclusions about outcome or generalizability. We focus here on several such qualifications with implications for future research: exclusion criteria, comorbidity, type of trauma, criteria for successful outcome, follow-up data, and differential efficacy of specific treatments. It is worth noting that many of these issues are not specific to the PTSD literature and are equally applicable to psychotherapy and pharmacotherapy research for many disorders.
Exclusion Criteria and Comorbidity
Clinical trials for PTSD have excluded roughly 30% of patients referred for treatment. This exclusion rate is lower than exclusion rates in controlled trials for many other disorders, such as depression (17). Nevertheless, it raises questions about generalizability to the population of patients treated for PTSD in the community because it is likely an underestimate. In many cases we were unable to determine the extent of prescreening either by telephone or by criteria given to potential referral sources. Our preliminary finding of a positive relationship between number of exclusion criteria and outcome suggests caution in unqualified generalizations about treatment of choice for patients with PTSD, who are a very heterogeneous group (50).
The lack of systematic data on axis I and axis II comorbidity also makes it difficult to specify for which patients the research literature is likely to apply. Overall, data are more available on axis I than axis II comorbidity, although few studies have focused on the potential impact of comorbidity or have had adequate power to detect moderators of outcome. The treatment guidelines from the International Society for Traumatic Stress Studies (51) essentially concur regarding the lack of adequate empirical data to guide treatments for comorbid disorders and suggest the possibility of adding modules to cognitive behavior therapy approaches to address specific forms of comorbidity. Although this may prove to be an effective strategy, it relies on the assumption that disorders are relatively independent of one another and hence can be understood using an essentially additive model of comorbidity, a model that is not supported by basic science research on PTSD or other psychiatric disorders (52). Although most studies did not exclude patients with axis II comorbidity, the common confluence of exclusion criteria for suicide risk and substance abuse/dependence is likely to exclude many patients with borderline features, the presence of which may or may not moderate treatment outcome (53, 54). Also worth noting is that none of the studies addressed the issue of treatment of PTSD with comorbid psychotic symptoms, despite research indicating that PTSD and psychotic symptoms commonly co-occur (55). Ruling out psychosis (typically without reliability of that determination reported) is also not always a simple matter in patients with severe or complex PTSD.
It is unknown whether the tendency of clinicians in community settings not to use empirically supported therapies such as exposure for PTSD reflects a lack of familiarity with the outcome data or the difficulty of applying such treatments to the polysymptomatic patients that are the norm in everyday practice. At this point, however, we would offer three suggestions for future research (which apply to treatment research for virtually all disorders [52]). First, researchers should take much more care in both detailing and justifying exclusion criteria and procedures (e.g., specifying information given to potential referral sources and the number of patients included/excluded at each stage). Second, future studies should impose only those exclusion criteria that are medically necessary or that a reasonable clinician in practice would impose (e.g., organic brain disorders, schizophrenia) and use correlational analyses to identify potential moderators of treatment response. Rather than excluding patients with suicidality for ethical or other reasons, researchers need to build into their treatment protocols contingencies for treating suicidality in PTSD patients, given that suicidality is not an infrequent symptom in PTSD patients. Third, to the extent that researchers exclude patients with co-occurring conditions such as substance abuse, they need to state clearly the population of patients to whom they expect the results to generalize.
Type of Trauma
Consistent with previous reviews and research (56, 57), treatments for combat-related PTSD showed the lowest effect sizes. These findings could have multiple explanations, including 1) greater severity of pathology of veterans who seek treatment at Veterans Administration hospitals; 2) tendency to limit disclosure upon returning home, which limits opportunities for both exposure and social support; and 3) potential for secondary gain (disability-based income may depend on remaining symptomatic). In general, however, the treatment literature does not permit consumers to make many of the most important distinctions among types of trauma, such as distinctions among physical and sexual assault in childhood, adulthood, or both, all of which are typically described as interpersonal violence. Similar to the problem of reporting comorbidity, few studies report data on complete trauma history, which is problematic in light of research suggesting that history of prior or multiple traumatic events affects severity of PTSD and response to subsequent traumas (58).
Criteria for Successful Outcome
Although we attempted to meta-analyze success and recovery, we could do so only very imperfectly because of two related problems. The first is the ambiguous meaning of no longer meeting PTSD criteria after treatment, given that a higher percentage of patients lost the PTSD diagnosis than demonstrated investigator-defined improvement, a situation very different from treatments of many other disorders (17, 18), where substantially more patients improve than fully recover. The ambiguity reflects the fact that patients can fall below diagnostic thresholds by changing only one or two symptoms while remaining highly symptomatic. Indeed, nearly 40% of supportive therapy comparison subjects who completed treatment no longer met criteria for PTSD, and raw posttreatment scores for patients in active conditions indicated substantial residual symptoms. Several recent studies find that subthreshold PTSD is associated with significant impairment in work and social functioning as well as suicide attempts (59, 60), underscoring the importance of clarifying and achieving consensus on standards for improvement and recovery across studies.
Follow-Up Data
Perhaps of most concern for applying the empirical literature to clinical practice is the absence of follow-up studies at extended intervals, given that PTSD is generally a disorder of long duration and frequently co-occurs with many other such disorders. We could identify only two studies with follow-up data at 12 months. For studies reporting follow-up data at 6–12 months, virtually none reported the proportion of patients with sustained improvement (i.e., those who get better and remain better). This can lead to the mistaken impression that patients who spontaneously remitted or sought other forms of treatment following an unsuccessful or partially successful treatment were treatment successes, or that those who initially improved or recovered did not experience a return of symptoms.
Differential Efficacy
We did not find support for differential efficacy across cognitive behavior treatments (e.g., those with or without exposure) or between cognitive behavior therapy and eye movement desensitization and reprocessing. Several potential explanations may account for these findings. The first is the dearth of research comparing a wide enough range of treatments and statistical power to provide definitive answers (61). Second, to control for length of treatment, the majority of studies comparing exposure to other cognitive behavior therapy approaches have condensed two treatments into the same number of sessions as each alone, raising questions about whether either treatment component is of adequate “dose.” Third, many treatments for PTSD share not only factors common to all psychotherapeutic approaches (the common factors traditionally described in the treatment literature; for such factors in PTSD, see reference 62) but also factors common to brief treatments focused on helping patients deal with traumatic events. For example, exposure may not only foster habituation or extinction but may also provide an opportunity for rethinking previous interpretations of the traumatic event. Similarly, therapy designed to address faulty cognitions or maladaptive coping strategies may indirectly foster exposure. Even psychodynamic treatments employ an exposure model to treat trauma, suggesting that patients need to confront their fears and be able to think freely and openly about them. Finally, different kinds of treatment may be more efficacious for different kinds of patients, although the search for such patient-by-treatment interactions has as yet been disappointing (63).
Limitations
Meta-analysis, like any procedure, has its advantages and limits (20, 64), and this study is no exception. For example, because we were interested in reexamining conclusions drawn from the published literature, we did not attempt to address the “file drawer” problem by tracking down unpublished studies. Similarly, too little is written about investigator bias in meta-analysis and the importance of maintaining blindness in making determinations that can substantially affect the findings. On the other hand, research over 50 years has consistently shown the advantages of statistical analysis over informal, synthetic judgments of the type made in qualitative literature reviews. The best we can do is to present a range of statistics that summarize the data as comprehensively as possible and let readers study the tables and draw their own conclusions.
Implications
This study has four primary implications. First, a variety of treatments, primarily exposure, other cognitive behavior therapy approaches, and eye movement desensitization and reprocessing, are highly efficacious in reducing PTSD symptoms. For 40%–70% of the patients who meet screening criteria for controlled clinical trials, relatively brief treatments are able to reduce their symptoms substantially or render them no longer diagnosable with PTSD. To what extent these effects are sustained beyond 6–12 months is unknown.
Second, given the numbers and types of patients who either are not included in these studies (e.g., substance abusers) or do not respond, we need to evaluate alternative or augmented treatments and vary treatment parameters in randomized trials, such as treatment length. It is unknown to what extent the treatments tested thus far are the most effective treatments for polysymptomatic patients with repeated childhood traumas, for which the focus of exposure is less clear and the broader impact on personality is likely to be more pervasive.
Third, this review, along with others (61), suggests that several factors in treatment design and reporting limit our capacity to draw more directly clinically applicable conclusions from the current treatment literature on PTSD. Many variables essential for drawing accurate conclusions and generalizing from efficacy trials to clinical practice are not reported often enough to allow for meta-analytic or even qualitative review.
Finally, the widespread use of wait-list and inert control conditions is highly problematic, as such control conditions do not rule out the common factors (65) that constitute the major threat to internal validity of these studies and do not control obvious confounds such as clinician commitment and belief in the treatment. The two most common control conditions other than wait list have been relaxation therapy and supportive psychotherapy, neither of which has been intended (and presumably perceived by the research therapists conducting them) to succeed. At this point, it seems to us unwise to design any further studies with any form of controls other than genuine therapies with committed therapists, preferably treatments as practiced in the community, working with samples of patients resembling those seen in the community. If researchers hope to convince experienced clinicians to make greater use of treatments studied in the laboratory, they need to demonstrate that such treatments are in fact superior to what clinicians are already doing in private practice or other settings with the opportunity for more open-ended care.
 |
 |
 |
 |
 |
 |
Received Sept. 10, 2003; revision received April 20, 2004; accepted June 1, 2004. From the Department of Psychology and the Department of Psychiatry and Behavioral Sciences, Emory University; and the Department of Psychology, Boston University, Boston. Address correspondence and reprint requests to Dr. Bradley, Department of Psychiatry and Behavioral Sciences, Emory University, 1462 Clifton Rd., Atlanta, GA 30322; [email protected] (e-mail). Preparation of this research was supported by NIMH grants MH-062377 and MH-062378 to Dr. Westen.
1. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson C: Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995; 52:1048–1060Crossref, Medline, Google Scholar
2. Shapiro F: Eye Movement Desensitization and Reprocessing: Basic Principles, Protocols, and Procedures. New York, Guilford, 1995Google Scholar
3. Wachtel PL: EMDR and psychoanalysis, in EMDR as an Integrative Psychotherapy Approach: Experts of Diverse Orientations Explore the Paradigm Prism. Edited by Shapiro F. Washington, DC, American Psychological Association, 2002Google Scholar
4. Barrowcliff AL, Gray NS, MacCulloch S, Freeman TC, MacCulloch MJ: Horizontal rhythmical eye movements consistently diminish the arousal provoked by auditory stimuli. Br J Clin Psychol 2003; 42:289–302Crossref, Medline, Google Scholar
5. Sherman JJ: Effects of psychotherapeutic treatments for PTSD: a meta-analysis of controlled clinical trials. J Trauma Stress 1998; 11:413–435Crossref, Medline, Google Scholar
6. Van Etten ML, Taylor S: Comparative efficacy of treatments for post-traumatic stress disorder: a meta-analysis. Clin Psychol Psychother 1998; 5:126–144Crossref, Google Scholar
7. Davidson PR, Parker KC: Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001; 69:305–316Crossref, Medline, Google Scholar
8. Hembree EA, Foa EB: Posttraumatic stress disorder: psychological factors and psychosocial interventions. J Clin Psychiatry 2000; 61(suppl 7):33–39Google Scholar
9. Foa EB, Rothbaum BO, Furr JM: Augmenting exposure therapy with other CBT procedures. Psychiatr Annals 2003; 33:47–53Crossref, Google Scholar
10. Hembree EA, Marshall RD, Fitzgibbons LA, Foa EB: The difficult-to-treat patient with posttraumatic stress disorder, in The Difficult-to-Treat Psychiatric Patient. Edited by Dewan MJ, Pies RW. Washington, DC, American Psychiatric Publishing, 2001, pp 149–178Google Scholar
11. Jaycox LH, Foa EB, Morral AR: Influence of emotional engagement and habituation on exposure therapy for PTSD. J Consult Clin Psychol 1998; 66:185–192Crossref, Medline, Google Scholar
12. Taylor S, Federoff IC, Koch WJ, Thordarson DS, Fecteau G, Nicki RM: Posttraumatic stress disorder arising after road traffic collisions: patterns of response to cognitive-behavior therapy. J Consult Clin Psychol 2001; 69:541–551Crossref, Medline, Google Scholar
13. Tarrier N, Sommerfield C, Pilgrim H, Fragher B: Factors associated with outcome of cognitive-behavioural treatment of chronic post-traumatic stress disorder. Behav Res Ther 2000; 38:191–202Crossref, Medline, Google Scholar
14. van Minnen A, Arntz A, Keijsers GPJ: Prolonged exposure in patients with chronic PTSD: predictors of treatment outcome and dropout. Behav Res Ther 2002; 40:439–457Crossref, Medline, Google Scholar
15. Breslau N, Davis GC, Andreski P, Peterson E: Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991; 48:216–222Crossref, Medline, Google Scholar
16. Yen SRS, Shea TM, Battlle LC, Johnson DM, Zlotnick C, Dolan-Sewell R, Skodol AE, Grilo CM, Gunderson JG, Sanislow CA, Zanarini MC, Bender DS, Rettew JM, McGlashan T: Traumatic exposure and posttraumatic stress disorder in borderline, schizotypal, avoidant and obsessive-compulsive personality disorders: findings from the Collaborative Longitudinal Personality Disorders Study. J Nerv Ment Dis 2002; 190:510–518Crossref, Medline, Google Scholar
17. Westen D, Morrison K: A multidimensional meta-analysis of treatments for depression, panic, and generalized anxiety disorder: an empirical examination of the status of empirically supported therapies. J Consult Clin Psychol 2001; 69:875–899Crossref, Medline, Google Scholar
18. Thompson-Brenner H, Glass S, Westen D: A multidimensional meta-analysis of psychotherapy for bulimia nervosa. Clin Psychol Sci Practice 2003; 10:269–287Crossref, Google Scholar
19. Kendall PC, Marrs-Garcia A, Nath SR, Sheldrick RC: Normative comparisons for the evaluation of clinical significance. J Consult Clin Psychol 1999; 67:285–299Crossref, Medline, Google Scholar
20. Rosenthal R: Meta-Analytic Procedures for Social Research. Thousand Oaks, Calif, Sage Publications, 1991Google Scholar
21. Brom D, Kleber RJ, Defares PB: Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989; 57:607–612Crossref, Medline, Google Scholar
22. Bryant RA, Moulds ML, Guthrie RM, Dang ST, Nixon RDV: Imaginal exposure alone and imaginal exposure with cognitive restructuring in treatment of posttraumatic stress disorder. J Consult Clin Psychol 2003; 71:706–712Crossref, Medline, Google Scholar
23. Carlson JG, Chemtob CM, Rusnak K, Hedlund NL, Muraoka MY: Eye movement desensitization and reprocessing (EMDR) treatment for combat-related posttraumatic stress disorder. J Trauma Stress 1998; 11:3–24Crossref, Medline, Google Scholar
24. Cloitre M, Koenen KC, Cohen LR, Han H: Skills training in affective and interpersonal regulation followed by exposure: a phase-based treatment for PTSD related to child abuse. J Consult Clin Psychol 2002; 70:1067–1074Crossref, Medline, Google Scholar
25. Devilly GJ, Spence SH: The relative efficacy and treatment distress of EMDR and a cognitive-behavior trauma treatment protocol in the amelioration of posttraumatic stress disorder. J Anxiety Disord 1999; 13:131–157Crossref, Medline, Google Scholar
26. Devilly GJ, Spence SH, Rapee RM: Statistical and reliable change with eye movement desensitization and reprocessing: treating trauma within a veteran population. Behav Ther 1998; 29:435–455Crossref, Google Scholar
27. Fecteau G, Nicki R: Cognitive behavioural treatment of post traumatic stress disorder after motor vehicle accident. Behavioural and Cognitive Psychotherapy 1999; 27:201–214Crossref, Google Scholar
28. Foa EB, Dancu CV, Hembree EA, Jaycox LH, Meadows EA, Street GP: A comparison of exposure therapy, stress inoculation training, and their combination for reducing posttraumatic stress disorder in female assault victims. J Consult Clin Psychol 1999; 67:194–200Crossref, Medline, Google Scholar
29. Foa EB, Rothbaum BO, Riggs DS, Murdock TB: Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991; 59:715–723Crossref, Medline, Google Scholar
30. Gersons BPR, Carlier IVE, Lamberts RD, van der Kolk BA: Randomized clinical trial of brief eclectic psychotherapy for police officers with posttraumatic stress disorder. J Trauma Stress 2000; 13:333–347Crossref, Medline, Google Scholar
31. Glynn SM, Eth S, Randolph ET, Foy DW, Urbaitis M, Boxer L, Paz GG, Leong GB, Firman G, Salk JD, Katzman JW, Crothers J: A test of behavioral family therapy to augment exposure for combat-related posttraumatic stress disorder. J Consult Clin Psychol 1999; 67:243–251Crossref, Medline, Google Scholar
32. Ironson G, Freund B, Strauss JL, Williams J: Comparison of two treatments for traumatic stress: a community-based study of EMDR and prolonged exposure. J Clin Psychol 2002; 58:113–128Crossref, Medline, Google Scholar
33. Keane TM, Fairbank JA, Caddell JM, Zimering RT: Implosive (flooding) therapy reduces symptoms of PTSD in Vietnam combat veterans. Behav Ther 1989; 20:245–260Crossref, Google Scholar
34. Krakow B, Hollifield M, Johnston L, Koss M, Schrader R, Warner TD, Tandberg D, Lauriello J, McBride L, Cutchen L, Cheng D, Emmons S, Germain A, Melendrez D, Sandoval D, Prince H: Imagery rehearsal therapy for chronic nightmares in sexual assault survivors with posttraumatic stress disorder. JAMA 2001; 286:537–545Crossref, Medline, Google Scholar
35. Lee C, Gavriel H, Drummond P, Richards J, Greenwald R: Treatment of PTSD: stress inoculation training with prolonged exposure compared to EMDR. J Clin Psychol 2002; 58:1071–1089Crossref, Medline, Google Scholar
36. Marcus SV, Marquis P, Sakai C: Controlled study of treatment of PTSD using EMDR in an HMO setting. Psychotherapy 1997; 34:307–315Crossref, Google Scholar
37. Marks I, Lovell K, Noshirvani H, Livanou M, Thrasher S: Treatment of posttraumatic stress disorder by exposure and/or cognitive restructuring. Arch Gen Psychiatry 1998; 55:317–324Crossref, Medline, Google Scholar
38. Paunovic N, Ost L: Cognitive-behavior therapy vs exposure therapy in the treatment of PTSD in refugees. Behav Res Ther 2001; 39:1183–1197Crossref, Medline, Google Scholar
39. Resick PA, Nishith P, Weaver TL, Astin MC, Feuer CA: A comparison of cognitive-processing therapy with prolonged exposure and a waiting condition for the treatment of chronic posttraumatic stress disorder in female rape victims. J Consult Clin Psychol 2002; 70:867–879Crossref, Medline, Google Scholar
40. Rothbaum BO: A controlled study of eye movement desensitization and reprocessing in the treatment of post traumatic stress disordered sexual assault victims. Bull Menninger Clin 1997; 61:317–334Medline, Google Scholar
41. Schnurr PP, Friedman MJ, Foy DW, Shea MT, Hsieh FY, Lavori PW, Glynn SM, Wattenberg M, Bernardy NC: Randomized trial of trauma-focused group therapy for posttraumatic stress disorder. Arch Gen Psychiatry 2003; 60:481–489Crossref, Medline, Google Scholar
42. Tarrier N, Pilgrim H, Sommerfield C, Faragher B, Reynolds M, Graham E, Barrowclough C: A randomized trial of cognitive therapy and imaginal exposure in the treatment of chronic posttraumatic stress disorder. J Consult Clin Psychol 1999; 67:13–18Crossref, Medline, Google Scholar
43. Taylor S, Thordarson DS, Maxfield L, Fedoroff IC, Lovell K, Ogrodniczuk J: Comparative efficacy, speed and adverse effects of three PTSD treatments: exposure therapy, EMDR, and relaxation training. J Consult Clin Psychol 2003; 71:330–338Crossref, Medline, Google Scholar
44. Vaughan K, Armstrong MS, Gold R, O’Connor N, Jenneke W: A trial of eye movement desensitization compared to image habituation training and applied muscle relaxation in posttraumatic stress disorder. J Behav Ther Exp Psychiatry 1994; 25:283–291Crossref, Medline, Google Scholar
45. Wilson SA, Becker LA, Tinker RH: Eye movement desensitization and reprocessing (EMDR) treatment for psychologically traumatized individuals. J Consult Clin Psychol 1995; 63:928–937Crossref, Medline, Google Scholar
46. Wilson SA, Becker LA, Tinker RH: Fifteen-month follow-up of eye movement desensitization and reprocessing (EMDR) treatment for posttraumatic stress disorder and psychological trauma. J Consult Clin Psychol 1997; 65:1047–1056Crossref, Medline, Google Scholar
47. Zlotnick C, Shea TM, Rosen K, Simpson E, Mulrenin K, Begin A, Pearlstein T: An affect management group for women with posttraumatic stress disorder and histories of childhood sexual abuse. J Trauma Stress 1997; 10:425–436Medline, Google Scholar
48. Hedges LV, Olkin I: Statistical Methods for Meta-Analysis. New York, Academic Press, 1985Google Scholar
49. Hunter J, Schmidt F, Jackson G: Meta-Analysis: Cumulating Research Findings Across Studies. Beverly Hills, Calif, Sage Publications, 1982Google Scholar
50. Schuetzwohl M, Maercker A: Effects of varying diagnostic criteria for posttraumatic stress disorder are endorsing the concept of partial PTSD. J Trauma Stress 1999; 12:155–165Crossref, Medline, Google Scholar
51. Shalev AY, Friedman MJ, Foa EB, Keane TM: Integration and summary, in Effective Treatments for PTSD. Edited by Foa EB, Keane TM, Friedman MJ. New York, Guilford, 2000, pp 359–379Google Scholar
52. Westen D, Novotny CM, Thompson-Brenner H: The empirical status of empirically supported psychotherapies: assumptions, findings, and reporting in controlled clinical trials. Psychol Bull 2004; 130:631–663Crossref, Medline, Google Scholar
53. Feeny NC, Zoellner LA, Foa EB: Treatment outcome for chronic PTSD among female assault victims with borderline personality characteristics: a preliminary examination. J Personal Disord 2002; 16:30–40Crossref, Medline, Google Scholar
54. Heffernan K, Cloitre M: A comparison of posttraumatic stress disorder with and without borderline personality disorder among women with a history of childhood sexual abuse: etiological and clinical characteristics. J Nerv Ment Dis 2000; 189:589–595Crossref, Google Scholar
55. Hamner MB, Frueh B, Ulmer HG, Huber MG, Twomey TJ, Tyson C, Arana GW: Psychotic features in chronic posttraumatic stress disorder and schizophrenia: comparative severity. J Nerv Ment Dis 2000; 188:217–221Crossref, Medline, Google Scholar
56. Ford JD, Fisher P, Larson L: Object relations as a predictor of treatment outcome with chronic posttraumatic stress disorder. J Consult Clin Psychol 1997; 65:547–559Crossref, Medline, Google Scholar
57. Johnson DR, Rosenheck R, Fontana A, Lubin H, Southwick S, Charney D: Outcome of intensive inpatient treatment for combat-related posttraumatic stress disorder. Am J Psychiatry 1996; 153:771–777Link, Google Scholar
58. Bremner JD, Southwick SM, Johnson DR, Yehuda R, Charney DS: Childhood physical abuse and combat-related posttraumatic stress disorder in Vietnam veterans. Am J Psychiatry 1993; 150:235–239Link, Google Scholar
59. Marshall RD, Galea S, Kilpatrick D: Psychiatric consequences of September 11 (letter). JAMA 2002; 288:2683–2684Crossref, Medline, Google Scholar
60. Zlotnick C, Franklin L, Zimmerman M: Does “subthreshold” posttraumatic stress disorder have any clinical relevance? Compr Psychiatry 2002; 43:413–419Crossref, Medline, Google Scholar
61. Harvey AG, Bryant RA, Tarrier N: Cognitive behaviour therapy for posttraumatic stress disorder. Clin Psychol Rev 2003; 23:501–522Crossref, Medline, Google Scholar
62. Bradley RG, Follingstad DR: Utilizing disclosure in the treatment of the sequelae of childhood sexual abuse: a theoretical and empirical review. Clin Psychol Rev 2001; 21:1–32Crossref, Medline, Google Scholar
63. Petry NM, Tennen H, Affleck G: Stalking the elusive client variable in psychotherapy research, in Handbook of Psychological Change. Edited by Snyder CR, Ingram RE. New York, John Wiley & Sons, 2000, pp 88–108Google Scholar
64. Eysenck HJ: Meta-analysis squared-does it make sense? Am Psychol 1995; 50:110–111Crossref, Google Scholar
65. Weinberger J: Common factors aren’t so common: the common factors dilemma. Clin Psychol Sci Practice 1995; 2:45–69Crossref, Google Scholar

