
Offspring of Depressed Parents: 20 Years Later
Abstract
Objective: This study was a 20-year follow-up of offspring of depressed and nondepressed parents to determine the magnitude and continuity of the risk of parental depression to the offspring. Method: The authors followed 151 offspring of moderately to severely depressed parents or nonpsychiatrically ill comparison subjects for about 20 years, to a mean age of 35 years. Four interviews and diagnostic assessments from childhood or adolescence to adulthood were conducted by assessors blind to the parents’ clinical status or the offspring’s previous history. Final best-estimate diagnoses were also made by blinded psychologists or psychiatrists. Results: The risks for anxiety disorders, major depression, and substance dependence were approximately three times as high in the offspring of depressed parents as in the offspring of nondepressed parents. Social impairment was also greater. The period of highest incidence for major depressive disorder remained between ages 15 and 20 years, largely in females. The early onset of disorder seen in the high-risk group was not offset by a later onset in the low-risk group as they matured. Higher rates of medical problems and mortality in the offspring of depressed parents were beginning to emerge as the offspring entered middle age. Conclusions: The offspring of depressed parents constitute a high-risk group for psychiatric and medical problems, which begin early and continue through adulthood. Early detection seems warranted.
We report results from a 20-year follow-up of offspring of depressed and nondepressed parents. Numerous studies have shown that the child and adolescent offspring of depressed, as compared to nondepressed, parents are at two- to threefold greater risk for major depressive disorder and anxiety disorders (1 – 9) . While there have been longitudinal studies of up to 40 years of adult depressed patients (10 – 12) , to our knowledge the longest follow-up of high-risk offspring is 4 years (7) . We know of no high-risk study that has followed the offspring into adulthood.
We previously reported findings from a 10-year follow-up of this cohort and showed that the highest risk for first-onset anxiety disorders was in childhood, for major depression it was in adolescence, and for substance dependence it was in adolescence and early adulthood. The peak age at onset of major depressive disorder in both high- and low-risk offspring ranged between 15 and 20 years (13) . At the 10-year follow-up the mean age of the offspring was 26 years. The mean age at this follow-up was 35 years. At the 10-year assessment some of the offspring had not yet passed through the critical period of risk for the onset of major depression and other disorders. With the availability of a longer follow-up, age-specific and cumulative lifetime rates of psychiatric disorders and their social and medical morbidity could be estimated more precisely. Medical morbidity was of particular interest as the cohort of offspring was aging and the medical burden of depression has been well documented (14 – 16) .
Method
In the original study, probands with moderate to severe major depressive disorder were selected from outpatient clinical specialty settings for the psychopharmacologic treatment of mood disorders. Nondepressed probands were also selected, at the same time, from an epidemiologic sample of adults from the same community. They were required to have no lifetime history of psychiatric illness, as indicated by several interviews. Full details of methods for wave 1 (baseline), wave 2 (year 2), and wave 3 (10-year follow-up) can be found elsewhere (8 , 13 , 17) . We have also presented data on the third generation (18 , 19) . In this article we report data from wave 4 (about 20 years after the first wave). The procedures were kept similar across the waves, with few exceptions, to avoid introducing methods bias. The proband, spouse, and offspring were interviewed by independent interviewers who were blind to the clinical status of the previous generations and the subject’s previous history. Two spouses of participants in the normal comparison group subsequently developed a major depression between waves 2 and 3, as determined by blind independent best-estimate diagnosis (described later). These families were reclassified as having depressed probands.
Study Group
At the initial interview (wave 1) the subjects consisted of 220 offspring between the ages of 6 and 23 years from 91 families (8) . Ten years after the initiation of the study, the families were reassessed. During the 10 years, among the 220 offspring interviewed at wave 1 there were two deaths and one offspring was found to have Down’s syndrome. Of the offspring interviewed at wave 1, 84% (182 of 217) were reinterviewed at the 10-year follow-up. There was no significant difference in attrition rate by parental diagnosis (13) . Over the next 10 years, there were two more deaths of offspring, leaving 215 offspring of the original cohort. Of the original available cohort of offspring, 70% (151 of 215) were reinterviewed about 20 years after the initial interview. There were no significant differences between interviewed and noninterviewed offspring by age, parental diagnosis, and depression status of the offspring at the last interview. Significantly more women (58%) than men (43%) were interviewed (χ 2 =5.20, df=1, p=0.02). All interview waves were approved by the institutional review board at New York State Psychiatric Institute/Columbia University. After complete description of the study to the subjects, written informed consent was obtained from adults and assent was obtained from the minors with written consent from their parents.
Assessments
The diagnostic interviews across all waves were conducted by using a semistructured diagnostic assessment, the Schedule for Affective Disorders and Schizophrenia—Lifetime Version (SADS-L) for adults (20) and the child version (K-SADS-E) modified for DSM-IV for subjects when they were between ages 6 and 17 (21 , 22) . The Global Assessment Scale (GAS) was completed by the best-estimate procedure at each wave (23) . This instrument is rated on a 0–100-point scale and provides an overall estimate of the person’s current functional adjustment based on all available information. A child’s version, the C-GAS, was used when the offspring were between ages 6 and 17 (24) . Lower scores on the GAS or C-GAS indicate more overall impairment. Life charts were used to record all episodes of illness and treatment that occurred during the period of assessment. Offspring completed the Social Adjustment Scale—Self Report, which contains questions on major areas of functioning on a 4-point scale, with higher scores indicating more impairment (25) . Data on medical illness were collected by using a standard medical checklist (available on request) that includes 57 conditions categorized according to the site or system affected, as well as the age at onset of each one and whether medication was taken for the condition. This information was collected at each wave from the subject and, in the case of minors, from the parent about the child. The data from all waves were pooled to create a lifetime history of medical conditions. Ambiguous reports of medical problems were coded during the best-estimate process by a physician blind to the depression status of the family.
Interviewers and Best-Estimate Procedures
The diagnostic assessments were administered by trained doctoral- and master’s-level mental health professionals, who were blind to the clinical status of the parents and to previous history information. Training remained the same across waves and has been described previously (13) . Multiple sources of information were obtained, including direct and informant interviews and medical records when available. Final diagnosis of all generations was based on the best-estimate procedure (26) . Two experienced clinicians, a child psychiatrist (D.P.) and psychologist (H.V.) who were not involved in the interviewing, independently and blind to the diagnostic status of the previous generation or prior assessments, reviewed all the material and assigned a DSM-IV diagnosis and a GAS score. The two diagnosticians co-rated 178 randomly selected cases from all generations. Kappa scores for interrater reliability were good to excellent: major depressive disorder, 0.82; dysthymia, 0.89; anxiety disorder, 0.65; alcohol abuse/dependence, 0.94; and drug abuse/dependence, 1.00.
Statistical Analysis
Preliminary analyses of group differences in the mean values for continuous outcomes by parental depression were tested by using the t test, and categorical outcomes were compared by the chi-square test. The potential confounding effects of age and sex were adjusted for in the analysis as follows. Continuous outcomes were analyzed by using linear regression with the offspring outcome, such as the C-GAS score, as the dependent variable and parental depression as the predictor variable (27) . Cross-sectional categorical outcomes (e.g., treatment variables) were analyzed by using logistic regression. Age and sex of offspring were considered a priori to be confounding variables and were retained in every model. These analyses were performed by applying the generalized estimating equations (GEE) approach (28) , by means of the GENMOD procedure in the SAS software package (29) , to estimate parameters and to adjust for potential nonindependence of outcomes for offspring from the same family. Survival analysis techniques adjusting for correlated survival times were used to estimate 1) the age-specific incidence rates of psychiatric disorder in 5-year intervals by using life-table methods and 2) cumulative lifetime rates of major depressive disorder in high-risk offspring by gender by means of a modified Kaplan-Meier method (30) . Cox proportional hazards regression models (31) , modified to adjust for clustered data (32) , were used to estimate the relative risks of disorder by parental depression status while controlling for potential confounding variables, by means of the SUDAAN software package (33) . The adjustment for clustered data was necessary to account for potential nonindependence of outcomes for offspring from the same family.
Results
Characteristics of Offspring
At the 20-year follow-up the offspring of the depressed and nondepressed probands did not differ by gender (58% female overall), age (mean age, 35 years), marital status (57% married, 29% never married, 13% separated/divorced), education (44% college graduates), employment status (78% working full time), mean annual individual income ($40,702), mean household income ($68,685), or mean number of children (1 , 6) .
Cumulative and Age-Specific Rates of Psychiatric Disorders
During the 20-year follow-up the offspring of depressed, as compared with nondepressed, parents had about a threefold higher risk of mood and anxiety disorders, mainly major depressive disorder and phobia ( Table 1 ). Among the offspring with major depression, the number of episodes, the duration of episodes, and the percentage of time in episodes did not differ between offspring of depressed and nondepressed parents. The mean age at onset of major depression was lower for the offspring of depressed parents than for the offspring of the nondepressed parents (16 versus 19 years), but this difference was not statistically significant (p=0.13) (table available on request). The higher risk of anxiety disorder in the offspring was not explained by comorbid anxiety in the parents (table available on request). While substance abuse was relatively common in both groups and not significantly different between the two groups, substance dependence was concentrated in the offspring of depressed parents. There was over a twofold greater risk of alcohol dependence and a sixfold higher risk of drug dependence (p=0.09 for each) and more than a twofold higher risk of either of these disorders. Bipolar disorder increased from 2% at the 10-year follow-up to 14% at the 20-year follow-up in the offspring of depressed parents, but the small numbers of subjects limit interpretation. None of the offspring of nondepressed parents developed bipolar I or II disorder over 20 years. The difference in social functioning between the offspring of depressed and nondepressed parents was independent of offspring psychopathology.
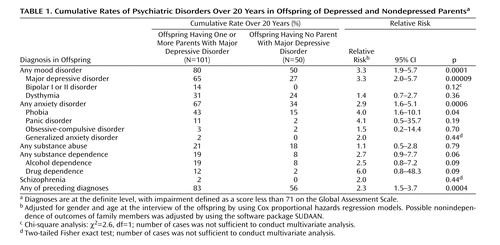
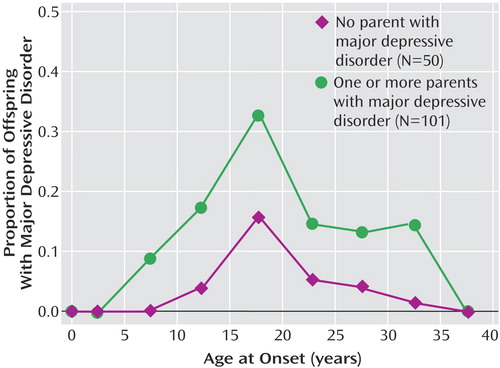
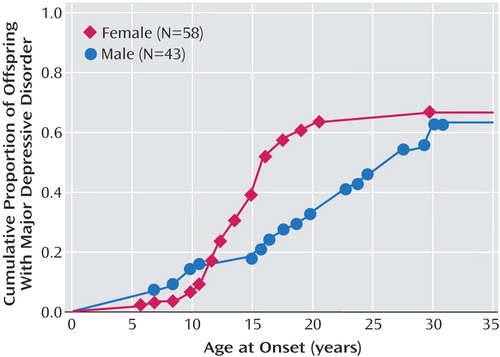
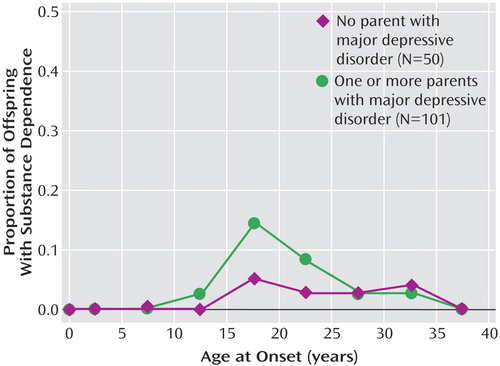
Figure 1 shows that even with a 20-year follow-up period the peak time for the incidence of major depressive disorder remained between ages 15 and 20 and that the rate of depressive onset remained higher in the offspring of depressed parents than in the low-risk offspring. Figure 2 shows the cumulative risk of major depressive disorder in male and female offspring of depressed parents only. Because of the small number of male offspring from the low-risk group, only rates from the high-risk offspring are presented. The peak rate of first onset between ages 15 and 20 was largely due to the females, whereas the males showed a gradual increase between ages 15 and 30. The gender difference in rates of major depressive disorder was significant. Figure 3 shows a different age pattern for anxiety disorders; “any anxiety disorder” includes panic disorder, generalized anxiety disorder, social and simple phobia, and obsessive-compulsive disorder, as well as the anxiety disorders specific to childhood (separation anxiety and overanxious disorder). The peak incidence of anxiety disorders, mainly phobias, was also before puberty but much earlier than that of major depressive disorder, especially in the offspring of depressed parents. The incidence rates declined after age 12, with a slight increase between ages 28 and 32 in the high-risk offspring. This increase around age 28 was largely due to panic disorder in women (data not shown). Figure 4 shows that the peak onset of substance dependence was also between ages 15 and 20; it largely involved males (data not shown).
a Significant difference between groups according to test of equality of strata (Wilcoxon test) (χ 2 =4.0, df=1, p=0.04).

Treatment and Impairment
As compared to the offspring of nondepressed parents, the offspring of depressed parents used significantly more outpatient mental health treatment over the 20 years and more continuous treatment over several years ( Table 2 ). More striking was the overall low rate of treatment.
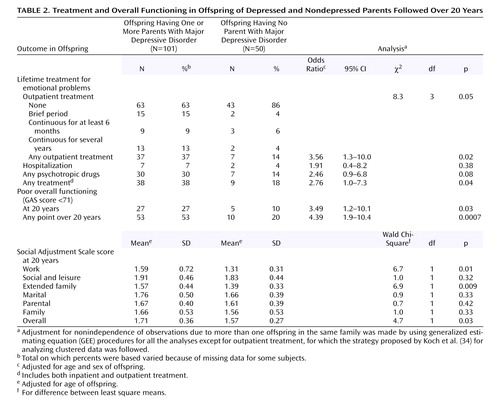
At the 20-year assessment, the offspring of depressed parents were also functioning more poorly overall, in work, and in the extended family. The impairment in the offspring of depressed parents, based on GAS scores, was evident at the 20-year follow-up; it was also shown by averages of the impairment scores across the four waves of interviews over 20 years.
Medical Illness and Mortality
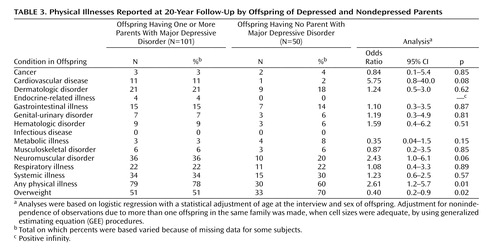
At an average age of 35 years, the offspring of depressed, as compared to nondepressed, parents were beginning to report more medical illnesses, particularly cardiovascular problems, which were more than five times as likely, and neuromuscular disorders, which were more than twice as likely. The likelihood of any physical health problem was also more than two times as high ( Table 3 ). The higher rates of cardiovascular and neuromuscular illnesses in the high-risk offspring were a reflection of positive responses to questions about a number of illnesses, none of which alone resulted in a significant difference between groups; for instance, 6% of the offspring of depressed parents and none of the comparison offspring reported hypertension. All of the subjects reporting cardiovascular illness had psychiatric disorders; 91% had mood disorders. The mean age at onset reported for cardiovascular problems was 31 years, and 28% of these subjects reported taking medication for the condition. The mean age at onset reported for hypertension was 34 years, and 50% reported taking medication for the condition. Data on age at onset of medication for neuromuscular illness were missing for so many subjects that the results could not be analyzed. The greater reports of medical problems in the high-risk subjects is not likely a function of overreporting in the high-risk group, since the rates reported for many problems (e.g., dermatologic conditions, headaches) did not differ between groups and more of the low-risk than high-risk offspring reported being overweight. The latter was also confirmed when we independently calculated body mass index from reported height and weight.
Consistent with the overall poorer medical health reported by the high-risk offspring was the mortality rate. Over the 20 years there were four deaths (two males and two females) in the high-risk offspring and none in the low-risk offspring. Based on a denominator of 220 (125 high- and 95 low-risk offspring who originally entered the study 20 years ago), a conservative estimate of the mortality rate in the high-risk group was 3% (same for males and females) and 0% in the low-risk group. This difference did not reach statistical significance according to Fisher’s exact test (p=0.14). The causes of death reported by family members for three of the deaths were suicide, lupus, and lymphoma. One cause was unknown because the offspring was estranged from the family.
Discussion
This 20-year follow-up into adulthood of the offspring of depressed and nondepressed parents confirmed previous observations about the early onset and greater risk of anxiety disorders and major depressive disorder in offspring of depressed parents and the high morbidity of major depression. The results were consistent with clinical observation of the medical morbidity of major depression as this cohort aged. The higher rates of anxiety disorders, major depression, and substance dependence in the offspring of depressed parents when they were adolescents were sustained over the follow-up, as they matured. The early onset of major depression, in adolescence, seen in the high-risk offspring was not offset by a later onset of major depression or other disorders in the low-risk offspring. Adolescence is a period of vulnerability to the onset of major depressive disorder, regardless of parental history. The peak in first onsets was before the age of 20, with anxiety disorders before puberty and with major depression and substance dependence after puberty. There was a small increase in panic disorder after age 25 in the high-risk offspring. This age at onset for panic disorder is consistent with findings from epidemiologic studies of community samples from diverse countries (35) . The findings also showed the sustained social morbidity and the emergence of medical morbidity in the offspring of depressed parents as the offspring entered middle age. Despite the poor course, over 60% of the high-risk offspring did not receive any psychiatric treatment.
This study has several strengths and limitations. We believe that it is the longest follow-up of high-risk offspring and comparison subjects ever reported; attrition over 20 years was relatively low and all clinical assessments were made by interviewers blind to the proband’s clinical status and to the subject’s previous psychiatric history. However, there are limitations. The number of subjects was relatively small, so that detailed comparison by gender or specific disorders could not be made. There was only one comparison group. The original probands, the depressed parents, were selected from a treatment clinic and had moderate to severe major depressive disorder. We cannot generalize to a community sample, members of which may have more mild depression or may not have received treatment. The comparison subjects came from a community sample, so generalizability may be more applicable to them. Finally, the design of four waves over 20 years is reasonable for determining patterns of onset but is inadequate for determining patterns of recurrence, which requires more closely spaced assessments.
Given the caveats about the study of treated subjects, findings from the 4-year prospective community study in Munich by Lieb et al. (7) are interesting. Direct diagnostic interviews based on the Munich version of the Composite International Diagnostic Interview were conducted on 2,548 offspring, ages 18–24, of depressed parents. A twofold higher risk of major depressive disorder, anxiety disorders, and substance abuse and greater impairment in offspring of depressed versus nondepressed parents were found. Comparable to our findings, the rate of bipolar disorder was slightly higher in the offspring of depressed than nondepressed parents (3% versus 1%). While there were higher rates of treatment in the offspring of depressed parents, the overall rates of treatment were low. Only about one-third of the offspring in the study by Lieb et al. and in ours received any psychiatric treatment.
The Munich study had the advantages of a large group of offspring and a less biased ascertainment of parents from the community. Our study had longer-term outcomes for the offspring, who are now in their mid to late 30s, and parents who were all clinically interviewed at multiple waves. The persistent impairment of depressed patients from childhood to adulthood regardless of parental history has been shown in numerous studies (11 , 12 , 36 , 37) . Taken together, these studies demonstrate once again that the offspring of depressed parents constitute an important high-risk group that includes many with early-onset depression. These findings are sturdy given that they are based in one study on parents from a treatment clinic and in the other on parents from a community survey.
The most intriguing finding in our study is the suggestion of more medical problems, particularly cardiovascular disease, in the high-risk offspring and the possibly higher mortality rate. Over the last few years studies have shown that 17%–27% of patients with coronary heart disease have major depression and an additional substantial number have subsyndromal symptoms (see references 16 and 38 for reviews). The most comprehensive review of studies of the relationship between coronary artery disease and depression, including 11 population-based prospective studies, indicated a 1.5 relative risk for the development of coronary artery disease conferred by major depressive disorder in patients initially free of clinical cardiac disease (16) , independent of other known risk factors for cardiac disease. Plausible biological mechanisms behind an etiologic role for major depression in coronary artery disease include altered immune, platelet, and hypothalamic-pituitary-adrenal axis functioning in depressed patients (39) . More speculative are the observations of increased hyperintensities in magnetic resonance imaging (MRI) studies of elderly depressed patients (40 , 41) . These findings in patients with late-onset depression (usually after age 50 years) have led to the tentative conclusion that late-onset depression may differ in biological mediation from earlier-onset depression. The offspring in our study are undergoing MRI studies. We may be able to see whether the same hyperintensities seen in late-onset major depressive disorder are present in the subjects with early-onset depression and whether this may be related to the suggestion of more coronary-related problems.
1. Kovacs M, Devlin B, Pollock M, Richards C, Mukerji P: A controlled family history study of childhood-onset depressive disorder. Arch Gen Psychiatry 1997; 54:613–623Google Scholar
2. Gershon ES, Hamovit JA, Guroff JJ, Dibble E, Leckman JF, Sceery W, Targum SD, Nurnberger JI Jr, Goldin LR, Bunney WE Jr: A family study of schizoaffective, bipolar I, bipolar II, unipolar, and normal control probands. Arch Gen Psychiatry 1982; 39:1157–1167Google Scholar
3. Hammen C, Burge D, Burney E, Adrian C: Longitudinal study of diagnoses in children of women with unipolar and bipolar affective disorder. Arch Gen Psychiatry 1990; 47:1112–1117Google Scholar
4. Downey G, Coyne JC: Children of depressed parents: an integrative review. Psychol Bull 1990; 108:50–76Google Scholar
5. Klein DN, Lewinsohn PM, Seeley JR, Rohde P: A family study of major depressive disorder in a community sample of adolescents. Arch Gen Psychiatry 2001; 58:13–20Google Scholar
6. Orvaschel H, Walsh-Allis G, Ye WJ: Psychopathology in children of parents with recurrent depression. J Abnorm Child Psychol 1988; 16:17–28Google Scholar
7. Lieb R, Isensee B, Hofler M, Pfister H, Wittchen HU: Parental major depression and the risk of depression and other mental disorders in offspring: a prospective-longitudinal community study. Arch Gen Psychiatry 2002; 59:365–374Google Scholar
8. Weissman MM, Gammon GD, John K, Merikangas KR, Warner V, Prusoff BA, Sholomskas D: Children of depressed parents: increased psychopathology and early onset of major depression. Arch Gen Psychiatry 1987; 44:847–853Google Scholar
9. Williamson DE, Birmaher B, Axelson DA, Ryan ND, Dahl RE: First episode of depression in children at low and high familial risk for depression. J Am Acad Child Adolesc Psychiatry 2004; 43:291–297Google Scholar
10. Angst J, Gamma A, Sellaro R, Lavori PW, Zhang H: Recurrence of bipolar disorders: a life-long perspective. Eur Arch Psychiatry Clin Neurosci 2003; 253:236–240Google Scholar
11. Judd LL, Akiskal HS, Zeller PJ, Paulus MP, Leon AC, Maser JD, Endicott J, Coryell W, Kunovac JL, Mueller TI, Rice JA, Keller MB: Psychological disability during the long-term course of unipolar major depressive disorder. Arch Gen Psychiatry 2000; 57:375–380Google Scholar
12. Mueller TI, Leon AC, Keller MB, Solomon DA, Endicott J, Coryell W, Warshaw M, Maser JD: Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry 1999; 156:1000–1006Google Scholar
13. Weissman MM, Warner V, Wickramaratne P, Moreau D, Olfson M: Offspring of depressed parents: 10 years later. Arch Gen Psychiatry 1997; 54:932–940Google Scholar
14. Evans DL, Charney DS: Mood disorders and medical illness: a major public health problem. Biol Psychiatry 2003; 54:177–180Google Scholar
15. Katon WJ: Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol Psychiatry 2003; 54:216–226Google Scholar
16. Rudisch B, Nemeroff CB: Epidemiology of comorbid coronary artery disease and depression. Biol Psychiatry 2003; 54:227–240Google Scholar
17. Weissman MM, Fendrich M, Warner V, Wickramaratne PJ: Incidence of psychiatric disorder in offspring at high and low risk for depression. J Am Acad Child Adolesc Psychiatry 1992; 31:640–648Google Scholar
18. Warner V, Weissman MM, Mufson L, Wickramaratne P: Grandparents, parents, and grandchildren at high risk for depression: a three-generation study. J Am Acad Child Adolesc Psychiatry 1999; 38:289–296Google Scholar
19. Weissman MM, Wickramaratne P, Nomura Y, Warner V, Verdeli H, Pilowsky D, Grillion C, Bruder G: Families at high and low risk for depression: a three generation study. Arch Gen Psychiatry 2005; 62:29–36Google Scholar
20. Mannuzza S, Fyer AJ, Klein DF, Endicott J: Schedule for Affective Disorders and Schizophrenia—Lifetime Version modified for the study of anxiety disorders (SADS-LA): rationale and conceptual development. J Psychiatr Res 1986; 20:317–325Google Scholar
21. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N: The Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 1997; 36:980–988Google Scholar
22. Orvaschel H, Puig-Antich J, Chambers W, Tabrizi MA, Johnson R: Retrospective assessment of prepubertal major depression with the Kiddie-SADS-E. J Am Acad Child Psychiatry 1982; 21:392–397Google Scholar
23. Endicott J, Spitzer RL, Fleiss JL, Cohen J: The Global Assessment Scale: a procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry 1976; 33:766–771Google Scholar
24. Shaffer D, Gould MS, Brasic J, Ambriosini P, Fisher P, Bird H, Aluwahlia S: Children’s Global Assessment Scale (C-GAS). Arch Gen Psychiatry 1983; 40:1228–1231Google Scholar
25. Weissman MM, Olfson M, Gameroff MJ, Feder A, Fuentes M: A comparison of three scales for assessing social functioning in primary care. Am J Psychiatry 2001; 158:460–466Google Scholar
26. Leckman JF, Sholomskas D, Thompson WD, Belanger A, Weissman MM: Best estimate of lifetime psychiatric diagnosis: a methodological study. Arch Gen Psychiatry 1982; 39:879–883Google Scholar
27. Kleinbaum DG, Kupper LL, Muller KE: Applied Regression Analysis and Other Multivariate Methods. Boston, PWS-Kent, 1988Google Scholar
28. Liang KY, Zeger SL: Longitudinal data analysis using generalized linear models. Biometrika 1986; 73:13–22Google Scholar
29. SAS/STAT* Software: Changes and Enhancements Through Release 6.11. Cary, NC, SAS Institute, 1996Google Scholar
30. Williams R: Product-limit survival functions with correlated survival times. Lifetime Data Anal 1995; 1:171–186Google Scholar
31. Cox DR: Regression models and life tables. Appl Stat 1972; 34:187–220Google Scholar
32. Binder DA: Fitting Cox’s proportional hazards models from survey data. Biometrika 1992; 79:139–147Google Scholar
33. Shah BV, Barnwell BG, Gayle GS: SUDAAN User’s Manual 7.5. Research Triangle Park, NC, Research Triangle Institute, 1997Google Scholar
34. Koch GG, Freeman DH Jr, Freeman JL: Strategies in the multivariate analysis of data from complex surveys. Int Stat Rev 1975; 43:59–78Google Scholar
35. Weissman MM, Bland RC, Canino GJ, Faravelli C, Greenwald S, Hwu HG, Joyce PR, Karam EG, Lee CK, Lellouch J, Lepine JP, Newman SC, Oakley-Browne MA, Rubio-Stipec M, Wells JE, Wickramaratne PJ, Wittchen HU, Yeh EK: The cross national epidemiology of panic disorder. Arch Gen Psychiatry 1997; 54:305–309Google Scholar
36. Geller B, Zimerman B, Williams M, Bolhofner K, Craney JL: Adult psychosocial outcome of prepubertal major depressive disorder. J Am Acad Child Adolesc Psychiatry 2001; 40:673–677Google Scholar
37. Reinherz HZ, Paradis AD, Giaconia RM, Stashwick CK, Fitzmaurice G: Childhood and adolescent predictors of major depression in the transition to adulthood. Am J Psychiatry 2003; 160:2141–2147Google Scholar
38. Meyer CM, Armenian HK, Eaton WW, Ford DE: Incident hypertension associated with depression in the Baltimore Epidemiologic Catchment Area Follow-Up Study. J Affective Disord 2004; 83:127–133Google Scholar
39. Joynt KE, Whellan DJ, O’Connor CM: Depression and cardiovascular disease: mechanisms of interaction. Biol Psychiatry 2003; 54:248–261Google Scholar
40. Hickie I, Scott E, Mitchell P, Wilhelm K, Austin MP, Bennett B: Subcortical hyperintensities on magnetic resonance imaging: clinical correlates and prognostic significance in patients with severe depression. Biol Psychiatry 1995; 37:151–160Google Scholar
41. Kramer-Ginsberg E, Greenwald BS, Krishnan KRR, Christiansen B, Hu J, Ashtari M, Patel M, Pollack S: Neuropsychological functioning and MRI signal hyperintensities in geriatric depression. Am J Psychiatry 1999; 156:438–444Google Scholar

