
A Comparison of Family Functioning, Temperament, and Childhood Conditions in Monozygotic Twin Pairs Discordant for Lifetime Bulimia Nervosa
Abstract
OBJECTIVE: The authors investigated differences between twins in nine pairs of female monozygotic twins in the Australian Twin Registry who were discordant for lifetime bulimia nervosa. METHOD: The twins affected and unaffected by lifetime bulimia nervosa were compared on self-report measures, including a measure of parental bonding, four measures of temperament, and six early-childhood medical conditions. RESULTS: No twins had current bulimia nervosa, and there was no difference in weight or eating status between the affected and unaffected twins. The affected twins reported significantly lower self-esteem and less warmth but more overprotection by their mothers during childhood. CONCLUSIONS: Although limited by the small number of discordant twin pairs and the inability to detect causal relationships, these results suggest that environmental influences that promote low self-esteem may also increase the risk for bulimia nervosa. These temperamental differences may explain the discrepancies in parenting or perceived parenting.
While bulimia nervosa has been shown to run in families (1), a phenomenon that is at least partly attributable to genetic influences (2), there remain many questions about the environmental influences that cause a person to express this genetic vulnerability. One approach that can be useful in the identification of environmental influences is studying monozygotic twins discordant for bulimia nervosa (3). Differences between these twins must necessarily be, in some way, the result of environmental influences, including prenatal influences (4).
We examined the differences between affected and unaffected twins in nine pairs of monozygotic twins discordant for a lifetime diagnosis of bulimia nervosa, in terms of reports of past family functioning, current temperament, and early-childhood conditions.
Method
The data are from a longitudinal study of 1,682 women in the volunteer Australian Twin Registry who were screened with a self-report health and lifestyle survey that included information about disordered eating. At the time of screening, in 1988–1989, they were between the ages of 30 and 45 years (mean=36.5, SD=4.7). These women were further interviewed over the telephone in 1992–1993 with a general semistructured psychiatric interview that included information about lifetime bulimia nervosa. The women indicating problems with eating from the first two waves of data were followed up during 1994–1995 and interviewed over the telephone more extensively about past history of bulimia nervosa, parental bonding, and temperament. Nine monozygotic twin pairs were found to be discordant for lifetime history of bulimia nervosa. The mean age of this group at the time of the third data collection was 40.3 years (SD=5.8), and their mean age at the first binge episode was 21.8 years (SD=7.3, range=16–38 years). Oral informed consent was obtained before the telephone interviews.
The wave 3 interview was performed with the Eating Disorder Examination (5), conducted by interviewers blind to information about the co-twins. The diagnostic questions of the Eating Disorder Examination were adapted to assess the presence of bulimia nervosa during the subject’s lifetime as well as over the previous 3 months. The Eating Disorder Examination also provides scores on four subscales, measuring dietary restraint, eating concern, weight concern, and shape concern over the previous 3 months. Other wave 3 measures included the Rosenberg Self-Esteem Scale (6), the subscale for dichotomous thinking style of the Dysfunctional Attitude Scale (7), and the “emotional reliance on another person” dimension of the Interpersonal Dependency Inventory (8) to measure external control. Warmth and overprotection from parents in the first 16 years of life was measured with the 25-item Parental Bonding Inventory (9), extensively used in the assessment of parental characteristics as influences on adjustment in adulthood (10). Scores on the Tridimensional Personality Questionnaire (11) were collected at wave 2, and information on birth weight, birth order (first born or second born), difficulties at birth, and six medical conditions before age 14 (migraine, hay fever, asthma, eczema, dust allergy, arthritis) was collected at wave 1. All wave 1 variables, with the exception of birth weight, were categorical.
Paired t tests were used for all continuous measures, and McNemar’s exact test was used for categorical variables. Given the clear directional hypotheses from the research literature, one-tailed significance was used for all t tests (with the exception of birth weight). All analyses were conducted by using SPSS for Unix, Release 6.1 (Chicago, SPSS).
Results
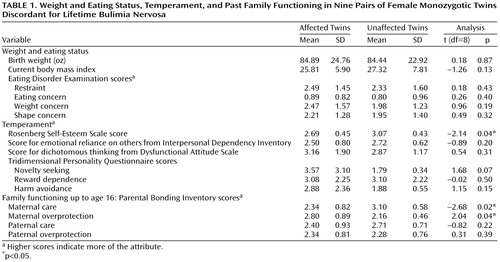
The results of the paired comparisons of the continuous variables are presented in Table 1. There was no significant difference in birth weight, body mass index, or current attitudes toward dieting or eating between the affected and unaffected twins, indicating that current eating problems were unlikely to affect the reporting of the other variables. All of the significant differences were in directions consistent with predictions from previous findings in the literature. The affected twins reported their mothers as being significantly less caring and significantly more overprotective in the first 16 years of their lives. In addition, the affected twins had significantly lower self-esteem than their nonaffected co-twins. Approaching significance was the score for novelty seeking from the Tridimensional Personality Questionnaire; the affected twins displayed higher levels of impulsivity, exploratory excitability, extravagance, and disorderliness. There was no significant difference in any of the categorical variables.
Discussion
This study must be interpreted as an exploratory investigation in the absence of correction for multiple testing due to our poor power. However, despite the small numbers of monozygotic twins discordant for bulimia nervosa in the Australian Twin Registry, we were able to observe some striking differences between the affected and unaffected twins. The twins affected by bulimia nervosa in the past displayed lower self-esteem and a tendency toward greater novelty seeking and reported experiencing less maternal care and more maternal overprotection while growing up.
While the correlations observed must be due to environmental factors, it is possible that these environmental factors either had an impact before the onset of bulimia nervosa or occurred after the onset of bulimia nervosa. The results are remarkably consistent with those from a study of risk factors for bulimia nervosa (12), which identified negative self-evaluation and parenting variables as distinguishing women with bulimia nervosa from psychiatric comparison subjects. Parental alcoholism, which is associated with impulsivity, was also identified as a risk factor. It may be that the experience of bulimia nervosa alters one’s perceptions of early parenting, the so-called “effort after meaning” effect, i.e., the search of past experiences by distressed people to find explanations of their distress (13). This experience may also influence the development of temperament.
Given that the mean age when these subjects developed binge eating was 21.8 years, by which time temperament is expected to be formed, alternative hypotheses can be suggested. Environmental influences that lead to low self-esteem and a high level of impulsivity may also either place a person at risk of being treated differently by her mother or lead to a different perception of the mothering she received while growing up. These same environmental influences may place a person at risk of developing bulimia nervosa in later life.
 |
Received Oct. 18, 2000; revision received Feb. 5, 2001; accepted March 8, 2001. From the School of Psychology, Flinders University of South Australia; and the Department of Epidemiology, Queensland Institute for Medical Research, Brisbane, Australia. Address reprint requests to Dr. Wade, School of Psychology, Flinders University of South Australia, G.P.O. Box 2100, Adelaide 5001, S.A., Australia; [email protected] (e-mail). Supported by a Flinders University Research Budget grant to Dr. Wade. The authors thank the twins for their participation in this research.
1. Lilenfeld LR, Kaye WH, Greeno CG, Merikangas KR, Plotnicov K, Pollice C, Rao R, Strober M, Bulik CM, Nagy L: A controlled study of anorexia nervosa and bulimia nervosa. Arch Gen Psychiatry 1998; 55:603-610Crossref, Medline, Google Scholar
2. Wade T, Martin NG, Neale MC, Tiggemann M, Treloar SA, Bucholz KK, Madden PAF, Heath AC: The structure of genetic and environmental risk factors for three measures of disordered eating. Psychol Med 1999; 29:925-934Crossref, Medline, Google Scholar
3. Bulik CM, Wade TD, Kendler KS: Characteristics of monozygotic twins discordant for bulimia nervosa. Int J Eat Disord 2001; 29:1-10Crossref, Medline, Google Scholar
4. Martin NG, Boomsma D, Machin G: A twin-pronged attack on complex traits. Nat Genet 1997; 17:387-392Crossref, Medline, Google Scholar
5. Fairburn CG, Cooper Z: The Eating Disorder Examination, 12th ed, in Binge Eating: Nature, Assessment and Treatment. Edited by Fairburn CG, Wilson GT. New York, Guilford Press, 1993, pp 317-360Google Scholar
6. Rosenberg M: Society and the Adolescent Self-Image. Princeton, NJ, Princeton University Press, 1965Google Scholar
7. Beck AT, Brown G, Steer RA, Weissman AN: Factor analysis of the Dysfunctional Attitude Scale in a clinical population. Psychol Assess 1991; 3:478-483Crossref, Google Scholar
8. Hirschfeld RM, Klerman GL, Gough HG, Barrett J, Korchin SJ, Chodoff P: A measure of interpersonal dependency. J Pers Assess 1977; 41:610-618Crossref, Medline, Google Scholar
9. Parker G, Tupling H, Brown LB: A parental bonding instrument. Br J Med Psychol 1979; 52:1-10Crossref, Google Scholar
10. Parker G, Gladstone GL: Parental characteristics as influences on adjustment in adulthood, in Handbook of Social Support and the Family. Edited by Pierce GR, Sarason BR, Sarason IG. New York, Plenum, 1996, pp 195-218Google Scholar
11. Cloninger CR, Przybeck TR, Svrakic DM: The Tridimensional Personality Questionnaire: US normative data. Psychol Rep 1991; 69:1047-1057Google Scholar
12. Fairburn CG, Welch SL, Doll HA, Davies BA, O’Connor ME: Risk factors for bulimia nervosa. Arch Gen Psychiatry 1997; 54:509-517Crossref, Medline, Google Scholar
13. Tennant C: Life events and psychological morbidity: the evidence from prospective studies. Psychol Med 1983; 13:483-486Crossref, Medline, Google Scholar

