
Teaching Trainees to Negotiate Research Collaborations With Industry: A Mentorship Model
Abstract
Abstract
Research collaborations with the pharmaceutical industry can offer valuable opportunities for academic psychiatrists to gain access to important resources. Such relationships, however, often produce significant conflicts of interest, and recent attention has focused on the ways in which these conflicts can compromise research integrity. Psychiatric residents generally receive little education about industry-academia interactions. The authors report their experience collaborating on a research project with representatives of a pharmaceutical company, and they propose a model for teaching psychiatric trainees responsible and productive engagement with industry investigators.
Residents in a psychiatric training program were unsure about whether and how they would like to interact with the pharmaceutical industry. They had been cautioned by some faculty members about the potential for industry influence to bias their thinking and behavior, while other faculty had suggested that associations with industry are inevitable and, frequently, desirable. The majority of residents in the program began to interact with the pharmaceutical industry via attendance at industry-funded activities, acceptance of industry-sponsored gifts, awards, and medication samples, and reading of industry-financed journals and research studies. A smaller group of residents, finding it difficult to disentangle the tendentious elements of industry influence from useful ones, eschewed contact with the pharmaceutical industry whenever possible.
Those residents who were considering research careers found themselves facing a particular challenge. They valued the intellectual independence of academia but, in an era of increasing competition for limited research funds, regarded collaboration with the pharmaceutical industry as an opportunity to gain access to valuable resources: therapeutic compounds, data, expertise, and funding. They wished to make informed and deliberate choices about how to engage responsibly with industry but were sometimes uncertain about how to proceed.
Over the past decade, it has become increasingly apparent that interactions among physicians, academic medical centers, and the pharmaceutical industry are fraught with conflicts of interest that threaten the reputations of industry and academia as well as the ability of doctors to interpret data and treat patients without undue bias (1–3). For example, a growing body of evidence shows that gifts from drug companies—ranging from food and pens to substantial stipends and honoraria—influence the choices that physicians make in treating their patients (1, 4–6).
In 2006, a joint task force of the American Board of Internal Medicine Foundation and the Institute on Medicine as a Profession published policy recommendations on conflicts of interest (7), and the Association of American Medical Colleges followed suit in 2008 (8). Both recommended strict guidelines, including a zero-dollar limit on all gifts (including food), restriction of interactions between industry representatives and physicians, centralized distribution of industry funds for continuing medical education, and discouragement of ghostwriting and speakers bureaus (1). Although there are no clear mechanisms for enforcing these recommendations, the institutions that have implemented them have generally found the transition to be smooth and rapid, with "top-down" modeling of proper conduct particularly effective (1). The current generation of residents and medical students may thus develop in a milieu where restraint and reflection in interactions with drug companies are the norm rather than the exception.
In the area of medical research, however, appropriate boundaries on interactions between academia and industry are less clear-cut, perhaps in part because this is a realm in which collaborations are more evidently mutually advantageous. Drug companies rely on medical centers to conduct trials and recruit patients, as well as for thought leaders to design studies and for academic scientists to identify new drug targets and test promising compounds. Complementarily, in an era of limited government funding, industry money is a much-needed boon to research activities in academic departments. In this context, industry-academia research collaborations have themselves become increasingly vulnerable to conflicts of interest. Whereas 20 years ago most academic investigators assumed complete responsibility for industry-sponsored studies, more recently the converse is true, with drug companies frequently exerting control over all aspects of the process, from designing experiments to analyzing data to writing papers to dictating final decisions on which data to publish and where (2, 9). Studies are frequently designed and reported in ways that suit the interests of sponsoring companies, including over- or underdosing comparator compounds, choosing placebo-controlled trials over comparison with active competitor drugs, designating primary endpoints that are likely to favor the sponsor's product rather than the most clinically relevant outcomes, publishing partial data sets, and neglecting to publish negative results (2). An illustrative example involves recent revelations about studies by Merck on the cyclo-oxygenase-2 inhibitor rofecoxib that were ghostwritten by company employees despite attribution to academic investigators (10) or manipulated to underreport mortality caused by the drug (11). Similarly, a review of 74 clinical trials of antidepressant medications found that all but one of 38 positive studies were published, but only three of 36 negative studies were accurately represented (12).
It has been argued that major policy overhaul and increased oversight are needed in funding and publication processes for industry-sponsored research (13). Equally important may be a culture and policy shift within academic departments to prioritize ethical and transparent interactions with industry, much as is currently happening with drug company contributions to individual clinicians and educational programs (1, 3). A crucial point of intervention may be in the education of residents, who are in the process of learning to navigate relationships with industry.
Professor Jeffrey Lieberman, chair of the department in which the above-mentioned residents were training, informed the residents that he had been approached by representatives of a pharmaceutical company who wished to collaborate on a research project. The company was interested in conducting a post hoc analysis of two large prospective trials to determine how its medication (aripiprazole) compared with a reference compound (haloperidol) in a subpopulation of patients with early-stage schizophrenia (14). Dr. Lieberman, with the company's agreement, invited residents to become involved and offered to mentor them through the collaboration process.
Several residents volunteered to attend meetings in which Dr. Lieberman modeled collegiality and professional independence in his dealings with the pharmaceutical representatives. There was limited interaction between the residents and the representatives when the chairman was not present (e.g., in the waiting room outside the conference room where the group met). After each meeting, Dr. Lieberman conferred with the residents and instructed them on responsible engagement with industry researchers. He emphasized the importance of careful review of the original trials (14) and subsequent analyses of these trials (15–17) to determine what meaningful information might be obtained from a post hoc analysis; thoughtful selection of research hypotheses; and critical appraisal of results. Together, Dr. Lieberman and the residents framed several hypotheses of scientific and clinical interest and identified methods to test them using the company's data. They then submitted their hypotheses and proposed analysis plan to the industry representatives for statistical analysis.
The nature of interactions between psychiatric trainees and the pharmaceutical industry is complex. Residents experience significant exposure to industry in a variety of contexts (18–21), and many do not appreciate the potential consequences of resident-industry contacts (18, 22). For example, in many, but not all (23), studies, only a minority of residents reported believing that interactions with industry influence their prescribing practices (18, 21, 24–26), despite substantial evidence that information provided by drug companies to caregivers affects prescribing patterns (18). In fact, psychiatric residents may feel more immune to industry influence than do residents in other medical specialties (25).
Curiously, psychiatric training programs have placed little emphasis on educating residents about their contacts with industry. Until recently, most programs allowed unsupervised interactions between residents and industry representatives, and few had formal policies regulating these interactions (20, 21, 27, 28). While the majority of programs provide some instruction on resident-industry relationships, teaching in this area is generally informal (28) and tends to focus on the acceptance of gifts that may affect prescribing practices, to the neglect of other important relationships with industry (18), such as research collaborations. The lack of guidance and training on research collaborations with industry is regrettable, given the importance of exposing residents to research early in their training (29) and the considerable role that pharmaceutical companies play in research, particularly in the field of pharmacotherapy (30).
One explanation for the dearth of policy and education on interactions between residents and industry may be the lack of clarity regarding the efficacy of such interventions. A variety of educational and policy strategies targeting residents have been investigated, including in a psychiatric training program (25), with mixed results (22, 31–35). In one study, policies restricting contact between residents and drug companies were found to decrease the perceived benefit of these interactions (34). Some educational interventions have been shown to improve residents' understanding of the complexity of relationships with the pharmaceutical industry (22) or to lead residents to report greater caution when considering their future interactions with industry (31). One intervention, in contrast, succeeded only in educating residents about the negative effects that interactions with industry may have on other physicians and did not persuade residents to reassess their own vulnerability to influence (32). Another strategy showed little impact on residents' opinions of industry (35). An educational intervention specifically targeting psychiatric residents resulted in decreased acceptance of gifts and supplies but did not appreciably alter attitudes about resident-industry interactions (25). In light of these conflicting data, further development and assessment of strategies for teaching residents how to understand and negotiate interactions with the pharmaceutical industry are merited (18, 20, 21, 24, 26, 27). Fortunately, there is substantial enthusiasm in the field of psychiatry, and among residents in particular, for more education in this area (25, 28).
Dr. Lieberman and the residents met with the industry representatives to review the results of the statistical analyses. The representatives' report included some of the analyses proposed by the departmental group and an outline for a manuscript that concluded that aripiprazole outperformed haloperidol in patients with early-stage schizophrenia. After careful inspection of the report, Dr. Lieberman and the residents found that the results did not, in fact, unequivocally support the conclusions of the draft manuscript. They noted that the mean dose of haloperidol used in the study was 8.6 mg/day, higher than that used in the most recent first-episode schizophrenia trials (36–38). Aware that early-stage schizophrenia patients are more sensitive to drug side effects and require lower doses of medications for therapeutic response (by 50% or more) than chronic patients (39–41) and that haloperidol in first-episode psychosis causes more extrapyramidal symptoms than do second-generation antipsychotics (36–38, 40, 1–44), the departmental group was prompted to consider whether the apparent superiority of aripiprazole may have been due predominantly to excessive dosing, and hence intolerable side effects, of haloperidol.
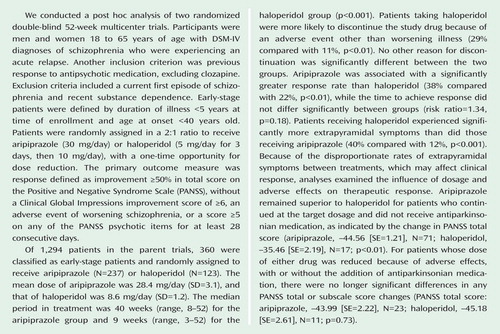
Dr. Lieberman and the residents worked with the industry representatives to obtain the complete results of the statistical analyses previously designated by the group (see Figure 1). These analyses revealed high rates of extrapyramidal symptoms and increased and more rapid dropout from the study among patients treated with haloperidol. Discontinuation due to an adverse event other than worsening illness was the only significant difference in reason for treatment discontinuation between treatments. In addition, the efficacy differences on the Positive and Negative Syndrome Scale (PANSS) favoring aripiprazole were seen in measures that could be confounded with extrapyramidal symptoms (45). Finally, when patients whose extrapyramidal symptoms were managed by dose reduction or the addition of antiparkinsonian medication were examined separately, all PANSS efficacy differences disappeared.
Under the supervision of Dr. Lieberman, the trainees drafted a manuscript that reflected their interpretation of these results, including their impression that the difference in drug efficacy may have been due to the differential dropout rate and greater side effects caused by the high dosage of haloperidol used in the study. These conclusions differed from publications of previous analyses of the parent trials, which found aripiprazole to be superior to haloperidol in durability of symptom response (14), adverse effects (14), remission rate (15), new-onset tardive dyskinesia rate (16), and utility (a function of PANSS scores and adverse effects) (14–17).
While developing the manuscript, the residents continued to meet, with Dr. Lieberman and separately, to discuss the challenges of the project. These challenges included the selection of appropriate statistical methods for a post hoc analysis with multiple hypotheses; the difficulty and importance of prioritizing the group's interpretations, even when they differed from those of the pharmaceutical company; and the lack of transparency regarding the original data, to which the company retained exclusive access.
By the end of the project, the departmental group believed that they had identified findings of interest to clinical and research communities and that their presentation of these findings was objective and accurate. They had also learned about post hoc hypothesis formation, several statistical techniques, and the importance of access to original study data.
Academic psychiatrists may benefit from research collaborations with industry (46), and the enterprise of industry-sponsored research may itself be improved by the involvement of experienced academic investigators, as compared to exclusive reliance on researchers employed by the pharmaceutical industry. Few psychiatric training programs, however, provide instruction on how to negotiate these collaborations responsibly. We propose that the mentoring of trainees by a senior academic psychiatrist through a research project with industry representatives may be a useful means of teaching appropriate modes of working cooperatively with the pharmaceutical industry. Role modeling by senior psychiatrists has been reported to have a significant effect on the shaping of resident perceptions about industry in general (21, 35), and our experience suggests that the same may be true of research collaborations in particular.
In the proposed arrangement, the academician-trainee-industry relationship is analogous to the supervisor-resident-patient triad that forms the backbone of psychiatric education in many training programs. Such an approach benefits from the reciprocal advantages of allowing trainees to learn fruitful and principled modes of engaging industry researchers and motivating senior psychiatrists to model critical thinking, independence, and integrity in their dealings with the pharmaceutical industry. Notably, this approach also suffers from the same limitations as other supervisory relationships, especially those imposed by the mentor's own biases.
Despite recent consternation over academia-industry research collaborations, we believe that these cooperative efforts will remain appropriate and valuable opportunities for academic psychiatrists, if conducted responsibly. Given the limited government resources currently available for research and teaching and the increasing costs of large long-term clinical trials, psychiatric training programs may wish to embrace the expanding role of research collaborations with pharmaceutical companies and teach ethical and productive engagement with industry investigators. We suggest that the mentoring of trainees by a senior academic psychiatrist may be one effective way of doing this.
1 : New developments in managing physician-industry relationships. JAMA 2008; 300:1067–1069 Crossref, Medline, Google Scholar
2 : Industry-sponsored clinical research: a broken system. JAMA 2008; 300:1069–1071 Crossref, Medline, Google Scholar
3 : Industry support of medical education. JAMA 2008; 300:1071–1073 Crossref, Medline, Google Scholar
4 : Doctors and drug companies. N Engl J Med 2004; 351:1885–1890 Crossref, Medline, Google Scholar
5 : A social science perspective on gifts to physicians from industry. JAMA 2003; 290:252–255 Crossref, Medline, Google Scholar
6 : Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA 2000; 283:373–380 Crossref, Medline, Google Scholar
7 : Health industry practices that create conflicts of interest: a policy proposal for academic medical centers. JAMA 2006; 295:429–433 Crossref, Medline, Google Scholar
8 Association of American Medical Colleges: Industry Funding of Medical Education: Report of an AAMC Task Force. Washington, DC, June 2008. https://services.aamc.org/Publications/showfile.cfm?file=version114.pdf&prd_id=232&prv_id=281&pdf_id=114 Google Scholar
9 : Gag clauses in clinical-trial agreements. N Engl J Med 2005; 352:2160–2162 Crossref, Medline, Google Scholar
10 : Guest authorship and ghostwriting in publications related to rofecoxib: a case study of industry documents from rofecoxib litigation. JAMA 2008; 299:1800–1812 Crossref, Medline, Google Scholar
11 : Reporting mortality findings in trials of rofecoxib for Alzheimer disease or cognitive impairment: a case study based on documents from rofecoxib litigation. JAMA 2008; 299:1813–1817 Crossref, Medline, Google Scholar
12 : Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med 2008; 358:252–260 Crossref, Medline, Google Scholar
13 : Impugning the integrity of medical science: the adverse effects of industry influence. JAMA 2008; 299:1833–1835 Crossref, Medline, Google Scholar
14 : Efficacy and safety of aripiprazole vs haloperidol for long-term maintenance treatment following acute relapse of schizophrenia. Int J Neuropsychopharmacol 2003; 6:325–327 Crossref, Medline, Google Scholar
15 : Symptomatic remission in schizophrenia patients treated with aripiprazole or haloperidol for up to 52 weeks. Schizophr Res 2007; 95:143–150 Crossref, Medline, Google Scholar
16 : Comparative assessment of the incidence and severity of tardive dyskinesia in patients receiving aripiprazole or haloperidol for the treatment of schizophrenia: a post hoc analysis. J Clin Psychiatry 2007; 68:1901–1906 Crossref, Medline, Google Scholar
17 : Comparative utility of aripiprazole and haloperidol in schizophrenia: post hoc analysis of two 52-week, randomized, controlled trials. Appl Health Econ Health Policy 2009; 7:109–119 Crossref, Medline, Google Scholar
18 : The role of the pharmaceutical industry in teaching psychopharmacology: a growing problem. Acad Psychiatry 2005; 29:222–229 Crossref, Medline, Google Scholar
19 : Pharmaceutical representatives and emergency medicine residents: a national survey. Ann Emerg Med 1993; 22:1593–1596 Crossref, Medline, Google Scholar
20 : Interactions with the pharmaceutical industry: a survey of family medicine residents in Ontario. CMAJ 1996; 155:1243–1248 Medline, Google Scholar
21 : Interactions between pharmaceutical representatives and doctors in training: a thematic review. J Gen Intern Med 2005; 20:777–786 Crossref, Medline, Google Scholar
22 : What residents don't know about physician-pharmaceutical industry interactions. Acad Med 2004; 79:432–437 Crossref, Medline, Google Scholar
23 : Pharmaceutical branding of resident physicians. JAMA 2001; 286:1024–1025 Crossref, Medline, Google Scholar
24 : Interactions with the pharmaceutical industry: experiences and attitudes of psychiatry residents, interns, and clerks. CMAJ 1995; 153:553–559 Medline, Google Scholar
25 : Attitudes and behaviors of psychiatry residents toward pharmaceutical representatives before and after an educational intervention. Acad Psychiatry 2005; 29:33–39 Crossref, Medline, Google Scholar
26 : Of principles and pens: attitudes and practices of medicine housestaff toward pharmaceutical industry promotions. Am J Med 2001; 110:551–557 Crossref, Medline, Google Scholar
27 : Pharmaceutical policies in Canadian family medicine training: survey of residency programs. Can Fam Physician 1997; 43:1947–1951 Medline, Google Scholar
28 : A survey of the interactions between psychiatry residency programs and the pharmaceutical industry. Acad Psychiatry 2005; 29:40–46 Crossref, Medline, Google Scholar
29 : A developmental model for enhancing research training during psychiatry residency. Acad Psychiatry 2006; 30:55–62 Crossref, Medline, Google Scholar
30 : Industry sponsorship and financial conflict of interest in the reporting of clinical trials in psychiatry. Am J Psychiatry 2005; 162:1957–1960 Link, Google Scholar
31 : A prospective before-and-after trial of an educational intervention about pharmaceutical marketing. Acad Med 2004; 79:1046–1050 Crossref, Medline, Google Scholar
32 : Effects of an educational intervention on residents' knowledge and attitudes toward interactions with pharmaceutical representatives. J Gen Intern Med 1997; 12:639–642 Crossref, Medline, Google Scholar
33 : Structured approach to pharmaceutical representatives: family medicine residency program. Can Fam Physician 1998; 44:1053–1056, 1059–1060 Medline, Google Scholar
34 : Effect of restricting contact between pharmaceutical company representatives and internal medicine residents on post training attitudes and behavior. JAMA 2001; 286:1994–1999 Crossref, Medline, Google Scholar
35 : Residents' perceptions over time of pharmaceutical industry interactions and gifts and the effect of an educational intervention. Acad Med 2006; 81:595–602 Crossref, Medline, Google Scholar
36 : Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomized clinical trial. Lancet 2008; 371:1085–1097 Crossref, Medline, Google Scholar
37 : Risperidone and haloperidol in first-episode psychosis: a long-term randomized trial. Am J Psychiatry 2005; 162:947–953 Link, Google Scholar
38 : Maintenance treatment with risperidone or low-dose haloperidol in first-episode schizophrenia: 1-year results of a randomized controlled trial within the German Research Network on Schizophrenia. J Clin Psychiatry 2007; 68:1763–1774 Crossref, Medline, Google Scholar
39 : Prevalence and clinical correlates of extrapyramidal signs and spontaneous dyskinesia in never-medicated schizophrenic patients. Am J Psychiatry 1995; 152:1724–1729 Link, Google Scholar
40 : Comparative efficacy and safety of atypical and conventional antipsychotic drugs in first-episode psychosis: a randomized, double-blind trial of olanzapine versus haloperidol. Am J Psychiatry 2003; 160:1396–1404 Link, Google Scholar
41 : Optimal dose of neuroleptic in acute schizophrenia: a controlled study of the neuroleptic threshold and higher haloperidol dose. Arch Gen Psychiatry 1991; 48:739–745 Crossref, Medline, Google Scholar
42 : A practical clinical trial comparing haloperidol, risperidone, and olanzapine for the acute treatment of first-episode nonaffective psychosis. J Clin Psychiatry 2006; 67:1511–1521 Crossref, Medline, Google Scholar
43 : Risperidone in the treatment of first-episode psychotic patients: a double-blind multicenter study. Schizophrenia Bull 1999; 25:721–729 Crossref, Medline, Google Scholar
44 : Olanzapine and haloperidol in first episode psychosis: two-year data. Schizophr Res 2006; 86:234–243 Crossref, Medline, Google Scholar
45 : Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry 2005; 10:79–104 Crossref, Medline, Google Scholar
46 : Institutional leadership and faculty response: fostering professionalism at the University of Pennsylvania School of Medicine. Acad Med 2007; 82:1049–1056 Crossref, Medline, Google Scholar

