
Anxiety Disorder Comorbidity in Bipolar Disorder Patients: Data From the First 500 Participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD)
Abstract
OBJECTIVE: The authors provide a detailed perspective on the correlates of comorbid anxiety in a large, well-characterized sample of bipolar disorder patients. METHOD: Anxiety and its correlates were examined in a cross-sectional sample from the first 500 patients with bipolar I or bipolar II disorder enrolled in the Systematic Treatment Enhancement Program for Bipolar Disorder, a multicenter project funded by the National Institute of Mental Health designed to evaluate the longitudinal outcome of patients with bipolar disorder. RESULTS: Lifetime comorbid anxiety disorders were common, occurring in over one-half of the sample, and were associated with younger age at onset, decreased likelihood of recovery, poorer role functioning and quality of life, less time euthymic, and greater likelihood of suicide attempts. Although substance abuse disorders were particularly prevalent among patients with anxiety disorders, comorbid anxiety appeared to exert an independent, deleterious effect on functioning, including history of suicide attempts (odds ratio=2.45, 95% CI=1.4–4.2). CONCLUSIONS: An independent association of comorbid anxiety with greater severity and impairment in bipolar disorder patients was demonstrated, highlighting the need for greater clinical attention to anxiety in this population, particularly for enhanced clinical monitoring of suicidality. In addition, it is important to determine whether effective treatment of anxiety symptoms can lessen bipolar disorder severity, improve response to treatment of manic or depressive symptoms, or reduce suicidality.
Data from both epidemiologic and clinical samples indicate elevated rates of anxiety disorders among patients with bipolar disorder (1–7). Comorbid anxiety disorders have been reported at rates of 10.6%–62.5% for panic disorder, 7.8%–47.2% for social anxiety disorder, 3.2%–35% for obsessive-compulsive disorder (OCD), 7%–38.8% for posttraumatic stress disorder (PTSD), and 7%–32% for generalized anxiety disorder. The clinical significance of comorbid anxiety has been less well delineated, though greater severity and dysfunction are suggested. High levels of anxiety symptoms have been associated with greater suicidality, substance abuse, and lower lithium responsivity (5, 8). Emerging data support a detrimental role for panic attacks, anxiety, and panic spectrum symptoms on bipolar disorder outcome (9, 10).
In this article, we provide a comprehensive perspective on the correlates of comorbid anxiety in the largest well-characterized sample of bipolar disorder patients published to date. We extend previous findings by examining specific current and lifetime anxiety disorders and their link to measures of bipolar severity, suicide attempts, and functional impairment in 475 patients. We also examine bipolar I and bipolar II subtypes, delineate the impact of anxiety from substance use disorders, and separately examine the impact of comorbid anxiety in different phases of bipolar disorder. We hypothesized that comorbid anxiety would be associated with markers of greater bipolar disorder severity and that the correlates of comorbid anxiety would exist independently from those of substance use disorders.
Method
Study Overview
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) is a multicenter project funded by the National Institute of Mental Health designed to evaluate the longitudinal outcome of patients with bipolar disorder. The overall study combines a large prospective naturalistic study and a series of randomized controlled trials (11). To enter the STEP-BD, patients are required to be at least 15 years of age and meet DSM-IV criteria for bipolar I disorder, bipolar II disorder, cyclothymia, bipolar disorder not otherwise specified, or schizoaffective manic or bipolar subtypes (12). Exclusion criteria are limited to unwillingness or inability to comply with study assessments or to give informed consent. After description of the study, written informed consent was obtained. For the present report, participants were the first 500 patients entered into the STEP-BD who met lifetime criteria for bipolar I or II disorder and who had completed baseline diagnostic assessments of comorbid anxiety.
Procedures
Diagnoses were obtained by semistructured interview utilizing the Mini International Neuropsychiatric Interview (MINI Plus Version 5.0 [13]), adapted to additionally assess lifetime anxiety and eating disorders. On the basis of presence or absence of DSM-IV-based criteria, one of eight operationally defined clinical states was assigned as the current clinical status. Four clinical states corresponded to the DSM-IV definitions for major depression, mania, hypomania, or mixed episodes. Patients achieving relative euthymia (two or fewer moderate symptoms) for at least a week were assigned a status of recovering or recovered, depending on whether this status had been sustained for at least 8 weeks. Two subsyndromal states (three or more moderate symptoms but not full criteria for a mood episode) categorized patients as either continued symptomatic (a subsyndromal state following an acute episode without an intervening full recovery) or roughening (a subsyndromal state occurring after recovery from the last full mood episode). These bipolar state categories and interrater reliability training are further discussed by Sachs et al. (11).
For the present study, data from all instruments were collected cross-sectionally at study initiation, regardless of treatment or clinical status. Information on the course and severity of bipolar symptoms, including age at onset, history of suicide attempts, and the longest euthymic period (“mood has been consistently normal”) in the preceding 2 years was elicited as part of the baseline semistructured interview (see Sachs et al. [11]). Quality of life and functional impairment were assessed with two patient-rated scales, the short form of the Quality of Life and Enjoyment Scale (14) and the Range of Impaired Functioning Tool (14, 15).
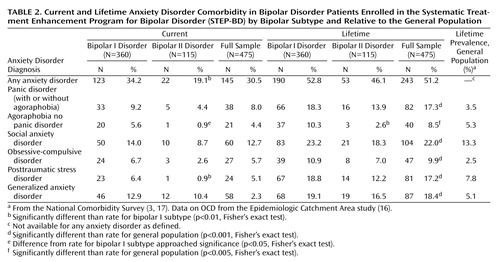
Within the class of anxiety disorders, we separately examined panic disorder with or without agoraphobia, agoraphobia without panic disorder, social anxiety disorder, OCD, PTSD, and generalized anxiety disorder. We defined “any anxiety disorder” as having met DSM-IV criteria for at least one of these six disorders.
Statistical Analyses
For all binary comparisons, Fisher’s exact test was used. Two-sided, two-sample t tests were performed for continuous variables. In the case of unequal variance, a conservative Sattherwaite correction was applied. The ordered categories of education were examined with a Cochran-Armitage Test for Trend. Because of the large number of tests, we conservatively set the level of significance at p<0.01 and report results that approached significance if they met a threshold of p<0.05. In addition, we examined whether the prediction afforded by comorbid anxiety was redundant with other variables by conducting a number of follow-up, stepwise, linear, and logistic regression equations.
Results
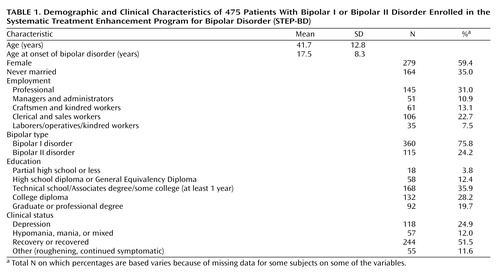
Patient characteristics are presented in Table 1. Twenty-five patients of the original 500 were excluded because of missing diagnostic or clinical status data at baseline.
Comorbid Anxiety and Bipolar Disorder Type
The prevalence of any lifetime anxiety disorder for the entire sample was 51.2% and was 30.5% for any current anxiety disorder. Greater overall anxiety comorbidity was seen among patients with bipolar I disorder relative to bipolar II disorder (Table 2), reaching significance only for the presence of at least one current anxiety disorder, current PTSD, and lifetime agoraphobia without panic. The lifetime prevalence of each individual anxiety disorder in the STEP-BD participants was compared with each respective anxiety disorder’s general population prevalence rate from the National Comorbidity Study (3, 17), with the exception of OCD, for which only an Epidemiologic Catchment Area study prevalence rate is available (16). The STEP-BD participants uniformly demonstrated significantly higher lifetime prevalence rates for each individual anxiety disorder than the general population (one-sample test of proportions: all p<0.005) (Table 2).
Comorbid Anxiety and Bipolar Disorder Severity
Age at onset of bipolar disorder was significantly lower for patients with any lifetime anxiety disorder (mean=15.6 years, SD=7.9) than in patients without an anxiety disorder (mean=19.4 years, SD=8.3) (t=5.03, df=471, p<0.0001) and in the presence of each single anxiety disorder except agoraphobia without panic and OCD. Patients with a lifetime anxiety disorder diagnosis had completed less education (Cochran-Armitage Test for Trend z=3.40, p<0.001).
There was wide variability across the sample in the reports of the maximum number of continuous euthymic days in the 2 years before study entry (mean=218, SD=290). Nonetheless, the presence of at least one or any individual current anxiety disorder was associated with a dramatically shorter time euthymic; the longest number of euthymic days was reduced to less than half in the presence of almost all individual anxiety disorders (Figure 1). This effect was also present, but to a lesser degree, for participants with a lifetime history of any anxiety disorder. When both a history of anxiety disorders and current (persisting) anxiety were entered as predictors in a multiple regression equation, only current anxiety offered significant prediction. Furthermore, at baseline evaluation, 59.3% of participants with no current anxiety disorder were recovering or recovered, compared with only 33.8% with at least one anxiety disorder, (p<0.0001, Fisher’s exact test). The proportion of participants currently recovering or recovered was significantly lower in the presence of most individual current anxiety disorders (p<0.01, Fisher’s exact test) with the exception of OCD and panic. For example, only 21% of those with PTSD and 33% of those with generalized anxiety disorder were recovering or recovered.
Rates of lifetime suicide attempts were significantly elevated for patients with at least one lifetime anxiety disorder and for each individual anxiety disorder, with the exception of OCD (Figure 2).
Alcohol and Substance Abuse and Anxiety
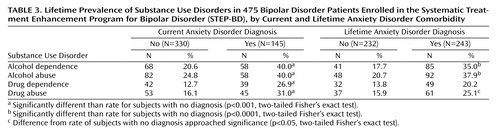
Although lifetime alcohol and substance use disorders were prevalent for the entire sample (37.8% with alcohol abuse or dependence, 26% with substance abuse or dependence), prevalence rates were significantly elevated for those with a current or lifetime anxiety disorder (Table 3). For example, the presence of at least one current anxiety disorder was associated with a doubling of the rate of lifetime alcohol dependence, with 40%–50% of patients with lifetime panic disorder, agoraphobia, social anxiety disorder (all p<0.001) and PTSD (p<0.01) affected (data not shown).
Quality of Life and Function
Anxiety disorder comorbidity was also significantly associated with diminished quality of life and role functioning. The presence of each current anxiety disorder (with the exception of OCD) was associated with poorer functioning (as measured by the Range of Impaired Functioning Tool) and poorer quality of life (as measured by the Quality of Life and Enjoyment Scale) (data not shown). For both of these variables, a lifetime history of comorbid anxiety disorder offered only redundant prediction to the presence of a current anxiety disorder. When the impact of at least one current anxiety disorder on these measures was examined on the basis of current bipolar status, this effect was significant for the Range of Impaired Functioning Tool only for recovered or recovering patients (t=–5.8, df=235, p<0.0001). However, quality of life was worse as determined by the Quality of Life and Enjoyment Scale regardless of bipolar state (t=6.9, df=344, p<0.0001).
Independent Association of Anxiety Disorders With Bipolar Disorder Severity
Because the presence of nonrecovered/recovering bipolar state and alcohol or substance use disorders were common in patients with anxiety disorders, we examined the independent association of anxiety comorbidity with measures of illness severity. We examined three regression models with the Quality of Life and Enjoyment Scale, the Range of Impaired Functioning Tool, and longest euthymic period within the preceding 2 years serving as separate outcome variables. For each model, we examined the impact of at least one current comorbid anxiety disorder after lifetime alcohol or substance abuse/dependence and current bipolar clinical state (e.g., depressed, manic/hypomanic/mixed, euthymic) were controlled. A current anxiety disorder was associated with a robust and consistent detrimental impact on quality of life (t=4.67, p<0.0001), role functioning (t=4.09, p<0.0001), and number of days euthymic (t=3.41, p<0.001), even after current clinical state and the presence of lifetime substance use disorders were controlled. For example, anxiety comorbidity was associated with reduction in length of euthymia from 262 to 113 days. Further, for all three regression models, there was no interaction of anxiety with substance use, suggesting that the detrimental effect associated with anxiety occurs independent of lifetime drug or alcohol abuse or dependence.
Similarly, even when each of the aforementioned covariates was controlled, the presence of a lifetime anxiety disorder was associated with an odds ratio for suicide attempt of 2.45 (95% confidence interval [CI]=1.4–4.2; Wald χ2=11.07, p<0.001) relative to patients without comorbid anxiety, with a similar tendency (odds ratio=1.9, 95% CI=1.09–3.4; Wald χ2=5.19, p<0.05) for those with a current anxiety disorder. Finally, to ensure that differences in functioning and suicide history among patients with anxiety disorders were not dependent on the duration of the bipolar disorder, we examined this variable as a covariate in multiple regression analyses. In the multiple regression analyses including duration of bipolar illness, the presence of comorbid anxiety disorders continued to predict each of the four indices of poorer functioning: less time euthymic, poorer quality of life, greater functional impairment, and an elevated risk for suicide attempts.
Multiple Anxiety Comorbidity
We evaluated the additive influence of multiple anxiety comorbidity by examining the association of number of anxiety disorders (i.e., none, one, two, or more than two) with measures of quality of life, functional impairment, and period of time euthymic, after controlling for current clinical status and substance use in regression models. The presence of multiple anxiety comorbidity was independently associated with added impairment in quality of life (t=2.87, p<0.01) and functioning (t=3.01, p<0.01) and tended to be associated with longest period euthymic (t=2.12, p<0.05).
Discussion
In the largest clinical sample of patients with bipolar I and bipolar II disorder reported to date, we found high levels of anxiety comorbidity, consistent with the growing literature from epidemiologic and outcome studies. We found elevated anxiety comorbidity in bipolar I disorder as did McElroy and colleagues (1), in contrast to reports of an anxiety association specific to bipolar II disorder derived primarily from primary anxiety disorder samples, not primary bipolar cohorts (18, 19).
Our findings of a worse course and poorer functioning among patients with a comorbid lifetime anxiety disorder are consistent with previous observations (1, 5, 9, 10), although our study extends these findings by examining the independent influence of substance abuse and anxiety comorbidity.
In our study, the degree of overlap between anxiety disorders and substance use disorders was striking. Nonetheless, in regression analyses examining the independent prediction afforded by each comorbidity, anxiety comorbidity continued to be significantly associated with poorer outcome (less time euthymic, poorer quality of life, greater functional impairment, and elevated risk for suicide attempts).
In particular, there was a dramatic and significant prediction of past suicide attempts by the presence of a lifetime anxiety disorder, with an odds ratio of 2.45, even after controlling for potential confounding by alcohol and substance disorder comorbidity and clinical bipolar state. Thus, lifetime anxiety comorbidity appears to be a significant marker of risk for a reported history of suicide attempts.
Our finding of a significantly younger age at onset of bipolar disorder in those with lifetime anxiety comorbidity is consistent with epidemiologic data suggesting that the presence of anxiety disorders may predict the onset of bipolar disorder (4), and research work by the Stanley Foundation group (1). Similarly, panic disorder with onset prior to age 21 has been reported to have a significantly higher association with bipolar disorder than later-onset panic disorder (20). Further, a 10-year prospective study of 717 adolescents found that, after controlling for adolescent mania, the presence of a childhood anxiety disorder predicted onset of bipolar disorder in young adulthood (21). However, the precise nature of the relationship between anxiety and bipolar illness remains unclear. Early anxiety may represent a prodromal symptom of bipolar disorder, or alternately, anxiety and bipolar disorders may share an associated biology or genetic risk. For example, recent genetic and family studies have supported a specific panic disorder-bipolar disorder connection, with evidence for a comorbid subtype with shared genetic transmission in some families (22, 23). Moreover, we found that the link between comorbid anxiety disorders and greater disability in bipolar disorder patients was independent of the duration of the bipolar disorder. In addition, anxiety symptoms may, in some cases, represent an inherent component of a more severe bipolar disorder subtype, perhaps attributable to dysphoric stimulation rather than a distinct disorder.
Although there is a growing awareness of the need to treat comorbid disorders such as panic and PTSD (24), anxiety interventions have not been highlighted as critical for high-risk bipolar patients nor for integration into suicide prevention strategies. In our study, anxiety disorders were consistently associated with poorer functioning. More than a decade ago, Fawcett and colleagues suggested anxiety symptoms may be a modifiable risk factor for suicide in individuals with mood disorders (25), but the field has been slow to develop specific anxiety-targeted interventions for patients with bipolar disorder and anxiety comorbidity. Although Frank, Cyranowski, and Shear are developing a modification of interpersonal psychotherapy for patients with unipolar depression and panic comorbidity (MH-49115, E. Frank, principal investigator), there are currently no data examining the efficacy of any anxiety treatment for the prevention of suicide attempts or improvement of clinical course specifically for patients with bipolar disorder. Furthermore, little is known about the precise mechanism by which anxiety elevates suicidality, and study of this issue may need to precede the development of interventions specifically aimed at suicide prevention in this population. Patients with acute anxiety may be less capable of tolerating uncomfortable affects and utilizing other resources, such as social supports or cognitive strategies, to reduce suicidality. Psychosocial interventions to prevent suicide should focus in part on problem-solving skills and improved tolerability of distress (26).
Conclusions drawn from the present study are limited by the cross-sectional nature of the assessments. Specifically, we are unable to address issues of causality and whether anxiety disorders predispose individuals with bipolar disorder to a worse course, or whether it is the characteristics of the bipolar disorder itself that determine anxiety onset. However, inclusion of patients at all levels of symptom severity, treatment, and phase of illness allows for broad generalizability. Nonetheless, conclusions based on some of our subsample analyses with less prevalent anxiety disorders or affective states (e.g., manic/hypomanic/mixed) are limited by relatively low power. In addition, the performance of multiple statistical comparisons may have increased the risk of false positive findings (type I error), although this is tempered to some degree by the use of a significance level of 0.01.
We do not know the extent to which comorbid anxiety motivates patients to seek care. Hence, our clinical sample may overrepresent this comorbidity relative to non-treatment-seeking populations (i.e., Berkson’s bias) (27) and may contribute to our finding of elevated anxiety prevalence compared with rates from epidemiologic samples. However, our results concur with the high levels of overall comorbidity (59.3%) found for bipolar I disorder in the epidemiologically derived National Comorbidity Survey sample (4). In contrast, our rates of substance abuse may be low, given that patients with substance use disorders may be more likely to present at or be referred to primary substance abuse treatment programs than general psychiatric settings. Finally, our reliance on retrospective self-report for lifetime disorders and severity of illness at this cross-sectional assessment does not protect from the possible bias that patients with greater severity of illness may have been more likely to acknowledge a history of anxiety in a structured interview.
Of note, our results do not address the impact of differential anxiety severity nor subsyndromal anxiety features. Anxiety symptoms below the threshold to meet criteria for diagnosis may still exert a pernicious effect on the course of bipolar disorder. For example, lifetime panic spectrum symptoms and traits, regardless of formal panic disorder diagnosis, are associated with greater bipolar severity and longer time to remission with treatment (10). Similarly, poorer treatment outcome has been reported for patients with panic or anxiety symptoms and bipolar I disorder (9). Further research to address these issues is currently ongoing.
In conclusion, anxiety disorder comorbidity is prevalent and appears to be an independent marker of greater severity of bipolar illness and suicide attempts. The presence of anxiety comorbidity should signal a need for enhanced clinical monitoring of suicidality, and a greater understanding of this connection is critical. Little is known about whether effective treatment of anxiety symptoms can lessen bipolar severity, improve response to treatment of manic or depressive symptoms, or reduce suicidality. Further research examining the impact of anxiety on treatment response and course in bipolar disorder is ongoing as part of the STEP-BD study. These efforts may further elucidate the impact of anxiety on bipolar disorder and the need for additional or alternate intervention for patients with bipolar disorder and anxiety comorbidity.
Acknowledgments
Core investigators and collaborators for the Systematic Treatment Enhancement Program for Bipolar Disorder are as follows: Contract: Gary S. Sachs, M.D. (principal investigator), Michael E. Thase, M.D. (co-principal investigator). Site principal investigators and co-principal investigators: Lauren B. Marangell, M.D., and James M. Martinez, M.D. (Baylor College of Medicine); Joseph R. Calabrese, M.D., and Melvin D. Shelton, M.D. (Case Western Reserve University); Michael W. Otto, Ph.D.*, Andrew A. Nierenberg, M.D., and Gary S. Sachs, M.D. (Massachusetts General Hospital and Harvard Medical School); R. Bruce Lydiard, M.D.* (Medical University of South Carolina); Joseph F. Goldberg, M.D. (New York Presbyterian Hospital and Weill Medical College of Cornell University); James C.-Y. Chou, M.D., and Joshua Cohen, D.O. (New York University School of Medicine); John Zajecka, M.D.* (Rush-Presbyterian St. Luke’s Medical Center); Terence A. Ketter, M.D., and Po W. Wang, M.D. (Stanford University School of Medicine); Uriel Halbreich, M.D.* (State University of New York at Buffalo); Alan Gelenberg, M.D.* (University of Arizona); Mark Rapaport, M.D.* (University of California, San Diego); Marshall Thomas, M.D., Michael H. Allen, M.D., and David J. Miklowitz, Ph.D. (University of Colorado Health Sciences Center); Rif S. El-Mallakh, M.D. (University of Louisville School of Medicine); Peter Hauser, M.D.* (University of Maryland); Jayendra Patel, M.D. (University of Massachusetts Medical Center); Kemal Sagduyu, M.D. (University of Missouri-Kansas City School of Medicine, Western Missouri Mental Health Center); Mark D. Fossey, M.D., and William R. Yates, M.D. (University of Oklahoma College of Medicine); Laszlo Gyulai, M.D., and Claudia Baldassano, M.D. (University of Pennsylvania Medical Center); Michael E. Thase, M.D., and Edward S. Friedman, M.D. (University of Pittsburgh Western Psychiatric Institute and Clinic); and Charles L. Bowden, M.D., and Cheryl L. Gonzales, M.D. (University of Texas Health Science Center at San Antonio). Executive Committee: Mark S. Bauer, M.D., Charles L. Bowden, M.D., Joseph R. Calabrese, M.D., Jennifer Conley, M.A., Maurizio Fava, M.D., Gary Gottleib, M.D., Ellen Frank, Ph.D., Terence A. Ketter, M.D., Jane N. Kogan, Ph.D., David Kupfer, M.D., Leslie Leahy, Ph.D.*, Lauren B. Marangell, M.D., David J. Miklowitz, Ph.D., Michael W. Otto, Ph.D., Jerrold F. Rosenbaum, M.D., Matthew V. Rudorfer, M.D., Gary S. Sachs, M.D., Linda Street, Ph.D., Michael E. Thase, M.D., and Sean Ward. NIMH Liaisons: Matthew V. Rudorfer, M.D., Joanne Severe, M.S., and Linda Street, Ph.D.
*No longer participating in this role.
 |
 |
 |
Presented in part at the 41st annual meeting of the American College of Neuropsychopharmacology, San Juan, Puerto Rico, December 8–12, 2002; and the 156th annual meeting of the American Psychiatric Association, San Francisco, May 17–22, 2003. Received Sept. 5, 2002; revisions received July 3, July 28, and Dec. 17, 2003; accepted Jan. 9, 2004. From the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Address correspondence and reprint requests to Dr. Simon, Associate Director, Center for Anxiety and Traumatic Stress Related Disorders, Wang ACC 815, Massachusetts General Hospital, 15 Parkman St., Boston, MA 02114; [email protected] (e-mail). This project has been funded in whole or in part with federal funds from NIMH grant N01 MH-80001. Any opinions, findings, and conclusions or recommendations expressed in this publication are those of the authors and do not necessarily reflect the views of NIMH. This article was approved by the STEP-BD publication committee. Work on this project was supported by an NIMH Career Development Award (MH-01831-01) to Dr. Simon.

Figure 1. Longest Euthymic Period Within the Preceding 2 Years of 469 Bipolar Disorder Patients Enrolled in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD), by Comorbid Anxiety Diagnosisa
aAnalyses of difference are for each diagnosis versus no anxiety disorder diagnosis.
*p<0.05. **p<0.01. ***p<0.001. †p<0.0001.

Figure 2. History of Suicide Attempts in 469 Bipolar Disorder Patients Enrolled in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD), by Comorbid Anxiety Diagnosisa
aAnalyses of difference are for each diagnosis versus no anxiety disorder diagnosis.
*p<0.05. **p<0.01. ***p<0.001. †p<0.0001.
1. McElroy SL, Altshuler LL, Suppes T, Keck PE Jr, Frye MA, Denicoff KD, Nolen WA, Kupka RW, Leverich GS, Rochussen JR, Rush AJ, Post RM: Axis I psychiatric comorbidity and its relationship to historical illness variables in 288 patients with bipolar disorder. Am J Psychiatry 2001; 158:420–426Link, Google Scholar
2. Pini S, Dell’Osso L, Mastrocinque C, Marcacci G, Papasogli A, Vignoli S, Pallanti S, Cassano G: Axis I comorbidity in bipolar disorder with psychotic features. Br J Psychiatry 1999; 175:467–471Crossref, Medline, Google Scholar
3. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen H-U, Kendler KS: Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8–19Crossref, Medline, Google Scholar
4. Kessler RC, Rubinow DR, Holmes C, Abelson JM, Zhao S: The epidemiology of DSM-III-R bipolar I disorder in a general population survey. Psychol Med 1997; 27:1079–1089Crossref, Medline, Google Scholar
5. Young LT, Cooke RG, Robb JC, Levitt AJ, Joffe RT: Anxious and non-anxious bipolar disorder. J Affect Disord 1993; 29:49–52Crossref, Medline, Google Scholar
6. Dilsaver SC, Chen YW, Swann AC, Shoaib AM, Tsai-Dilsaver Y, Krajewski KJ: Suicidality, panic disorder and psychosis in bipolar depression, depressive-mania and pure-mania. Psychiatry Res 1997; 73:47–56Crossref, Medline, Google Scholar
7. Chen Y-W, Dilsaver SC: Comorbidity of panic disorder in bipolar illness: evidence from the Epidemiologic Catchment Area survey. Am J Psychiatry 1995; 152:280–282Link, Google Scholar
8. Cassano GB, Pini S, Saettoni M, Dell’Osso L: Multiple anxiety disorder comorbidity in patients with mood spectrum disorders with psychotic features. Am J Psychiatry 1999; 156:474–476Link, Google Scholar
9. Feske U, Frank E, Mallinger AG, Houck PR, Fagiolini A, Shear MK, Grochocinski VJ, Kupfer DJ: Anxiety as a correlate of response to the acute treatment of bipolar I disorder. Am J Psychiatry 2000; 157:956–962Link, Google Scholar
10. Frank E, Cyranowski JM, Rucci P, Shear MK, Fagiolini A, Thase ME, Cassano GB, Grochocinski VJ, Kostelnik B, Kupfer DJ: Clinical significance of lifetime panic spectrum symptoms in the treatment of patients with bipolar I disorder. Arch Gen Psychiatry 2002; 59:905–911Crossref, Medline, Google Scholar
11. Sachs G, Thase ME, Otto MW, Bauer M, Miklowitz D, Wisniewski SR, Lavori P, Lebowitz B, Rudorfer M, Frank E, Nierenberg AA, Fava M, Bowden C, Ketter T, Marangell L, Calabrese J, Kupfer D, Rosenbaum JF: Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003; 53:1028–1042Crossref, Medline, Google Scholar
12. First MB, Spitzer RL, Gibbon M, Williams JBW: Structured Clinical Interview for DSM-IV Axis I Disorders (SCID). New York, New York State Psychiatric Institute, Biometrics Research, 1996Google Scholar
13. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC: The Mini-International Neuropsychiatric Interview (MINI): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998; 59(suppl 20):22–33Google Scholar
14. Endicott J, Nee J, Harrison W, Blumenthal R: Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol Bull 1993; 29:321–326Medline, Google Scholar
15. Leon AC, Solomon DA, Mueller TI, Endicott J, Posternak M, Judd LL, Schettler PJ, Akiskal HS, Keller MB: A brief assessment of psychosocial functioning of subjects with bipolar I disorder: the LIFE-RIFT: Longitudinal Interval Follow-Up Evaluation-Range Impaired Functioning Tool. J Nerv Ment Dis 2000; 188:805–812Crossref, Medline, Google Scholar
16. Regier DA, Narrow WE, Rae DS: The epidemiology of anxiety disorders: the Epidemiologic Catchment Area (ECA) experience. J Psychiatr Res 1990; 24(suppl 2):3–14Google Scholar
17. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB: Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995; 52:1048–1060Crossref, Medline, Google Scholar
18. Perugi G, Akiskal HS, Ramacciotti S, Nassini S, Toni C, Milanfranchi A, Musetti L: Depressive comorbidity of panic, social phobic, and obsessive-compulsive disorders re-examined: is there a bipolar II connection? J Psychiatr Res 1999; 33:53–61Crossref, Medline, Google Scholar
19. Himmelhoch JM: Social anxiety, hypomania and the bipolar spectrum: data, theory and clinical issues. J Affect Disord 1998; 50:203–213Crossref, Medline, Google Scholar
20. Goodwin RD, Hamilton SP, Milne BJ, Pine DS: Generalizability and correlates of clinically derived panic subtypes in the population. Depress Anxiety 2002; 15:69–74Crossref, Medline, Google Scholar
21. Johnson JG, Cohen P, Brook JS: Associations between bipolar disorder and other psychiatric disorders during adolescence and early adulthood: a community-based longitudinal investigation. Am J Psychiatry 2000; 157:1679–1681Link, Google Scholar
22. Rotondo A, Mazzanti C, Dell’Osso L, Rucci P, Sullivan P, Bouanani S, Gonnelli C, Goldman D, Cassano GB: Catechol O–methyltransferase, serotonin transporter, and tryptophan hydroxylase gene polymorphisms in bipolar disorder patients with and without comorbid panic disorder. Am J Psychiatry 2002; 159:23–29Link, Google Scholar
23. MacKinnon DF, Zandi PP, Cooper J, Potash JB, Simpson SG, Gershon E, Nurnberger J, Reich T, DePaulo JR: Comorbid bipolar disorder and panic disorder in families with a high prevalence of bipolar disorder. Am J Psychiatry 2002; 159:30–35Link, Google Scholar
24. Myers JE, Thase ME: Anxiety in the patient with bipolar disorder: recognition, significance, and approaches to treatment. Psychiatr Annals 2000; 30:456–464Crossref, Google Scholar
25. Fawcett J, Scheftner WA, Fogg L, Clark DC, Young MA, Hedeker D, Gibbons R: Time-related predictors of suicide in major affective disorder. Am J Psychiatry 1990; 147:1189–1194Link, Google Scholar
26. Gray SM, Otto MW: Psychosocial approaches to suicide prevention: applications to patients with bipolar disorder. J Clin Psychiatry 2001; 62(suppl 25):56–64Google Scholar
27. Berkson S: Limitations of the application of fourfold table analysis to hospital data. Biometrics Bulletin 1946; 2:47–53Crossref, Google Scholar

