
Unmet Need for Mental Health Care Among U.S. Children: Variation by Ethnicity and Insurance Status
Abstract
OBJECTIVE: Policy discussions regarding the mental health needs of children and adolescents emphasize a lack of use of mental health services among youth, but few national estimates are available. The authors use three national data sets and examine ethnic disparities in unmet need (defined as having a need for mental health evaluation but not using any services in a 1-year period) to provide such estimates. METHOD: The authors conducted secondary data analyses in three nationally representative household surveys fielded in 1996–1998: the National Health Interview Survey, the National Survey of American Families, and the Community Tracking Survey. They determined rates of mental health service use by children and adolescents 3–17 years of age and differences by ethnicity and insurance status. Among the children defined as in need of mental health services, defined by an estimator of mental health problems (selected items from the Child Behavior Checklist), they examined the association of unmet need with ethnicity and insurance status. RESULTS: In a 12-month period, 2%–3% of children 3–5 years old and 6%–9% of children and adolescents 6–17 years old used mental health services. Of children and adolescents 6–17 years old who were defined as needing mental health services, nearly 80% did not receive mental health care. Controlling for other factors, the authors determined that the rate of unmet need was greater among Latino than white children and among uninsured than publicly insured children. CONCLUSIONS: These findings reveal that most children who need a mental health evaluation do not receive services and that Latinos and the uninsured have especially high rates of unmet need relative to other children. Rates of use of mental health services are extremely low among preschool children. Research clarifying the reasons for high rates of unmet need in specific groups can help inform policy and clinical programs.
It is estimated that one of every five children and adolescents in the United States has a mental disorder (1–3); left untreated, these disorders are often debilitating (4–7). Empirically validated treatments exist for many mental disorders, including attention deficit hyperactivity disorder (ADHD), conduct disorder, mood disorders, and anxiety disorders (4–9). However, recent health policy discussions concerning the mental health needs of children and adolescents have been limited by the lack of national data on rates of mental health service use and unmet need for such services (10).
Populations that may be particularly vulnerable to lower rates of use of mental health services include ethnic minority youth and the uninsured. Previous studies on child mental health service use have largely been based on regional data or data from insured populations and have yielded a mixed pattern of results regarding possible disparities in service use. For example, in a sample of children in New Haven, Conn. (11), African American and Latino children had lower rates of mental health service use than did Caucasian children. A study of a group of insured children (12) found lower rates of service use for African American but not Latino children than for white children. However, in the Great Smoky Mountains Study (13), African American children did not differ from Caucasian children in service use. How insurance status affects use of child mental health services is also unclear (14, 15).
Recent national studies of adults (16, 17) suggest that, compared with whites, African Americans have lower rates of access, African Americans and Latinos with mental health or substance abuse problems have lower rates of active treatment, and African Americans have lower rates of appropriate care for depressive or anxiety disorders. In addition, uninsured adults have lower rates of access to mental health care and lower rates of active treatment for mental health or substance abuse problems than insured adults (18).
To study rates of use and unmet need for children and adolescents in the United States, we primarily used data from the National Survey of American Families, a large nationally representative sample, and attempted when possible to confirm findings across several national data sets. We hypothesized that the rate of overall mental health service use for children is low and that most children who need a mental health evaluation do not receive any services (our definition of unmet need). In addition, we hypothesized that minority and uninsured children have greater rates of unmet need for a mental health evaluation than their white and insured counterparts.
Method
Data Sources
We provide separate cross-sectional analyses of three nationally representative household samples of U.S. civilian, noninstitutionalized children 3–17 years old. Full descriptions of the study designs are available elsewhere (19–21). Because methods differ across surveys, we examined rates of use and ethnic and insurance status within each survey and then considered the consistency of conclusions across data sets. The main data set for this study is the National Survey of American Families (19), with supporting analyses from the National Health Interview Survey (20) and the Community Tracking Survey (21) when applicable.
The main data set for the study, the 1997 National Survey of American Families (19, 22, 23), sampled more than 44,000 households and 28,867 children, with larger shares of the sample from 13 states that account for more than half of the U.S. population and a smaller sample of the balance of the nation to permit national estimates. The most knowledgeable adult in the household (95% were parents) provided information about the sampled child, but emancipated minors provided their own information. The survey oversampled people with low incomes. Interviews were conducted in Spanish and English. The response rate was 65.4%.
The 1998 National Health Interview Survey (20) sampled 38,209 households, including 11,017 children, using a multistage stratified cluster design and oversampling African Americans and Latinos. A knowledgeable adult in the household provided information about the randomly selected child. The response rate was 82.4%. The 1996–1997 Community Tracking Survey (21) sampled 32,732 family insurance units, which included 8,852 children and adolescents aged 3–17. Sixty sites were randomly selected on the basis of metropolitan statistical areas, and sites were stratified by region and size. Households were randomly selected. To increase the precision of the national estimates, a smaller supplemental sample was included in this survey that randomly selected households from the 48 continental United States. An adult informant from each family insurance unit provided information about the randomly selected child. Interviews were conducted in English and Spanish. The overall response rate was 65.0%.
Outcome Measures
Each survey elicited information on use of child mental health services over the preceding 12 months. For each data set, we derived a dichotomous variable indicating whether the child had received any mental health care. The National Survey of American Families respondents were asked how many times the child had received mental health services from a doctor, mental health counselor, or therapist, excluding visits for smoking cessation and treatment for substance abuse. The National Health Interview Survey asked whether the adult respondent had seen or talked to a mental health professional about the child. The Community Tracking Survey asked if the child had received any care from a mental health professional.
Children were categorized as having unmet need if they had exceeded a cutoff point on a mental health screening measure (described later in this article) but had not received any mental health services in the past 12 months. Need was not measured in the Community Tracking Survey.
Main Independent Variables
The adult respondent reported the race of each child, which was categorized as white, black, Hispanic, or other; the white and black groups excluded subjects of Hispanic background.
The National Survey of American Families defined current child health insurance coverage as public insurance (Medicaid, Medicare, military insurance, and Indian Health Service insurance), private insurance (employment related or directly purchased), or no insurance. We grouped the National Health Interview Survey and Community Tracking Survey data into similar categories. For children with multiple coverages, a hierarchy was used to assign a child to the applicable category (private insurance, then public insurance, followed by no insurance). Whether a child’s health insurance included mental health coverage was not elicited in the surveys.
The measure that estimates need for a mental health evaluation, included in both the National Survey of American Families and the National Health Interview Survey, is the Mental Health Indicator (24), which comprises selected items from the Child Behavior Checklist (25). The original Child Behavior Checklist is a standardized questionnaire of parent-rated child behavior over the preceding 6 months. Child Behavior Checklist items that best discriminated between demographically similar children who were or were not referred for mental health services were chosen for inclusion in the Mental Health Indicator, which is thus a measure of the need for clinical evaluation. The Mental Health Indicator includes four age- and gender-specific items from the Child Behavior Checklist rated on a scale of 0, 1, or 2, for a total possible score of 8; higher scores represent greater need.
Validation of the Mental Health Indicator was based on receiver operator characteristic analysis of Mental Health Indicator scores compared with external criteria such as a lifetime history of ADHD, mental retardation, learning disability, and past use of mental health services (26). The recommended cutoff point for defining a level of need meriting evaluation is a score of 2, but to avoid concerns about overinclusion of minor or transient symptoms, we relied on a more stringent criterion of 3 or higher for analyses of unmet need, with specificity ranging from 88% to 90% for each age-gender category (26). Mental Health Indicator scores are available in the National Health Interview Survey for children 4 and older and in the National Survey of American Families for children 6 and older. The Community Tracking Survey has no child mental health need indicator, so we used the Community Tracking Survey to describe rates of services use only.
Demographic and Parent Characteristic Variables
Demographic information included the child’s age and gender and the household income. The U.S. Census poverty ratio was used to assess total family income in each data set. Poor was defined as a ratio below 1.0, indicating that the family income was below the poverty level. In the National Health Interview Survey, this information was missing for 20% of the children, but we imputed the variable using other sociodemographic information.
The designations of West, South, Midwest, and Northeast for regional location were based on the U.S. Census statistical groupings (27).
The adult’s level of education was categorized as less than high school, high school, some college, or 4 or more years of post-high-school education. Household composition was defined as single-parent household or non-single-parent household. Emancipated minors (0.2% of the youth) were grouped with non-single-parent households for analyses. Mental health functioning of the adult respondent was determined by using the five-item Mental Health Inventory (28), which assesses psychological well-being in adults. Scores on this instrument range from 25 to 100, and higher scores indicate better mental health. A cutoff of 67 or below indicates poor mental health, approximately the lowest 20% of the general population (29).
Statistical Analysis
Descriptive analyses of service use by age group, ethnicity, and insurance status were conducted for each data set separately. We used statistical tests appropriate for the complex sampling design of each data set. We used a modified Pearson’s chi-square statistic (30) to test the independence of two categorical variables in the National Survey of American Families data, and a Wald statistic (31) was used to test independence for each two-way table in the National Health Interview Survey and Community Tracking Survey data. For each data set, standard errors of individual coefficients were calculated by using a jackknife replication method (32), which took into account the complex weighting schemes.
We used logistic regression in both the National Survey of American Families and the National Health Interview Survey for the unadjusted analyses of unmet need, which estimated the probability of having no mental health care in a year for those children 6–17 years old who met criteria for need (Mental Health Indicator score of 3 or higher). To examine the effect of race and insurance characteristics on unmet need while controlling for other factors, we performed multiple logistic regression using only the main data set, the National Survey of American Families. Following the Aday and Andersen health service model (33), we included covariates shown in previous studies (11, 12, 15, 34–39) to be significantly associated with service use such as predisposing factors (age, gender, race, parental education, single-parent household, parental mental health), enabling resources (income, insurance, and regional location), and child’s mental health need.
Statistical analyses were performed by using WesVar software (40) for the National Survey of American Families and SUDAAN software (41) for the National Health Interview Survey and Community Tracking Survey. All estimates are weighted to be nationally representative.
Results
Prevalence of Mental Health Service Use and Need
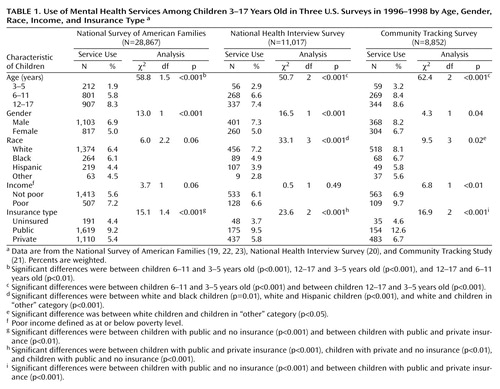
For children aged 3–17, the rate of having any mental health service use varied from 6.0% (both National Survey of American Families and National Health Interview Survey) to 7.5% (Community Tracking Survey) (data not shown). Rates were lower for preschool children (2%–3% for children 3–5 years old) (Table 1). Across data sets, a higher percentage of children with public insurance used services (9%–13%) than did the uninsured (4%–5%) and privately insured (5%–7%) children. In these unadjusted analyses, ethnic minority status was significantly associated with lower rates of use in the Community Tracking Survey and National Health Interview Survey data sets, but not in the National Survey of American Families data. Across data sets, male children had higher rates of mental health use than did female children.
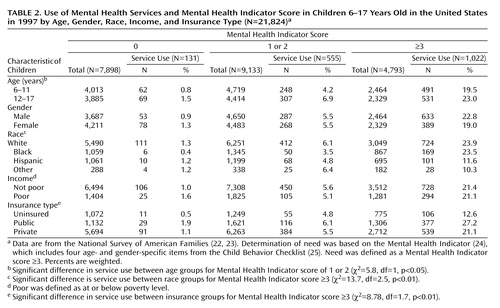
Table 2 shows the use of mental health services among children with different levels of need for these services. The weighted percentage of 6–17-year-olds with mental health problems was 15.2% in the National Health Interview Survey (1,350 out of 8,679) and 20.8% in the National Survey of American Families (4,793 out of 21,260). Data from the National Survey of American Families showed that greater levels of mental health need were associated with higher rates of having any mental health care among children 6–17 years old: 2% of youth with a Mental Health Indicator score of 0, 6% with scores of 1 or 2, and 21% with scores of 3 or greater used mental health services (χ2=151.014, df=1.3, p<0.001) (data not shown). The National Health Interview Survey had similar associations between level of need and service use: 1.6% of youth with a Mental Health Indicator score of 0, 8.3% with scores of 1 or 2, and 24.8% with scores of 3 or greater used mental health services (χ2=332.35, df=2, p<0.000) (data not shown).
Weighed estimates of unmet need for children under age 6 were available only in the National Health Interview Survey. Of 1,499 children 4–5 years old, 131 (8.5%) were estimated to have mental health problems, but of the 131 children in need, only nine (6.0%) used any mental health services in the preceding year.
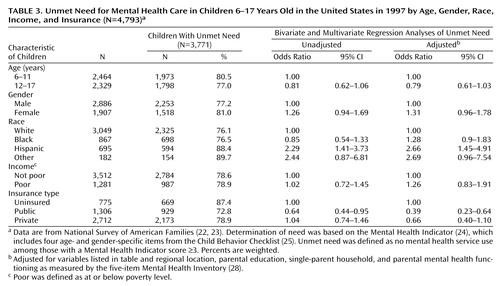
Among children 6–17 years old in the National Survey of American Families estimated to have need (Mental Health Indicator score ≥3), 79% had not used mental health services in the past 12 months (data not shown). A higher percentage of Hispanic children in need (88%) than white children in need (76%) did not receive care (Table 3). In addition, a higher percentage of uninsured children (87%) than those with public insurance (73%) received no care (Table 3). Likewise, in the National Health Interview Survey, 75% of children who had mental health problems had not received services: 80% of blacks, 82% of Hispanics, and 72% of whites had unmet need (χ2=14.6, df=3, p<0.01) (data not shown). Fewer children with public or private insurance than uninsured children had unmet need (χ2=38.0, df=2, p<0.001).
After adjusting for other demographic factors and parent characteristics and using multiple logistic regression with the National Survey of American Families data only, we found that Hispanic children with mental health problems had greater odds of having no care, or unmet need, than white children (odds ratio=2.66) (Table 3). The adjusted odds of having unmet need were significantly lower for the publicly insured than for uninsured children (odds ratio=0.39) (Table 3), but there was no significant difference in unmet need between uninsured and privately insured children.
Discussion
To our knowledge, this study is the first to provide national estimates of use of child mental health services and the unmet need for such services. Overall, the data suggest that 6.0%–7.5% of U.S. children receive mental health services, a result confirmed across three data sets. We also found that most children and adolescents who need a mental health evaluation do not get any mental health care in a year, and this was more pronounced for Latinos and the uninsured. “Need” in this study is based on a screening measure that estimates need for clinical evaluation, not necessarily indicating that treatment or intensive services are warranted. Nevertheless, we applied a more stringent cutoff point than recommended for these national surveys specifically to avoid concerns that we would comment on high unmet need for a group largely consisting of milder cases of need.
Another issue is whether we could have underestimated levels of use or need being met because of the brief utilization question in these surveys and emphasis on specialty mental health services. Although this is a general estimate of service use for mental health problems, the service use item in one survey did encompass primary care and nonpsychiatric care for mental health problems, yet conclusions were similar about levels of use and unmet need across data sets even though they differed in methodology. In addition, even if the rate of overall unmet need is somewhat lower, there is no reason to assume that comparative estimates of use or unmet need (i.e., across ethnic groups) are biased.
With these caveats in mind, we found that only 21% of the children who need a mental health evaluation receive services. This suggests that about 7.5 million children have an unmet need for mental health services in the United States, largely confirming findings from others (37). At a time of continuing concern over the high costs of health care, including mental health care, it may be difficult to focus national policy debates on the implications of such a high rate of unmet need among children. However, the implications for children and adolescents with untreated mental health problems can have major developmental consequences. For example, longitudinal studies have found that depressed children are at greater risk for later suicidal behavior, poor academic functioning, substance abuse, and unemployment (42), necessitating improvement in access to effective mental health prevention and early intervention for youth and their families.
Our finding that Latino children have even greater rates of unmet need than white children is particularly concerning given the national estimates suggesting that Latino adolescents have higher rates of suicidal thoughts, depression, and anxiety symptoms and greater rates of dropping out of high school than white adolescents (43). As described in the Surgeon General’s Report on Mental Health: Culture, Race, and Ethnicity (44), services could be improved for Latinos by dealing with barriers such as financial constraints and lack of bilingual bicultural mental health providers. In examining birthplace of parent, we found that unmet need did not significantly differ between children with non-U.S.-born parents (N=79, 93%) and those with U.S.-born parents (N=515, 88%) (χ2=1.42, df=1, p>0.05).
Additional research is needed to clarify the mechanisms underlying disparities in unmet need for mental health care among children because these different mechanisms have unique intervention and policy implications. For example, differences in parental attitudes may require educational interventions, but community differences in service availability require policy targeted at developing resources. Although Latino children had the highest rates of unmet need, the rates for white children were also quite high, emphasizing the general conclusion that there is a high rate of unmet need nationally for mental health care among children and adolescents.
We also found that uninsured children had higher rates of unmet need than publicly insured children, suggesting that Medicaid and other public insurance programs offer an important safety net, but we cannot comment as to whether the uninsured children in these studies were eligible for but not enrolled in public programs such as Medicaid or the State Children’s Health Insurance Program. Expanding insurance coverage to currently uninsured children, as proposed by the State Children’s Health Insurance Program (45), could be an important avenue for addressing unmet need (46). However, implementation of the State Children’s Health Insurance Program has been variable across states (47), with lower enrollment among black and Hispanic children than among white children (48). Our findings for children differ from those found in adults (18), in which the uninsured had less access than the privately insured, but the lower differences by insurance status among children could be partly due to the high level of unmet need across insurance groups among children.
We provide only a first sketch of national mental health care among preschoolers, who are referred most often for behavioral problems such as aggression, defiance, and overactivity (49, 50). Our descriptive findings suggest that the vast majority of preschool children with mental health needs in the United States do not receive services for those problems. The more talked-about public concern is the high rate of psychotropic medication use in young children (51, 52), but an even greater problem may be the lack of any evaluation or care for children with mental health problems. Further research is needed to confirm these findings on larger samples of young children and to determine whether unmet need is due to parent preference, unavailability of services, or problems in recognizing problems or identifying specialists for this age group (53).
As we have suggested, this study is limited by the use of parent-reported screening measures of need and service use; national studies using diagnostic measures for specific childhood disorders, level of impairment, and type and quality of service use are needed. In addition, only noninstitutionalized children were surveyed, which excludes those living in out-of-home placements and the homeless, who may have higher rates of mental health need than the general population (54–56). However, our overall estimate of unmet need is similar to estimates based on diagnostic measures (37), and our findings concerning the use of services were consistent across three independent national data sets.
This study reinforces the finding of the recent Surgeon General’s report (10) that there is substantial unmet need for child mental health care in the United States, which is particularly acute for some minority and uninsured groups.
 |
 |
 |
Presented at the Robert Wood Johnson Clinical Scholars Program 2000 National Meeting, Fort Lauderdale Fla., Nov. 8–11, 2000. Received Oct. 9, 2001; revision received April 15, 2002; accepted May 8, 2002. From the Department of Psychiatry and Biobehavioral Sciences, Child and Adolescent Psychiatry Division, and the Research Center on Managed Care for Psychiatric Disorders, University of California, Los Angeles; and RAND, Santa Monica, Calif. Address reprint requests to Dr. Kataoka, UCLA Health Services Research Center, 10920 Wilshire Blvd., Suite 300, Los Angeles, CA 90024; [email protected] (e-mail). Funded by the Robert Wood Johnson Foundation Healthcare for Communities grant 031280 and Clinical Scholars Program grant 037098 and by NIMH grant MH-01170 from the Research Center on Managed Care for Psychiatric Disorders. The authors thank Ruth Klap, Ph.D., Arlene Fink, Ph.D., and Bonnie Zima, M.D., M.P.H., for their reviews of this article; Susan Stockdale, Ph.D., for assistance with a previous version; and Lingqi Tang, Ph.D., and Naihua Duan, Ph.D., for statistical assistance.
1. Bird HR, Canino G, Rubio-Stipec M, Gould MS, Ribera J, Sesman M, Woodbury M, Huertas-Goldman S, Pagan A, Sanchez-Lacay A, Moscoso M: Estimates of the prevalence of childhood maladjustment in a community survey in Puerto Rico: the use of combined measures. Arch Gen Psychiatry 1988; 45:1120-1126; correction, 1994; 51:429Google Scholar
2. Costello EJ, Angold A, Burns BJ, Stangl DK, Tweed DL, Erkanli A, Worthman CM: The Great Smoky Mountains Study of Youth: goals, design, methods, and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry 1996; 53:1129-1136Crossref, Medline, Google Scholar
3. Offord DR, Boyle MH, Szatmari P, Rae-Grant NI, Links PS, Cadman DT, Byles JA, Crawford JW, Blum HM, Byrne C, Thomas H, Woodward CA: Ontario Child Health Study, II: six-month prevalence of disorder and rates of service utilization. Arch Gen Psychiatry 1987; 44:832-836Crossref, Medline, Google Scholar
4. Dulcan M (American Academy of Child and Adolescent Psychiatry): Practice parameters for the assessment and treatment of children, adolescents, and adults with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 1997; 36(10 suppl):85S-121SGoogle Scholar
5. Birmaher B, Brent D (American Academy of Child and Adolescent Psychiatry): Practice parameters for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry 1998; 37(10 suppl):63S-83SGoogle Scholar
6. Bernstein GA, Shaw K (American Academy of Child and Adolescent Psychiatry): Practice parameters for the assessment and treatment of children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 1997; 36(10 suppl):69S-84SGoogle Scholar
7. Steiner H (American Academy of Child and Adolescent Psychiatry): Practice parameters for the assessment and treatment of children and adolescents with conduct disorder. J Am Acad Child Adolesc Psychiatry 1997; 36(10 suppl):122S-139SGoogle Scholar
8. Brestan EV, Eyberg SM: Effective psychosocial treatments of conduct-disordered children and adolescents: 29 years, 82 studies, and 5,272 kids. J Clin Child Psychol 1998; 27:180-189Crossref, Medline, Google Scholar
9. Pelham WE Jr, Wheeler T, Chronis A: Empirically supported psychosocial treatments for attention deficit hyperactivity disorder. J Clin Child Psychol 1998; 27:190-205Crossref, Medline, Google Scholar
10. Report of the Surgeon General’s Conference on Children’s Mental Health: A National Action Agenda. Washington, DC, Department of Health and Human Services, US Public Health Service, 2000Google Scholar
11. Zahner GE, Daskalakis C: Factors associated with mental health, general health, and school-based service use for child psychopathology. Am J Public Health 1997; 87:1440-1448Crossref, Medline, Google Scholar
12. Padgett DK, Patrick C, Burns BJ, Schlesinger HJ, Cohen J: The effect of insurance benefit changes on use of child and adolescent outpatient mental health services. Med Care 1993; 31:96-110Crossref, Medline, Google Scholar
13. Burns BJ, Costello EJ, Angold A, Tweed D, Stangl D, Farmer EM, Erkanli A: Children’s mental health service use across service sectors. Health Aff (Millwood) 1995; 14:147-159Crossref, Medline, Google Scholar
14. Glied S, Hoven CW, Moore RE, Garrett AB, Regier DA: Children’s access to mental health care: does insurance matter? Health Aff (Millwood) 1997; 16:167-174Crossref, Medline, Google Scholar
15. Burns BJ, Costello AJ, Erkanli A, Tweed DL, Farmer EM, Angold A: Insurance coverage and mental health service use by adolescents with serious emotional disturbance. J Child and Family Studies 1997; 6:89-111Crossref, Google Scholar
16. Wells K, Klap R, Koike A, Sherbourne C: Ethnic disparities in unmet need for alcoholism, drug abuse, and mental health care. Am J Psychiatry 2001; 158:2027-2032Link, Google Scholar
17. Young AS, Klap R, Sherbourne CD, Wells KB: The quality of care for depressive and anxiety disorders in the United States. Arch Gen Psychiatry 2001; 58:55-61Crossref, Medline, Google Scholar
18. Wells KB, Sherbourne CD, Sturm R, Young A, Burnam M: Profiles of care for alcohol, drug abuse, and mental health problems for uninsured and insured adults. Health Serv Res (in press)Google Scholar
19. Dean Brick P, Kenney G, McCullough-Harlin R, Rajan S, Scheuren F, Wang K, Brick JM, Cunningham P: Report Number 1:1997 National Survey of America’s Families: Survey Methods and Data Reliability. Washington, DC, Urban Institute, 1999Google Scholar
20. National Center for Health Statistics: Data File Documentation, National Health Interview Survey, 1998 (machine readable data file and documentation). Hyattsville, Md, National Center for Health Statistics, 2000Google Scholar
21. Center for Studying Health System Change: Community Tracking Study Household Survey, 1996-1997: United States, ICPSR Version (computer file). Washington, DC, Center for Studying Health System Change, Inter-University Consortium for Political and Social Research, 1998Google Scholar
22. Wigton A, Scheuren F, Wenck S, Zhang H, Nooter D, Smith W: 1997 NSAF Child Public Use File Documentation and Codebook With Undercount Adjusted Weights:1997 National Survey of America’s Families Methodology Reports, Number 17. Washington, DC, Urban Institute, 2000Google Scholar
23. McCullough-Harlin R, Russell B, Safir A, Scheuren F, Wigton A, Zhang H, Nooter D, Cohen E, Smith W: 1997 NSAF MKA Public Use File Documentation and Codebook With Undercount Adjusted Weights:1997 National Survey of America’s Families Methodology Reports, Number 18. Washington, DC, Urban Institute, 2000Google Scholar
24. Ehrle J, Moore K: Report Number 6: Benchmarking Child and Family Well-Being Measures in the NSAF. Washington, DC, Urban Institute, 1999Google Scholar
25. McConaughy SH, Achenbach TM: Practical Guide for the Child Behavior Checklist and Related Materials. Burlington, University of Vermont, Department of Psychiatry, 1988Google Scholar
26. Data File Documentation, National Health Interview Survey, 1998: Mental Health Indicator (MHI) Appendices 1-5. Hyattsville, Md, National Center for Health Statistics, 2000Google Scholar
27. Geographical Areas Reference Manual. Washington, DC, Bureau of the Census, 2000Google Scholar
28. Berwick DM, Murphy JM, Goldman PA, Ware JE Jr, Barsky AJ, Weinstein MC: Performance of a five-item mental health screening test. Med Care 1991; 29:169-176Crossref, Medline, Google Scholar
29. Stewart AL, Hays RD, Ware JE Jr: The MOS Short-Form General Health Survey: reliability and validity in a patient population. Med Care 1988; 26:724-735Crossref, Medline, Google Scholar
30. Rao JNK, Scott AJ: The analysis of categorical data from complex sample surveys: chi-squared tests for goodness of fit and independence in two-way tables. J Am Statistical Assoc 1981; 76:221-230Crossref, Google Scholar
31. Koch GG, Freeman DH, Freeman JL: Strategies in the multivariate analysis of data from complex surveys. Int Statistical Rev 1975; 43:59-78Crossref, Google Scholar
32. Kish L, Frankel MR: Inferences from complex samples. J R Statistical Society 1974; 36:1-37Google Scholar
33. Aday LA, Andersen R: A framework for the study of access to medical care. Health Serv Res 1974; 9:208-220Medline, Google Scholar
34. Horgan CM: Specialty and general ambulatory mental health services: comparison of utilization and expenditures. Arch Gen Psychiatry 1985; 42:565-572Crossref, Medline, Google Scholar
35. Verhulst FC, van der Ende J: Factors associated with child mental health service use in the community. J Am Acad Child Adolesc Psychiatry 1997; 36:901-909Crossref, Medline, Google Scholar
36. Jensen PS, Bloedau L, Davis H: Children at risk, II: risk factors and clinic utilization. J Am Acad Child Adolesc Psychiatry 1990; 29:804-812Crossref, Medline, Google Scholar
37. Flisher AJ, Kramer RA, Grosser RC, Alegria M, Bird HR, Bourdon KH, Goodman SH, Greenwald S, Horwitz SM, Moore RE, Narrow WE, Hoven CW: Correlates of unmet need for mental health services by children and adolescents. Psychol Med 1997; 27:1145-1154Crossref, Medline, Google Scholar
38. Farmer EM, Stangl DK, Burns BJ, Costello EJ, Angold A: Use, persistence, and intensity: patterns of care for children’s mental health across one year. Community Ment Health J 1999; 35:31-46Crossref, Medline, Google Scholar
39. Zahner GE, Pawelkiewicz W, DeFrancesco JJ, Adnopoz J: Children’s mental health service needs and utilization patterns in an urban community: an epidemiological assessment. J Am Acad Child Adolesc Psychiatry 1992; 31:951-960Crossref, Medline, Google Scholar
40. WesVar: WesVar Complex Sample 4.0 User’s Guide. Rockville, Md, Westat, 2000Google Scholar
41. SUDAAN: Professional Software for Survey Data Analysis, Version 7.5. Research Triangle Park, NC, Research Triangle Institute, 1997Google Scholar
42. Fergusson DM, Woodward LJ: Mental health, educational, and social role outcomes of adolescents with depression. Arch Gen Psychiatry 2002; 59:225-231Crossref, Medline, Google Scholar
43. Centers for Disease Control and Prevention: Youth Risk Behavior Surveillance—United States, 1999. MMWR Morb Mortal Wkly Rep 2000; 49:1-96Medline, Google Scholar
44. Mental Health: Culture, Race, and Ethnicity: A Supplement to Mental Health: A Report of the Surgeon General. Rockville, Md, US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, 2001Google Scholar
45. US Department of Health and Human Services: State Child Health: State Children’s Health Insurance Program Allotments and Payments to States: Health Care Financing Administration (HCFA) Final Rule. Federal Register 2000; 65(101):33616-33633Google Scholar
46. American Academy of Pediatrics: Insurance coverage of mental health and substance abuse services for children and adolescents: a consensus statement. Pediatrics 2000; 106:860-862Crossref, Medline, Google Scholar
47. Long SH, Marquis MS: Geographic variation in physician visits for uninsured children: the role of the safety net. JAMA 1999; 281:2035-2040Crossref, Medline, Google Scholar
48. Szilagyi PG, Holl JL, Rodewald LE, Shone LP, Zwanziger J, Mukamel DB, Trafton S, Dick AW, Raubertas RF: Evaluation of children’s health insurance: from New York State’s Child Health Plus to SCHIP. Pediatrics 2000; 105(3 suppl E):687-691Google Scholar
49. Campbell SB: Behavior Problems in Preschool Children: Clinical and Developmental Issues. New York, Guilford, 1990Google Scholar
50. Lavigne JV, Arend R, Rosenbaum D, Binns HJ, Christoffel KK, Gibbons RD: Psychiatric disorders with onset in the preschool years, I: stability of diagnoses. J Am Acad Child Adolesc Psychiatry 1998; 37:1246-1254Crossref, Medline, Google Scholar
51. Minde K: The use of psychotropic medication in preschoolers: some recent developments. Can J Psychiatry 1998; 43:571-575Crossref, Medline, Google Scholar
52. Zito JM, Safer DJ, dosReis S, Gardner JF, Boles M, Lynch F: Trends in the prescribing of psychotropic medications to preschoolers. JAMA 2000; 283:1025-1030Crossref, Medline, Google Scholar
53. Lavigne JV, Arend R, Rosenbaum D, Binns HJ, Christoffel KK, Burns A, Smith A: Mental health service use among young children receiving pediatric primary care. J Am Acad Child Adolesc Psychiatry 1998; 37:1175-1183Crossref, Medline, Google Scholar
54. Litrownick AJ, Taussig HN, Landsverk JA, Garland AF: Youth entering an emergency shelter care facility: prior involvement in juvenile justice and mental health systems. J Soc Serv Res 1999; 25:5-19Crossref, Google Scholar
55. Pliszka SR, Sherman JO, Barrow MV, Irick S: Affective disorder in juvenile offenders: a preliminary study. Am J Psychiatry 2000; 157:130-132Link, Google Scholar
56. Zima BT, Wells KB, Benjamin B, Duan N: Mental health problems among homeless mothers: relationship to service use and child mental health problems. Arch Gen Psychiatry 1996; 53:332-338Crossref, Medline, Google Scholar

