Connectome-Based Prediction of Cocaine Abstinence
Abstract
Objective:
The authors sought to identify a brain-based predictor of cocaine abstinence by using connectome-based predictive modeling (CPM), a recently developed machine learning approach. CPM is a predictive tool and a method of identifying networks that underlie specific behaviors (“neural fingerprints”).
Methods:
Fifty-three individuals participated in neuroimaging protocols at the start of treatment for cocaine use disorder, and again at the end of 12 weeks of treatment. CPM with leave-one-out cross-validation was conducted to identify pretreatment networks that predicted abstinence (percent cocaine-negative urine samples during treatment). Networks were applied to posttreatment functional MRI data to assess changes over time and ability to predict abstinence during follow-up. The predictive ability of identified networks was then tested in a separate, heterogeneous sample of individuals who underwent scanning before treatment for cocaine use disorder (N=45).
Results:
CPM predicted abstinence during treatment, as indicated by a significant correspondence between predicted and actual abstinence values (r=0.42, df=52). Identified networks included connections within and between canonical networks implicated in cognitive/executive control (frontoparietal, medial frontal) and in reward responsiveness (subcortical, salience, motor/sensory). Connectivity strength did not change with treatment, and strength at posttreatment assessment also significantly predicted abstinence during follow-up (r=0.34, df=39). Network strength in the independent sample predicted treatment response with 64% accuracy by itself and 71% accuracy when combined with baseline cocaine use.
Conclusions:
These data demonstrate that individual differences in large-scale neural networks contribute to variability in treatment outcomes for cocaine use disorder, and they identify specific abstinence networks that may be targeted in novel interventions.
Addictions are a leading cause of disability worldwide. Despite advances in substance use treatment, the effectiveness of most interventions remains highly variable across individuals, and multiple quit attempts are common. While a growing body of research suggests that variability in treatment response is linked to individual differences in neural functioning (1–6), the search for brain-based predictors has yet to yield a reliable indicator of future treatment response or abstinence (7, 8). Identification of brain-based predictors of abstinence not only may expand existing biological knowledge of addiction pathophysiology (which may itself be used to refine existing interventions) but also may ultimately be used to directly inform real-world clinical practice by assignment of patients to therapies based on individual patterns of neural function, or neuromarkers (7, 9, 10).
In most cases, treatment-oriented neuroimaging studies in addiction and other disorders rely on prospective associations (1–4), where the term “predict” is often used inaccurately to refer to correlation or regression (11, 12). True predictive models, however, require application of the model to novel data (8, 11, 13–15). Newly available alternatives, such as machine learning, allow for actual prediction (9, 11, 12) but have not yet been used to identify pretreatment predictors of abstinence. Nonetheless, research indicates that alterations within well-established neural networks (e.g., frontoparietal, salience, default mode) likely contribute to individual differences in treatment outcomes for cocaine use disorder (3, 5, 16). For example, functional connectivity strength between the medial prefrontal cortex and the temporal pole, when combined with years of education, has been identified as a predictor of relapse (5). However, no previous study has used a whole-brain, machine learning approach to identify neuromarkers of future abstinence.
Connectome-based predictive modeling (CPM) (13, 17) is a machine learning approach for generating brain-behavior models from whole-brain functional connectivity data (“connectomes”). Unlike correlation or regression models, CPM with built-in cross-validation protects against overfitting by testing the strength of the relationship in a novel sample, increasing the likelihood of replication in future studies and thus applicability to other clinical samples (13). Unlike the machine learning approaches that have previously been used to study addictions, CPM is entirely data driven and requires no a priori selection of networks. It is therefore both a predictive tool and a method of identifying networks that subserve specific behaviors—referred to as “neural fingerprints”—and thus it may also be used to identify novel treatment targets (13, 17). CPM has previously been used to identify neural fingerprints of IQ and attention using whole-brain functional connectivity data acquired during neurocognitive task performance (17–19), but it has not previously been used to predict future behaviors or a clinical outcome.
In this study, we used dimensional CPM to identify neural networks predictive of future abstinence from cocaine by applying CPM to functional MRI (fMRI) reward task data acquired at the start of a 12-week treatment for cocaine use disorder. We further tested the stability of these networks over time and in relation to posttreatment abstinence. Finally, we tested the ability of identified networks to predict treatment response in a heterogeneous replication sample. Based on previous work focusing on selected networks (5, 16), we hypothesized that increased connectivity within and between medial frontal, frontoparietal, and salience networks would positively predict abstinence.
Methods
Participants and Recruitment
Participants (N=74) were recruited from a randomized controlled trial of behavioral therapy plus galantamine or placebo treatment for cocaine use disorder (20). Demographic and clinical characteristics are summarized in Table 1. In addition to seeking treatment for cocaine, all participants were currently enrolled in methadone maintenance treatment for opioid use disorder. Consistent with the parent trial (20), the fMRI sample was predominantly male (63.5%) and unemployed (73.0%), with multiple previous treatment attempts (a mean of 2.97 outpatient treatments [SD=3.63] and 3.16 inpatient treatments [SD=5.24]) and legal problems (a mean of 5.46 lifetime arrests [SD=6.29]). After exclusion of individuals with incomplete data (N=4) or excessive motion during scanning (N=17; further details below), the final sample used for CPM analyses consisted of 53 individuals (73.6% male). Further details on motion controls and follow-up analyses controlling for time of scanning are provided in the online supplement. As shown in Table 1, included and excluded participants did not differ significantly in years of cocaine use, treatment assignment, or other clinical variables, with the exception of sex (p=0.004). As in our previous work (2, 4), abstinence during treatment was assessed with biweekly urine testing and was defined in terms of the percentage of urine samples provided during the treatment period that were negative for cocaine. All participants provided written informed consent after receiving a complete description of the study procedures.
| fMRI Data Included in CPMb | ||||||
|---|---|---|---|---|---|---|
| Variable | Total (N=74) | Yes (N=53) | No (N=21) | |||
| N | % | N | % | N | % | |
| Female | 27 | 36.5 | 14 | 26.4 | 13 | 61.9 |
| Completed high school | 53 | 71.6 | 37 | 69.8 | 16 | 76.2 |
| Unemployed | 54 | 73.0 | 36 | 71.7 | 16 | 76.2 |
| Mean | SD | Mean | SD | Mean | SD | |
| Methadone dosage at baseline (mg/day) | 73.0 | 24.4 | 74.7 | 23.1 | 69.0 | 27.5 |
| Days in treatment at fMRI scan | 1.9 | 7.3 | 1.5 | 6.7 | 2.9 | 8.6 |
| Age (years) | 36.3 | 9.4 | 35.2 | 9.4 | 39.3 | 9.1 |
| Days of opioid use, past 28 days | 3.6 | 5.8 | 3.8 | 6.1 | 3.1 | 5.0 |
| Days of marijuana use, past 28 days | 2.0 | 5.5 | 1.9 | 5.9 | 2.2 | 4.2 |
| Days of cocaine use, past 28 days | 16.2 | 8.1 | 16.9 | 8.3 | 14.5 | 7.4 |
| Days of cigarette use, past 28 days | 26.1 | 6.6 | 25.6 | 7.6 | 27.4 | 2.8 |
| Days of alcohol use, past 28 days | 2.4 | 5.9 | 2.1 | 5.1 | 3.2 | 7.7 |
| Years of regular cocaine use | 9.0 | 7.8 | 8.1 | 6.5 | 11.3 | 10.2 |
| Number of previous outpatient drug treatments | 3.0 | 3.6 | 3.0 | 3.8 | 2.9 | 3.4 |
| Number of previous inpatient drug treatments | 3.2 | 5.2 | 3.0 | 4.7 | 3.6 | 6.6 |
| Lifetime number of arrests | 5.5 | 6.3 | 5.3 | 6.1 | 5.8 | 6.9 |
| Estimated IQ | 90.5 | 12.8 | 90.1 | 12.8 | 91.2 | 13.2 |
| Percent cocaine-negative urine samples | 21.6 | 28.9 | 23.0 | 28.0 | 18.0 | 31.5 |
| N | % | N | % | N | % | |
| Route of cocaine use | ||||||
| Smoking | 52 | 70.3 | 37 | 69.8 | 15 | 71.4 |
| Snorting | 15 | 20.3 | 11 | 20.8 | 4 | 19.0 |
| Intravenous | 7 | 9.5 | 5 | 9.4 | 2 | 9.5 |
TABLE 1. Demographic and clinical characteristics of methadone-maintained, cocaine-dependent participants in a connectome-based predictive modeling (CPM) study (N=74)a
Neuroimaging Data Acquisition
fMRI data were acquired during performance of a well-validated monetary incentive delay task (21) (see the online supplement, including Figure S1). Preprocessing was conducted using SPM8 and the BioImage Suite and is described in the online supplement.
Functional Connectivity
Whole-brain functional connectivity analyses were conducted using the BioImage suite, using previously described methods (17–19). Network nodes were defined using the Shen 268-node brain atlas, which includes the cortex, subcortex, and cerebellum (22), as in previous CPM work (17–19) (further details are provided in the online supplement). Task connectivity was calculated on the basis of the “raw” task time courses, with no regression of task-evoked activity (18, 23). This involved computation of mean time courses for each of the 268 nodes (i.e., average time course of voxels within the node) for use in node-by-node pairwise Pearson’s correlations. The resultant r values were transformed using Fisher’s z-transformation to create symmetric 268×268 connectivity matrices in which each element of the matrix represents the strength of connection between two individual nodes (hereafter referred to as an “edge”) (13, 19).
Connectome-Based Predictive Modeling (CPM)
CPM was conducted using previously validated custom MATLAB scripts (13). A schematic diagram of CPM is presented in Figure S2 in the online supplement. Briefly, CPM takes group connectivity matrices and behavioral data (in this case, percentage of cocaine-negative urine samples during treatment) as input to generate a predictive model of the behavioral data from connectivity matrices (13). Edges and behavioral data from the training data set are correlated using regression analyses (here using either Pearson’s correlation or partial correlation) to identify positive and negative predictive networks. Positive networks are networks for which increased edge weights (increased connectivity) are associated with the variable of interest, and negative networks are those for which decreased edge weights (decreased connectivity) are associated with the variable of interest. While both networks are used for predicting the same variable, they are by definition independent, because a single edge cannot be both a positive and a negative predictor. Single-subject summary statistics are then created as the sum of the significant edge weights in each network and are entered into predictive models that assume linear relationships with behavioral data. The resultant polynomial coefficients (linear equation including slope and intercept) are then applied to the test data set to predict behaviors. In the case of leave-one-out cross-validation (used here), a single participant’s predicted value (i.e., the “left-out” participant) is generated by taking the data from all other participants as the training data set in an iterative manner until all participants have a predicted value.
Model performance (i.e., correspondence between predicted and actual values) was assessed using Spearman’s rho correlations. When using leave-one-out cross-validation, analyses in the leave-one-out folds are not wholly independent, and the number of degrees of freedom is thus overestimated for parametric p values based on correlation. Instead of parametric testing, we therefore performed permutation testing. To generate null distributions for significance testing, we randomly shuffled the correspondence between behavioral variables and connectivity matrices 5,000 times and reran the CPM analysis with the shuffled data. Based on these null distributions, the p values for leave-one-out predictions were calculated as in previous work (13, 18). Details on characterization of the resultant network anatomy are provided in the online supplement.
Results
Associations Between Baseline Variables and Abstinence
Spearman’s correlation analyses indicated no significant associations between baseline clinical variables (years of use, past-month use, methadone dosage) and within-treatment abstinence (p values, >0.05). For comparison with CPM findings, a machine learning analysis (i.e., support vector regression [SVR]) of baseline clinical data was also conducted (details are provided in the online supplement). Because CPM is optimized for neuroimaging data, SVR was selected over CPM for this analysis. SVR incorporating baseline clinical variables did not predict within-treatment abstinence (p>0.05).
Predicting Within-Treatment Abstinence
To control for putative effects of residual motion, CPM analyses were conducted both with and without motion as a covariate, and the two approaches yielded similar results (further details are provided in the online supplement). For simplicity, findings including motion as a covariate are presented here unless otherwise specified. The overall CPM model successfully predicted abstinence (as indicated by cocaine-negative urine samples) (combined positive and negative networks: r=0.42, df=52, p=0.001) (Figure 1), as did connectivity within the positive (r=0.43, df=52, p<0.001) and negative (r=0.40, df=52, p=0.003) networks separately.

FIGURE 1. Connectome-based predictive modeling (CPM) performance and positive and negative abstinence networksa
a Panel A shows positive (red) and negative (blue) abstinence networks. For the positive network, increased edge weights (i.e., increased functional connectivity) predict more within-treatment abstinence. For the negative network, decreased edge weights (i.e., decreased functional connectivity) predict more within-treatment abstinence. Larger spheres indicate nodes with more edges, and smaller spheres indicate fewer edges. Panel B illustrates the correspondence between actual (x-axis) and predicted (y-axis) abstinence values generated using CPM. Abstinence values correspond to the percentage of urine samples provided during treatment that were negative for cocaine. Despite the clinical complexity of the population, CPM successfully predicted within-treatment abstinence (p values, <0.005). Predictions remained significant in follow-up analyses controlling for clinical variables, including years of cocaine use and treatment retention (see the online supplement).
Follow-up comparisons controlling for methadone dosage, medication group (galantamine or placebo), cocaine use history (years of use, days of past-month use), other drug and alcohol use, smoking status, and timing of fMRI scanning with respect to treatment initiation also successfully predicted abstinence (r values >0.40, with p values <0.003) and are presented in the online supplement. Post hoc correlations indicated significant correspondence between network strengths and other abstinence indices (e.g., percent days self-reported abstinence, maximum days of consecutive abstinence) and are presented in the online supplement.
Network Anatomy
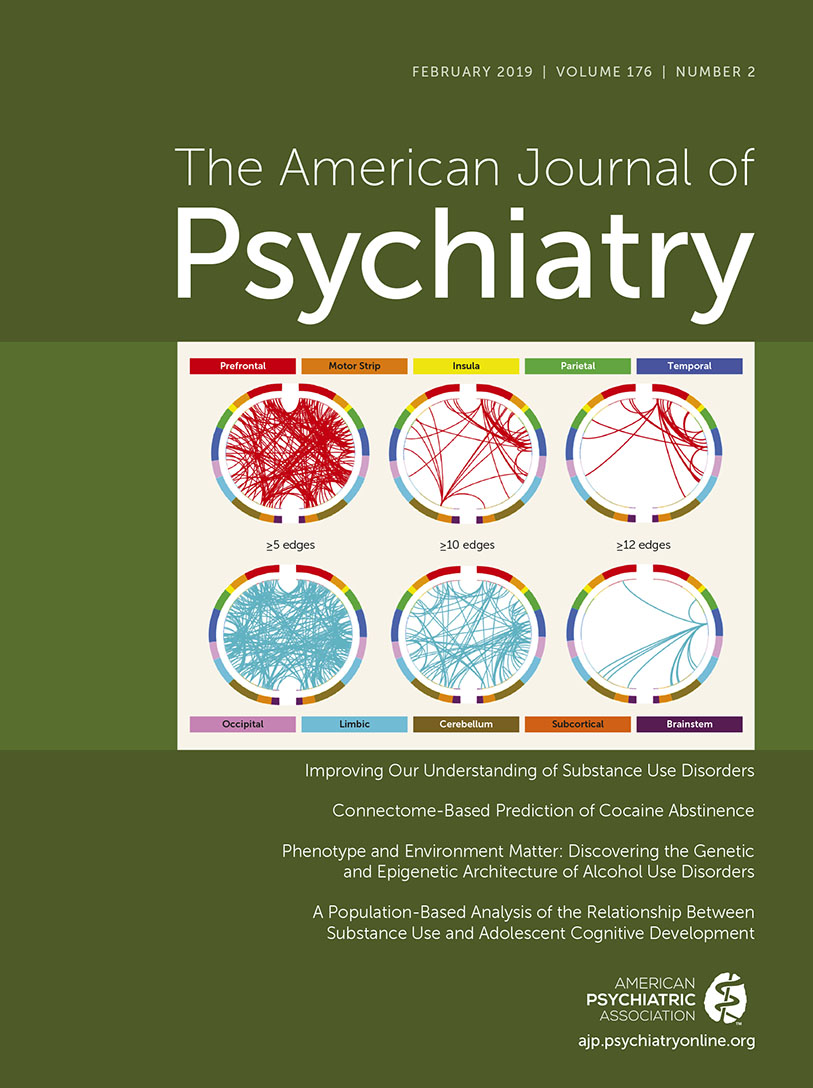
Figure 2 summarizes positive and negative abstinence networks based on connectivity between macroscale brain regions (note that brain regions are presented in approximate anatomical order, such that longer-range connections are represented by longer lines). Consistent with previous CPM work (17–19), network anatomies for both networks were complex and included connections between frontal, parietal, occipital, and temporal lobes. Despite this complexity, the spatial extent of both positive and negative networks together included only 529 edges (266 positive, 263 negative), or less than 1.5% of possible connections. Highest-degree nodes (i.e., nodes with the most connections) for the positive network included a prefrontal node with connections to limbic, temporal, parietal, cerebellar, and other prefrontal nodes, and a temporal node with connections to limbic, parietal, motor, and prefrontal nodes. Highest-degree nodes for the negative network also included a temporal node with connections to limbic, parietal, and prefrontal nodes as well as with connections to cerebellar and subcortical nodes. Both abstinence networks included short- and long-range connections. However, the positive network was characterized by relatively more long-range connections (56% long-range; 44% short-range), whereas the negative network included more short-range connections (42% long-range; 58% short-range).

FIGURE 2. Positive and negative abstinence networks summarized by connectivity between macroscale brain regionsa
a From the top, brain regions are presented in approximate anatomical order, such that longer-range connections are represented by longer lines.
Overlap With Canonical Neural Networks
To facilitate characterization of identified abstinence networks, Figure 3 summarizes connectivity based on the number of connections within and between canonical neural networks (e.g., frontoparietal, motor/sensory) for the positive (Figure 3A) and negative (Figure 3B) networks. By definition, positive and negative networks do not contain overlapping connections (as a single edge cannot be both a positive and a negative predictor). However, positive and negative abstinence networks included connections within and between similar large-scale canonical neural networks. Comparison of networks (Figure 3C) indicated that the positive network included relatively more connections between medial frontal and frontoparietal and default mode networks; between motor/sensory and cerebellar and salience networks; and between subcortical and motor/sensory and salience networks. The negative network included relatively more connections between medial frontal and salience networks; between medial frontal and subcortical networks; between medial frontal and motor/sensory networks; between default mode and salience networks; and between frontoparietal and motor/sensory networks. The positive network was further characterized by more within-network connections across medial frontal, frontoparietal, default mode, motor/sensory, visual association, and salience networks, whereas the negative network included more within-network connections for occipital and subcortical networks.

FIGURE 3. Positive and negative abstinence networks summarized by overlap with canonical neural networksa
a Within- and between-network connectivity for the positive network (panel A), for the negative network (panel B) and for the positive minus the negative network (panel C) are summarized based on overlap with canonical neural networks. In panels A and B, cells represent the total number of edges connecting nodes within (and between) each network, with darker colors indicating a greater number of edges. In panel C, cells represent the number of positive versus negative edges connecting nodes within (and between) each network, with warmer colors (orange and yellow) indicating more edges in the positive network and cooler colors (blue and green) indicating more edges in the negative network. Despite this visual simplification, it is important to note that, by definition, positive and negative networks do not contain overlapping edges. (For further details on network definitions, see Figure S3 in the online supplement.)
Relationship to Posttreatment Abstinence
Trial participants were also invited to participate in posttreatment fMRI scanning. After exclusion for excess motion (as described above), 40 participants who underwent posttreatment fMRI scanning were included in the analyses. To determine the extension of our networks to predict abstinence after treatment, individual participant network summary scores were created as the sum of connectivity strengths within positive and negative networks (negative network values were first sign-flipped so that higher values indicated “better” networks). The resultant scores from posttreatment matrices were entered into correlation analyses with abstinence during 6-month follow-up (as defined by self-report using the timeline follow-back method, assessed monthly). Posttreatment connectivity strengths were significantly associated with abstinence during follow-up (r=0.34, df=39, p=0.03). Comparison of pre- and posttreatment networks indicated no significant changes in connectivity strength (t=0.81, df=38, p=0.42).
Out-of-Sample Replication and Binary Prediction
To determine the generalizability of our findings, we tested the ability of the identified networks to predict cocaine-negative urine toxicology outcomes in a heterogeneous sample of cocaine-dependent individuals (N=45). This included previously excluded individuals with excess motion during scanning (N=17) and individuals from an independent, previously published randomized controlled trial (N=28) (2). As in our original analyses, residual motion was included as a covariate. Further details on exclusion for motion and related analyses are provided in the online supplement.
Because the practical clinical utility of biomarkers is unlikely to rely on their ability to generate continuous indices of treatment outcome but rather on their ability to identify, a priori, treatment responders from nonresponders in a binary manner, we further tested the ability of the identified networks to predict abstinence in a binary manner (any drug-free urine specimens, yes/no) in our replication sample. Individual participant summary scores were extracted from functional connectivity matrices, as above, and entered into regression analyses with within-treatment abstinence values.
Pretreatment network strength in the independent sample predicted abstinence during treatment for both continuous outcomes (percent cocaine-negative urine samples during treatment; r=0.36, df=44, p=0.016) and binary outcomes (any cocaine-negative urine; 64% accuracy, χ2=5.99, df=2, p=0.014; 82% specificity; 35% sensitivity). For binary prediction, accuracy was increased to 71% after inclusion of baseline cocaine use (days of use in the month preceding treatment) in the model (χ2=6.20, df=2, p=0.02; 89% sensitivity; 41% specificity). As shown in Figure S4 in the online supplement, binarization across different levels of use (≥25% drug-free urine samples, ≥75% drug-free urine samples) decreased sensitivity (57% and 25%, respectively) but increased specificity (71% and 89%, respectively).
Discussion
The translation of brain imaging findings into real-world clinical settings is one of the primary challenges of modern neuropsychiatry (7–9, 11–13). In this study, we demonstrated the ability of a recently developed connectome-based machine learning approach to predict treatment outcomes (abstinence from cocaine during 12-week treatment) using baseline patterns of connectivity. We further demonstrated that posttreatment patterns of connectivity within these networks predicted abstinence during 6-month follow-up. Finally, we demonstrated that the same networks can be used to predict treatment response in an independent, heterogeneous sample. Despite this predictive ability, identified networks could be considered potential treatment targets (3, 5, 16), and further replication and model refinement are needed before the findings can be directly applied to clinical decision making.
Consistent with the connectome-based approach, abstinence networks were complex and included connections between multiple well-established neural networks (17, 18). The positive network included more frontoparietal–medial frontal–default mode connections as well as more salience–subcortical–motor/sensory connections. In contrast, the negative network (the network for which increased connectivity is negatively associated with abstinence) included more connections between the medial frontal network and salience, subcortical, and motor/sensory networks as well as more salience–default mode connections. Based on these findings, Figure 4 presents a theoretical network model of abstinence. We propose that abstinence is positively predicted by 1) integration of a cognitive/executive control system involving increased connectivity between frontoparietal and medial frontal networks; 2) integration of a reward responsiveness system involving increased connectivity between salience, motor/sensory, and subcortical networks; and 3) segregation (decreased connectivity) between these two systems. This model builds on previous models of addiction emphasizing separation of frontoparietal and salience networks (24, 25) but also incorporates medial frontal, motor/sensory, and subcortical networks to provide a theoretical framework for future research.

FIGURE 4. Five-network model of abstinence during substance use treatmenta
a Large-scale patterns of between-network connectivity for abstinence networks identified using connectome-based predictive modeling are summarized based on relative number of connections within positive (red) versus negative (blue) networks. Stronger connectivity (i.e., network integration) between frontoparietal and medial-frontal networks (top) and between sensory-motor, salience, and subcortical networks (bottom) positively predicted within-treatment abstinence. Weaker connectivity between these two systems (i.e., network segregation) also predicted more within-treatment abstinence.
Within the above context, cognitive/executive control networks are theorized to contribute to abstinence via coordination of top-down processes necessary for treatment engagement (e.g., acquisition of new skills, enhanced control over impulsive behavior), whereas integration of reward networks may support motivational processes relevant to treatment (e.g., willingness to change, attending to alternate rewards) (3, 26). In addition, based on previous resting-state research in cocaine use disorder (27), appropriate separation between these two systems is theorized to relate to greater behavioral flexibility (or to decreased compulsivity), as would be required for behavior change during treatment.
Although we did not model specific events of interest but rather used “raw” time courses, our findings are nonetheless intuitive when considered within the context of reward task performance, which requires coordination of both attentional and cognitive control processes as well as of salience encoding and reward response behaviors (28, 29). These findings are further consistent with recent data prospectively linking medial prefrontal, frontoparietal, and salience networks to cocaine relapse (5, 16), as well as with data from activation-based studies linking individual differences in brain reward responses to treatment outcomes in addiction (2, 6, 30). They further suggest that segregation of executive control/attention and salience/reward response systems within the context of performance on the monetary incentive delay task may be optimal for achieving abstinence from cocaine. More generally, these data add to emerging evidence that manipulation of brain states (e.g., via reward task performance) may be helpful in detecting individual differences in brain-behavior relationships (23). For example, connectome-based predictive models derived from task-based data have consistently outperformed those derived from resting-state data in nonaddicted populations (31). However, further work across different brain states and in relation to diverse substance use behaviors is needed to test this hypothesis in the specific context of addictions.
Connectivity strength within abstinence networks did not differ between pre- and posttreatment assessments. Previous activation-based studies have demonstrated changes in neural responses after substance use treatments; however, comparatively little is known about network-level changes with treatment. For example, individual differences in connectivity have been found to predict subsequent relapse to cocaine (5, 16, 32), yet no previous study has compared connectivity before and after treatment for cocaine use disorder. Our findings suggest relative stability of identified networks over 12-week treatment, raising the possibility that abstinence may be more closely linked to pretreatment neural function than to within-treatment neuroplasticity. In this context, it is possible that pretreatment interventions influencing connectivity within the identified networks (e.g., cognitive training, targeted pharmacotherapies) may be helpful in promoting abstinence during treatment (33–36). For example, previous CPM work has demonstrated that connectivity strength within networks predictive of attention deficit hyperactivity disorder symptoms is changed after administration of methylphenidate (19). Thus, it is possible that effective treatments for addiction also influence connectivity within complex networks.
It is further possible that networks contributing to treatment response are distinct from those that are directly implicated in disease pathology or that change with treatment. Brain regions predictive of treatment response in other disorders often have limited overlap with regions consistently found to differentiate patients from control subjects (37). Clinically, factors that predict treatment response (e.g., motivation to change) may be distinct from those that change with treatment (e.g., acquisition of new skills). Thus, the same may be true for neural networks. Furthermore, it is possible that changes within abstinence networks may take time to emerge and thus may be detectable only after treatment, as would be consistent with data indicating protracted emergence of treatment effects (38). Additional work is therefore needed to characterize network-level changes over time and in relation to addiction pathology per se. Similarly, future studies should consider how “positive” and “negative” networks change over the course of treatment.
While continuous prediction approaches, which maximize individual differences, are optimal for feature selection in heterogeneous clinical samples (11), the practical value of predictive modeling within a clinical context will likely involve binary prediction (e.g., identifying treatment responders and nonresponders). We therefore tested the ability of the identified networks to predict categorical outcomes (cocaine-negative urine samples, yes/no) as well as to predict dimensional (percent cocaine-negative urine samples) within-treatment abstinence in an independent, heterogeneous sample of individuals with cocaine use disorder with and without concurrent methadone treatment. Connectivity within the identified networks successfully predicted both categorical and dimensional treatment response in our replication sample.
In our replication sample, our model had high sensitivity but low specificity. In this instance, low sensitivity would translate to underidentification of responders (and thus underassignment of individuals to effective treatment), whereas low specificity would translate to underidentification of nonresponders (overassignment to ineffective treatment). Given that multiple failed treatment attempts are common in addictions—and that only resources are lost in the instance of overassignment to ineffective treatment—maximizing sensitivity in this instance appears paramount.
Strengths and Limitations
This study has several strengths, including use of a recently developed whole-brain predictive modeling approach, multiple-time-point fMRI data (before and after treatment), and out-of-sample replication. Several limitations should be noted, too. Some participants were excluded for missing data or excess motion during scanning, resulting in a relatively modest sample size for our primary analysis (N=53); thus, further work in larger samples is warranted, as noted above. Second, the functional significance of the identified networks in relation to other aspects of substance use pathology remains to be determined. While networks were relatively robust and not significantly changed in follow-up analyses controlling for other factors, we cannot entirely exclude the effects of other clinical variables, such as concurrent use of other substances or even acute intoxication, on connectivity strength. Third, given the relatively limited temporal specificity of urine toxicology analyses, future studies should consider incorporation of salivary testing for acute drug effects. Fourth, further work will be needed to determine generalizability of these findings to fMRI data acquired during performance of different tasks or while the brain is “at rest.” To avoid circularity, we did not test the ability of pretreatment data to predict abstinence during follow-up; however, this will be an important next step for future studies (5). Consistent with recommendations to encourage model testing in diverse samples (39), we have made the positive and negative abstinence network masks publicly available at our web site (https://www.nitrc.org/projects/bioimagesuite/).
Identified networks accounted for just under 20% of the variance in within-treatment abstinence for novel subjects. While arguably somewhat modest, it is important to note that effect size estimates derived from “traditional” statistical approaches—that is, statistics applied to test explanatory hypotheses—are typically larger than those derived from machine learning approaches—that is, statistics applied to predict unknown information (17, 40). Predictive models are less likely to overfit a specific data set, leading to both increased likelihood of out-of-sample replication as well as typically decreased (more realistic) effect size estimates (12, 41, 42). Similarly, small effect sizes are found in mega-analyses with ∼10,000 subjects (e.g., findings from the ENIGMA project).
Conclusions
This study demonstrates that baseline patterns of whole-brain connectivity can predict a complex clinical outcome—in this case, cocaine abstinence. Consistent with the parent randomized controlled trial (20), participants had significant addiction histories, including multiple previous quit attempts, legal problems, and concurrent methadone treatment for opioid use disorder. Despite this clinically complex profile, baseline connectivity within the identified networks successfully predicted within-treatment abstinence, even after controlling for other baseline variables, including other drug use history and treatment assignment.
The predictive ability of these networks translated to a separate, heterogeneous sample of individuals (including non–methadone-maintained individuals with cocaine use disorder who underwent scanning before enrollment in a different treatment trial). These data demonstrate that individual differences in connectivity within large-scale neural networks implicated in cognitive/executive control and reward responsiveness processes contribute to variability in cocaine use outcomes. As such, these “neural fingerprints” may be an appropriate target for future intervention efforts.
1 : Individual differences in anterior cingulate activation associated with attentional bias predict cocaine use after treatment. Neuropsychopharmacology 2013; 38:1085–1093Crossref, Medline, Google Scholar
2 : Neurofunctional reward processing changes in cocaine dependence during recovery. Neuropsychopharmacology 2016; 41:2112–2121Crossref, Medline, Google Scholar
3 : Functional brain networks associated with cognitive control, cocaine dependence, and treatment outcome. Psychol Addict Behav 2013; 27:477–488Crossref, Medline, Google Scholar
4 : Anticipatory reward processing among cocaine-dependent individuals with and without concurrent methadone-maintenance treatment: relationship to treatment response. Drug Alcohol Depend 2016; 166:134–142Crossref, Medline, Google Scholar
5 : Salience and default mode network dysregulation in chronic cocaine users predict treatment outcome. Brain 2017; 140:1513–1524Crossref, Medline, Google Scholar
6 : Toward biomarkers of the addicted human brain: using neuroimaging to predict relapse and sustained abstinence in substance use disorder. Prog Neuropsychopharmacol Biol Psychiatry 2018; 80(Pt B):143–154Crossref, Medline, Google Scholar
7 : An overview of translational approaches to the treatment of addictions, in Neuroimaging and Psychosocial Addiction Treatment: An Integrative Guide for Researchers and Clinicians. Edited by Feldstein Ewing S, Witkiewitz K, Filbey F. New York, Palgrave, 2015Crossref, Google Scholar
8 : The neurobiology of successful abstinence. Curr Opin Neurobiol 2013; 23:668–674Crossref, Medline, Google Scholar
9 : Brain connectomics predict response to treatment in social anxiety disorder. Mol Psychiatry 2016; 21:680–685Crossref, Medline, Google Scholar
10 : Brain mechanisms of change in addictions treatment: models, methods, and emerging findings. Curr Addict Rep 2016; 3:332–342Crossref, Medline, Google Scholar
11 : Prediction as a humanitarian and pragmatic contribution from human cognitive neuroscience. Neuron 2015; 85:11–26Crossref, Medline, Google Scholar
12 : When optimism hurts: inflated predictions in psychiatric neuroimaging. Biol Psychiatry 2014; 75:746–748Crossref, Medline, Google Scholar
13 : Using connectome-based predictive modeling to predict individual behavior from brain connectivity. Nat Protoc 2017; 12:506–518Crossref, Medline, Google Scholar
14 : Puzzlingly high correlations in fMRI studies of emotion, personality, and social cognition. Perspect Psychol Sci 2009; 4:274–290Crossref, Medline, Google Scholar
15 : The potential of neuroimaging for identifying predictors of adolescent alcohol use initiation and misuse. Addiction 2017; 112:719–726Crossref, Medline, Google Scholar
16 : Executive control network connectivity strength protects against relapse to cocaine use. Addict Biol 2017; 22:1790–1801Crossref, Medline, Google Scholar
17 : Functional connectome fingerprinting: identifying individuals using patterns of brain connectivity. Nat Neurosci 2015; 18:1664–1671Crossref, Medline, Google Scholar
18 : A neuromarker of sustained attention from whole-brain functional connectivity. Nat Neurosci 2016; 19:165–171Crossref, Medline, Google Scholar
19 : Methylphenidate modulates functional network connectivity to enhance attention. J Neurosci 2016; 36:9547–9557Crossref, Medline, Google Scholar
20 : Galantamine and computerized cognitive behavioral therapy for cocaine dependence: a randomized clinical trial. J Clin Psychiatry 2018; 79:17m11669 (doi: 10.4088/JCP.17m11669)Crossref, Medline, Google Scholar
21 : Individuals family history positive for alcoholism show functional magnetic resonance imaging differences in reward sensitivity that are related to impulsivity factors. Biol Psychiatry 2011; 69:675–683Crossref, Medline, Google Scholar
22 : Groupwise whole-brain parcellation from resting-state fMRI data for network node identification. Neuroimage 2013; 82:403–415Crossref, Medline, Google Scholar
23 : Can brain state be manipulated to emphasize individual differences in functional connectivity? Neuroimage 2017; 160:140–151Crossref, Medline, Google Scholar
24 : Resting state functional connectivity in addiction: lessons learned and a road ahead. Neuroimage 2012; 62:2281–2295Crossref, Medline, Google Scholar
25 : Resting state functional connectivity analysis for addiction medicine: from individual loci to complex networks, in Brain Research. Edited by Ekhtiari H, Martin P. Amsterdam, Elsevier, 2016, pp 155–173. in Progress.Google Scholar
26 : Behavioral therapies: the glass would be half full if only we had a glass, in Rethinking Substance Abuse: What the Science Shows, and What We Should Do About It. Edited by Miller W, Carroll K. New York, Guilford, 2006, pp 223–239Google Scholar
27 : Impaired functional connectivity within and between frontostriatal circuits and its association with compulsive drug use and trait impulsivity in cocaine addiction. JAMA Psychiatry 2015; 72:584–592Crossref, Medline, Google Scholar
28 : Anticipatory reward processing in addicted populations: a focus on the monetary incentive delay task. Biol Psychiatry 2015; 77:434–444Crossref, Medline, Google Scholar
29 : Dissociation of reward anticipation and outcome with event-related fMRI. Neuroreport 2001; 12:3683–3687Crossref, Medline, Google Scholar
30 : Enhanced midbrain response at 6-month follow-up in cocaine addiction, association with reduced drug-related choice. Addict Biol 2012; 17:1013–1025Crossref, Medline, Google Scholar
31 : Task-induced brain state manipulation improves prediction of individual traits. Nat Commun 2018; 9:2807Crossref, Medline, Google Scholar
32 : Cortico-amygdala coupling as a marker of early relapse risk in cocaine-addicted individuals. Front Psychiatry 2014; 5:16Crossref, Medline, Google Scholar
33 : Effects of chronic and acute stimulants on brain functional connectivity hubs. Brain Res 2015; 1628(Pt A):147–156Crossref, Medline, Google Scholar
34 : Cognitive enhancement as a treatment for drug addictions. Neuropharmacology 2013; 64:452–463Crossref, Medline, Google Scholar
35 : Performance-based contingency management in cognitive remediation training: a pilot study. J Subst Abuse Treat 2017; 72:80–88Crossref, Medline, Google Scholar
36 : Remember the future: working memory training decreases delay discounting among stimulant addicts. Biol Psychiatry 2011; 69:260–265Crossref, Medline, Google Scholar
37 : Predicting treatment response in social anxiety disorder from functional magnetic resonance imaging. JAMA Psychiatry 2013; 70:87–97Crossref, Medline, Google Scholar
38 : One-year follow-up of disulfiram and psychotherapy for cocaine-alcohol users: sustained effects of treatment. Addiction 2000; 95:1335–1349Crossref, Medline, Google Scholar
39 : Building better biomarkers: brain models in translational neuroimaging. Nat Neurosci 2017; 20:365–377Crossref, Medline, Google Scholar
40 : To explain or to predict? Stat Sci 2010; 25:289–310Crossref, Google Scholar
41 : Choosing prediction over explanation in psychology: lessons from machine learning. Perspect Psychol Sci 2017; 12:1100–1122Crossref, Medline, Google Scholar
42 : The relation between statistical power and inference in fMRI. PLoS One 2017; 12:e0184923Crossref, Medline, Google Scholar