
Association of Different Adverse Life Events With Distinct Patterns of Depressive Symptoms
Abstract
Objective: The authors sought to determine whether, in a general population sample, different categories of adverse life events were associated with different patterns of depressive symptoms. Method: A total of 4,856 individuals (53% female) who experienced depressive symptoms in the previous year were assessed in up to four waves over a maximum of 12 years. At each wave, participants reported the severity of 12 symptoms disaggregated from the nine DSM-III-R criteria for major depression and the self-identified cause of these symptoms, which were classified into nine categories of adverse life events. Results: The patterns of depressive symptoms associated with the nine categories of adverse life events differed significantly. Deaths of loved ones and romantic breakups were marked by high levels of sadness, anhedonia, appetite loss, and (for romantic breakups) guilt. Chronic stress and, to a lesser degree, failures were associated with fatigue and hypersomnia, but less so with sadness, anhedonia, and appetite loss. Those who reported that no adverse life events caused their dysphoric episodes reported fatigue, appetite gain, and thoughts of self-harm, but less sadness or trouble concentrating. These symptom patterns were found in a between-persons analysis of participants who had a single dysphoric episode, and they were replicated in an independent within-persons analysis of episode-specific symptom deviations among individuals with multiple episodes. Similar results were obtained when the sample was restricted to those meeting DSM-III-R diagnostic criteria for major depression. Conclusions: Depression is a pathoplastic syndrome. Different types of life events are related to different depressive symptom profiles. The results from the within-persons analysis suggest that these relationships are causal.
A central question in psychiatry has been whether variation in causal factors is related to variation in clinical presentation. While aspects of a syndrome may be central or core (pathogenic), other aspects may be pathoplastic, differing as a function of personal or precipitating factors (1) . Much of the debate over the nosology of major depression—the “unitary” (2) versus “pluralistic” (3) viewpoints—can be seen as attempts to understand the pathogenic and pathoplastic nature of depression. What aspects of depression are invariant across individuals and across episodes within individuals, and what, if any, aspects depend on factors specific to the individual or episode? Attempts to understand this latter issue generally focus on differences in symptom profiles, precipitating causes, or both (4) .
The two most common subdivisions of major depression, melancholic (or endogenous) depression and atypical depression, are based on depressive symptom profiles that are thought to reflect stable interpersonal differences in how depression is manifested in different people. Similarly, diathesis-stress models suggest that distinct symptom profiles arise from interactions between specific cognitive styles and adverse life events (ALEs) to which people with the predisposing cognitive style are particularly vulnerable (5 , 6) . Both approaches predict that differences in depressive symptoms between episodes are due to stable interpersonal differences and that the symptom profiles of multiple episodes in an individual should be similar. However, several recent studies have found only modest stability in symptom profiles across episodes in the same individual (7 – 9) , which raises the possibility that some of the differences in depressive symptoms across episodes are caused by situational factors.
Research on college students (10 , 11) has shown relationships between broad ALE categories and distinct depressive symptom patterns. Social losses, such as deaths of loved ones and romantic breakups, were associated with more emotional pain, crying, desire for social support, and appetite loss. Wintertime blues were associated with symptoms typical of seasonal affective disorder. Failures and chronic stress were associated with more guilt, hopelessness, and fatigue.
These associations between ALE categories and depressive symptom profiles could result from several processes. The two most plausible are that ALE categories cause the variable symptom profiles or that some stable personal characteristic, such as personality, causes individuals to exhibit certain patterns of depressive symptoms and place themselves at higher risk of certain types of ALEs. Studying multiple depressive episodes within individuals can definitively discriminate between these two hypotheses. The effects of stable personal characteristics on symptom patterns are removed by analyzing episode-specific symptom deviations—the symptom levels in an episode after controlling for the person’s mean level across episodes. In this study, we determined whether particular ALE categories were associated with distinct depressive symptom profiles in a general population sample of adults. We also examined whether these results occurred among persons with syndromal major depression, and we analyzed episode-specific symptom deviations among individuals who experienced multiple dysphoric episodes in order to test whether these results were due to stable interpersonal versus situational factors.
Method
Sample
Participants came from the Virginia Adult Twin Study of Psychiatric and Substance Use Disorders, a longitudinal study of Caucasian twins drawn from the population-based Mid-Atlantic Twin Registry (12) . Longitudinal data came from female-female twin pairs who participated in up to four personal interviews and from male-male and male-female twin pairs who participated in up to two personal interviews. This study is based on individuals who experienced one or more dysphoric episodes (see Measures below) during any wave; this included 2,595 women with a mean age at assessment of 33.9 years (SD=8.5) and 2,261 men with a mean age at assessment of 35.5 years (SD=8.8). Additional details of sample ascertainment and characteristics are available elsewhere (12 , 13) .
Measures
During each interview, we assessed the occurrence over the previous year of 12 depressive symptoms lasting at least 5 days and representing the disaggregated nine symptoms of criterion A for major depression in DSM-III-R (insomnia, hypersomnia, appetite/weight gain, appetite/weight loss, psychomotor retardation, and restlessness were assessed as six separate symptoms). Participants used a 5-point scale to indicate the degree to which each symptom interfered with their daily life, which served as a measure of symptom severity (from 0, absence of the symptom, to 4, symptom interfering completely with daily life). Interviewers probed to ensure that each symptom was not due to medication or physical illness. Participants were then asked which symptoms co-occurred, and the interviewer aggregated these symptoms into co-occurring syndromes. We define dysphoric episode as any syndrome in which two or more of the nine symptoms of DSM-III-R criterion A co-occurred. This level of depressive symptoms has been shown to be associated with substantial psychosocial and role impairment (14 , 15) . We did not require the presence of a large number of symptoms (e.g., five of nine) because we wanted to analyze subthreshold depressive episodes first, and we did not require the presence of any specific symptoms (e.g., sadness or anhedonia) because such an approach would bias the very phenomena—symptom profiles—under investigation. However, in a follow-up analysis, we restricted our sample to those who met full criteria for major depression (see Statistical Analysis below). If more than one dysphoric episode occurred within the previous year, we analyzed the one the participant identified as being the worst. Test-retest reliability was assessed in 119 individuals who experienced a dysphoric episode and who were interviewed twice by different interviewers (average interview interval of 30 days [SD=9]) and was found to be adequate: the average weighted kappa coefficient across the 12 symptoms was 0.47, and the average polychoric correlation coefficient was 0.72.
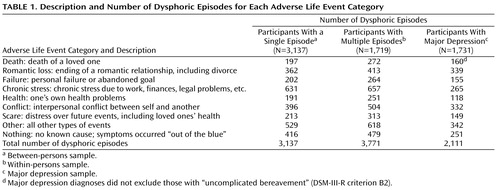
For each dysphoric episode, participants were asked, “During this period, did something happen to make you feel that way or did the feeling just come on you ‘out of the blue’?” If participants could think of a cause, they were asked to describe it. Interviewers assigned these responses to one of several hundred specific causal codes. When participants indicated multiple causes (21% of the time), they ordered them by causal importance. For this study, we collapsed the primary (first) causal codes into nine ALE categories ( Table 1 ). Thus, each dysphoric episode was associated with a single ALE category for a given wave, although different ALE categories could and often did occur across waves for the same person. A list of the correspondence between the nine broad ALE categories and the specific causal codes is available at the first author’s web site (http://matthewckeller.com/html/publications.html). In the 119 individuals who experienced a dysphoric episode and who were interviewed twice by different interviewers, the test-retest reliability of the ALE categories was adequate, with a kappa coefficient of 0.51.
To control for mood in the previous 30 days, respondents completed the depression and anxiety subscales of the Revised Symptom Checklist-90 (16) . This information was missing for 731 dysphoric episodes (11%) because it was not collected for one of the waves; its mean value was substituted when it was missing, although a follow-up analysis also dropped these subjects (see below). We used an adapted version of the Structured Clinical Interview for DSM-III-R (17) to make diagnoses of major depression in the previous year.
Statistical Analysis
We conducted three analyses. The first was restricted to the 3,137 individuals (the between-persons sample) who experienced only one dysphoric episode or who experienced multiple dysphoric episodes all caused by the same ALE category. Among participants who experienced multiple episodes caused by the same ALE category, we randomly selected one for analysis. The dependent variables for this analysis were the 12 standardized symptom scales.
The second analysis was restricted to the 1,719 individuals (the within-persons sample) who experienced two or more dysphoric episodes across waves that were caused by two or more different ALE categories. There were 3,771 dysphoric episodes in the within-persons sample. To control for stable interpersonal differences in mean symptom levels, the dependent variables for the primary analysis of this sample were 12 within-persons symptom deviations: a participant’s symptom levels from a given episode subtracted from the symptom means across all episodes for that participant. For comparability with the between-persons sample results, we also performed a supplementary analysis on the (nondeviation) standardized symptom scales from this sample. The within-persons and between-persons samples were mutually exclusive, so tests on them are essentially independent.
The third analysis was restricted to the 1,731 individuals (the major depression sample) from both the within-persons and the between-person samples whose dysphoric episodes met full DSM-III-R criteria for major depression. This sample was therefore not independent of the first two samples. We randomly selected one episode for analysis among participants who experienced multiple depressive episodes caused by the same ALE category, although we allowed multiple episodes from the same person if they were caused by different ALE categories. The dependent variables were the 12 standardized symptom scales.
For each analysis, we conducted an omnibus test and several follow-up contrasts (described in Results). The omnibus prediction that different ALE categories are associated with different depressive symptom patterns was tested by the ALE-by-symptom interaction term in a repeated-measures multivariate analysis of variance (MANOVA). The 12 standardized depressive symptoms (in the analyses of the between-persons sample and the major depression sample) or the 12 standardized depressive symptom deviations (in the within-persons analyses) served as repeated-measures dependent variables, and the nine categorical ALE categories served as between-subjects predictor variables.
For valid statistical inference, MANOVA requires multivariate normality of the residuals, equality of the variance-covariance matrices of the dependent variables across the levels of the predictors, and independence of the residual terms. In our data, none of these assumptions was met. For example, multiple data entries from the same family (across twins) were present in all three analyses. To generate valid inferential statistics despite these violations of assumptions, we derived all p values of inferential statistics empirically, via permutation testing, based on 10,000 runs. These empirical p values are denoted p e . We permuted the data accounting for its nested dependencies (e.g., multiple episodes nested within individuals nested within twin pairs).
Given that so few of the symptom data were missing (<0.1% in all data sets), we imputed missing symptom data using an expectation maximization algorithm developed by Schafer (18) . We used an approximation to the F statistic (a transformation of Wilks’s lambda developed by Rao [19] ) as the inferential statistic from MANOVA analyses. All tests controlled for age, gender, duration of the dysphoric episode, and depression and anxiety in the previous 30 days. The results did not substantively change when tests did not control for these variables or when episodes with any data missing on the independent, dependent, or control variables were removed. The results were also similar when we conducted separate tests on men versus women, and on participants who were younger versus older than the median age. The statistical software used for all analyses was “R,” version 2.1.1 (20) .
Results
Between-Persons Analyses
Among the 3,137 individuals who experienced one dysphoric episode or who experienced multiple episodes associated with the same ALE category, the ALE-by-symptom MANOVA interaction term was highly significant across the 12 depressive symptoms (F=6.20, df=88, 20403, p e <0.001), indicating that different ALE categories were associated with different patterns of depressive symptoms. Figure 1 compares the symptom profiles of the nine ALE categories in the between-persons sample. The F values (in the figure notes) indicate that the mean symptom levels varied significantly across symptoms (the symptom profiles were nonflat) for seven of the nine ALE categories. Social losses due to deaths or romantic breakups were associated with grief-like responses; the mean levels of feeling blue, anhedonia, appetite loss, and insomnia were one-quarter to one-half of a standard deviation (Cohen’s d ranging from 0.25 to 0.5) above the mean levels of fatigue, psychomotor retardation, and appetite gain within both of these ALE categories. Chronic stress and reactions that had no precipitating cause (the “nothing” ALE category) were associated with enervation and appetite gain but few emotional symptoms; the mean levels of fatigue, psychomotor retardation, and appetite gain were one-quarter to one-half of a standard deviation above the mean levels of feeling blue, anhedonia, and appetite loss.
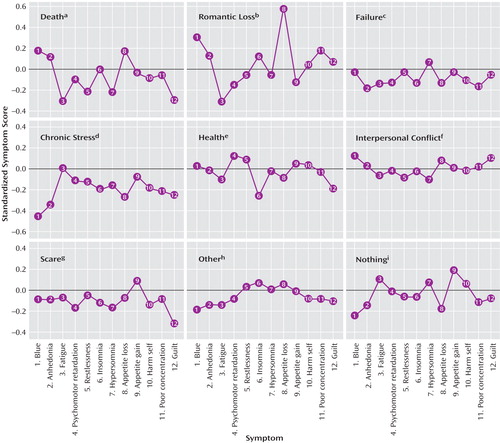
a F=10.03, p<0.001.
b F=15.96, p<0.001.
c F=1.58, p<0.29.
d F=10.14, p<0.001.
e F=3.81, p<0.002.
f F=2.59, p<0.07.
g F=4.02, p<0.001.
h F=3.58, p<0.01.
i F=5.75, p<0.001.
An alternative way of exploring these results is to examine the mean profiles symptom by symptom. To do this, we must control for main effects of ALE categories (i.e., average symptom levels differing between ALE categories) (21) . A series of one-way analyses of variance revealed that every symptom except self-harm and trouble concentrating differed significantly between ALE categories. The mean levels of feeling blue, fatigue, and appetite loss were especially variable ( Figure 2 ; for profiles of average depressive symptoms for this sample, see Figure S3 in the data supplement that accompanies the online version of this article). Anhedonia was elevated after deaths and romantic losses and was lowest after stress and failures. Fatigue was elevated for stress and episodes with no precipitating cause but not for deaths or romantic losses. Guilt was commonly reported after conflicts but rarely after deaths, scares, and health concerns. Appetite gain was frequently reported after scares and episodes with no precipitating cause and was reported especially infrequently after romantic loss. Psychomotor retardation was reported most after health problems and least after romantic loss.
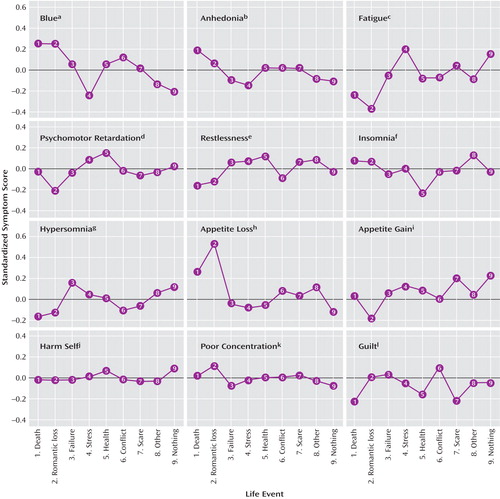
a F=17.69, p<0.001.
b F=4.68, p<0.001.
c F=17.59, p<0.001.
d F=5.37, p<0.001.
e F=3.14, p<0.001.
f F=4.01, p<0.001.
g F=4.29, p<0.001.
h F=17.82, p<0.001.
i F=3.94, p<0.001.
j F=1.04, p<0.40.
k F=1.67, p<0.10.
l F=4.36, p<0.001.
Within-Persons Analyses
To address whether the symptom pattern differences described above resulted from stable interpersonal differences rather than from the ALEs, we examined episode-specific symptom deviation data from the 1,719 individuals who experienced two or more dysphoric episodes caused by different ALE categories. The MANOVA omnibus test again indicated that depressive symptom patterns differed significantly between the ALE categories (F=3.35, df=88, 24567, p e <0.001). The mean symptom levels varied significantly across symptoms for four of the nine ALE categories ( Figure 3 ). The reactions associated with deaths, romantic losses, and chronic stress and with no precipitating cause (the “nothing” ALE category) in the within-persons sample were similar to the corresponding reactions described above for the between-persons sample. Moreover, controlling for main effects of ALE categories, the mean levels of all but four symptoms (restlessness, insomnia, trouble concentrating, and self-harm) differed significantly between the ALE categories (see Figure S1 in the data supplement that accompanies the online version of this article). As in the analysis of the between-persons sample, the mean levels of feeling blue, fatigue, and appetite loss were especially variable between ALE categories.
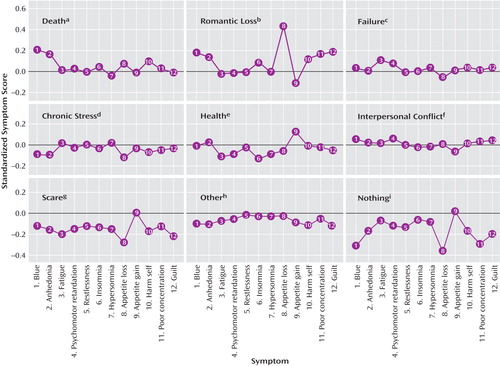
a F=3.9, p<0.001.
b F=9.58, p<0.001.
c F=0.71, p<0.73.
d F=2.85, p<0.002.
e F=1.77, p<0.06.
f F=1.23, p<0.26.
g F=1.01, p<0.45.
h F=0.8, p<0.64.
i F=4.72, p<0.001.
We also analyzed the standardized symptom scores from the within-persons sample. The MANOVA omnibus test again indicated that depressive symptom patterns differed significantly between ALE categories (F=4.73, df=88, 24567, p e <0.001). Symptom patterns were similar to those seen previously (see Figures S2 and S3 in the online data supplement).
Analyses Restricted to Those With Major Depression
Depressive symptom patterns could depend on ALE categories for dysphoric episodes but not for syndromal depression meeting DSM criteria. To evaluate this possibility, we analyzed the data from individuals who met DSM-III-R criteria for major depression. The ALE-by-symptom MANOVA again indicated that different ALE categories were associated with different patterns of depressive symptom deviations (F=2.81, df=88, 13688, p e <0.001). Symptom means varied significantly across symptoms for six of the nine ALE categories (see Figure S4 in the online data supplement), and symptom levels differed significantly between ALE categories for nine of the 12 symptoms (see Figure S5 in the online data supplement).
Consistency of Depressive Symptom Patterns Across Analyses
Table 2 presents a series of follow-up contrasts testing whether the average level of each symptom was significantly higher or lower than the average level of the other 11 symptoms within each ALE category. We performed these follow-up contrasts separately for each sample to determine whether the same symptoms were prominent or diminished in different samples. The results were highly consistent across the three samples: in only one case (insomnia associated with no precipitating cause) were the results discrepant between samples. Such consistency across samples cannot have arisen by chance (exact binomial test, p<10 –26 ).
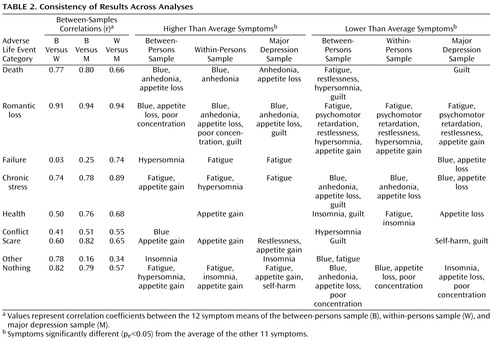
To quantify this similarity of results across samples, for each of the nine ALE categories, we correlated the 12 symptom means from one of the samples to the corresponding 12 symptom means from one of the other two samples (the first three columns of Table 2 ). All 27 resulting correlation coefficients were positive, meaning that the patterns of symptom means were similar across the three analyses for every ALE category. The average correlation coefficient between the symptom means from the between-persons sample and the symptom deviation means from the independent within-persons sample was 0.67. Likewise, the symptom means from the major depression sample were similar to those from the between-persons sample (average r=0.64) and to the symptom deviation means from the within-persons sample (average r=0.63). Finally, the results from the supplementary analysis were also similar to those from the primary analyses (see Figures S3 and S4 in the online data supplement): the means of the (nondeviation) symptom scores from the within-persons sample were positively correlated with the symptom deviation means from the within-persons sample (average r=0.75), as well as with the symptom means from both the between-persons (average r=0.51) and major depression (average r=0.74) samples.
Discussion
We sought to determine, in a population-based sample of adult twins, whether depressive symptom patterns differed according to the type of event that precipitated them. In two independent samples and a subset of individuals from both samples who met DSM-III-R criteria for major depression, the patterns of depressive symptoms consistently differed, depending on the ALE category. When symptoms followed the death of a loved one, participants reported more sadness, anhedonia, and appetite loss but less hypersomnia and guilt. The reaction following a romantic breakup was similar but not identical: participants reported sadness, appetite loss, trouble concentrating, and guilt but less fatigue, psychomotor retardation, restlessness, hypersomnia, and appetite gain. When symptoms followed chronic stress and, to a lesser degree, failures, participants reported higher fatigue, hypersomnia, and appetite gain but less sadness, anhedonia, and appetite loss. People who feared for the future reported appetite gain but little guilt. Appetite gain, fatigue, psychomotor retardation, and hypersomnia were prominent symptoms among those who indicated that nothing caused their episodes, while appetite loss, sadness, and poor concentration were not. Thoughts of self-harm were elevated for this ALE category in the between-persons sample (see Figure 2 ) but not in the within-persons sample (see Figure S1 in the online data supplement), which suggests that people who state that their dysphoria had no precipitating cause are also more likely to contemplate harming themselves.
The similarity of depressive symptom patterns from the independent within- and between-persons samples makes it highly unlikely that our findings were due to chance. Furthermore, our results were not driven by those with subthreshold depression, because similar depressive symptom patterns were found among participants who met full criteria for major depression. Our results were not due to stable interpersonal differences or to the main effects of several potential confounding variables (gender, age, current depression levels, etc.). Finally, the symptom patterns for the different ALE categories were similar for men and women and for young and old persons (results available from first author upon request).
These findings considerably extend those from two previous studies that found that ALEs are associated with different patterns of depressive symptoms (10 , 11) . The previous studies were based on data from undergraduate students who were not screened for depression and who reported on depressive symptoms during a single session. Data for the present study came from a population-based sample of adult twins of all ages who had been screened for depression and who reported on depressive symptoms across multiple time points. Despite the different samples and methodologies, the symptom profiles for the overlapping ALE categories were similar across the reports.
These results should be interpreted in the context of five potential limitations. First, the study data were from Caucasian twins born in Virginia. While similar results were found among college students at a large Midwestern university (10 , 11) , it is unknown whether these results will generalize to other populations. Second, both ALE attributions and depressive symptom levels had moderate test-retest reliability in our samples; more precise measures could increase the signal-to-noise ratio. Third, we analyzed one ALE category per episode, even though participants attributed their symptoms to multiple causes 21% of the time; more advanced statistical procedures might better elucidate the symptom patterns caused by multiple ALEs. Fourth, we did not collect information on all the symptoms that would be necessary to fully understand whether previously proposed subtypes (sociotropic depression, autonomous depression, hopelessness depression, etc.) existed in our data. Fifth, because ALE categories cannot be randomly assigned, we cannot definitively conclude that different ALEs caused different symptom profiles. However, the symptom pattern-ALE associations were similar both within and between persons, meaning that stable interpersonal differences cannot account for our findings. Moreover, previous research has shown a high correspondence between causal attributions of depressive symptoms (as analyzed here) and reports on stressful life events over the previous year collected earlier in the interview well before depressive symptoms were assessed (22) , which suggests that reporting depressive symptoms does not influence the causal attributions of the symptoms. Finally, a study in which participants were randomly assigned to visualize a major failure or the death of a loved one found symptom patterns similar to those reported here (11) . These observations cast doubt on the most likely noncausal explanations for our findings but cannot rule them out.
Conclusions
Considered alongside evidence that, after controlling for severity, there was little within-persons stability of specific depressive symptoms across episodes (7 – 9) , our results suggest that the particular presentation of depressive symptoms may have more to do with the situation than the person. Previously identified depression subtypes could be due at least in part to the fact that certain depressive symptoms tend to be more salient after specific classes of events. Furthermore, the fact that sadness and anhedonia were not prominent in the wake of several types of events raises the question of whether these symptoms should be considered core aspects of depression, as they are in the DSM classification system.
Today psychiatry tends to look for reductive explanations for the diversity of symptoms of psychiatric illness. However, as postulated long ago by Birnbaum (1) , certain aspects of clinical illness are critically affected by the psychological, environmental, or cultural context. The results of this study suggest that the depressive syndrome is flexible and environmentally responsive. This flexibility argues against reductive models that suggest that neural and molecular levels are the only ones at which we will find “true” explanations for the phenomenon of clinical depression.
1. Birnbaum K: The making of a psychosis: the principles of structural analysis in psychiatry, in Der aufbau der psychose. Berlin, Springer, 1923Google Scholar
2. Akiskal HS, McKinney WT: Depressive disorders: toward a unified hypothesis. Science 1973; 107:20–29Google Scholar
3. Eysenck HJ: The classification of depressive illness. Br J Psychiatry 1970; 24:305–319Google Scholar
4. Almasy L, Blangero J: Endophenotypes as quantitative risk factors for psychiatric disease: rationale and study design. Am J Med Genetics 2001; 105:42–44Google Scholar
5. Beck AT: Depression: Clinical, Experimental, and Theoretical Aspects. New York, Harper & Row, 1967Google Scholar
6. Abramson LY, Metalsky GI, Alloy LB: Hopelessness depression: a theory-based subtype of depression. Psychol Rev 1989; 96:358–372Google Scholar
7. Coryell W, Winokur G, Shea T, Maser JD, Endicott J, Akiskal HS: The long-term stability of depressive subtypes. Am J Psychiatry 1994; 151:199–204Google Scholar
8. Angst J, Vollrath M, Merikangas KR, Ernst C: Comorbidity of anxiety and depression in the Zurich cohort study of young adults, in Comorbidity of Mood and Anxiety Disorders. Edited by Maser JD, Cloninger CR. Washington, DC, American Psychiatric Press, 1990Google Scholar
9. Oquendo MA, Barrera A, Ellis SP, Li S, Burke AK, Grunebaum M, Endicott J, Mann JJ: Instability of symptoms in recurrent major depression: a prospective study. Am J Psychiatry 2004; 161:255–261Google Scholar
10. Keller MC, Nesse RM: Subtypes of low mood provide evidence of its adaptive significance. J Affective Disorders 2005; 86:27–35Google Scholar
11. Keller MC, Nesse RM: The evolutionary significance of depressive symptoms: different adverse situations lead to different depressive symptoms patterns. J Pers Soc Psychol 2006; 91:316–330Google Scholar
12. Kendler KS, Prescott CA: Genes, Environment, and Psychopathology: Understanding the Causes of Psychiatric and Substance Use Disorders. New York, Guilford, 2006Google Scholar
13. Prescott CA, Aggen SH, Kendler KS: Sex-specific genetic influences on the comorbidity of alcoholism and major depression in a population-based sample of US twins. Arch Gen Psychiatry 2000; 57:803–811Google Scholar
14. Judd LL, Rapaport MH, Paulus M, Brown JD: Subsyndromal symptomatic depression: a new mood disorder? J Clin Psychiatry 1994; 55(April suppl):18–28Google Scholar
15. Judd LL, Paulus MP, Wells KB, Rapaport MH: Socioeconomic burden of subsyndromal depressive symptoms and major depression in a sample of the general population. Am J Psychiatry 1996; 153:1411–1417Google Scholar
16. Derogatis LR: SCL-90-R: Administration, Scoring, and Procedures Manual, II. Towson, Md, Clinical Psychometric Research, 1983Google Scholar
17. Spitzer RL, Williams JBW: Structured Clinical Interview for DSM-III-R (SCID). New York, New York State Psychiatric Institute, Biometrics Research, 1985Google Scholar
18. Schafer JL: Analysis of Incomplete Multivariate Data. London, Chapman & Hall, 1997Google Scholar
19. Rao CR: Advanced Statistical Methods in Biometrical Research. New York, John Wiley & Sons, 1952Google Scholar
20. R Development Core Team: R: A Language and Environment for Statistical Computing, reference index version 2.2.1. Vienna, Austria, R Foundation for Statistical Computing, 2005Google Scholar
21. Tabachnick BG, Fidell LS: Using Multivariate Statistics. Needham Heights, Mass, Allyn & Bacon, 2001Google Scholar
22. Kendler KS, Karkowski LM, Prescott CA: Causal relationship between stressful life events and the onset of major depression. Am J Psychiatry 1999; 156:837–841Google Scholar

